Abstract
Background
The purpose of this study was to evaluate the usefulness of hook wire localization biopsy under imaging guidance for nonpalpable breast lesions detected radiologically.
Methods
This was a descriptive study conducted at the Department of Radiology, Aga Khan University Hospital, Karachi. All patients undergoing needle localization biopsy of a nonpalpable breast lesion under mammographic or ultrasound guidance between January 2009 to December 2010 were included in the study. Patients with incomplete medical records were excluded. All patients’ mammograms or ultrasound were categorized using BI-RADS® assessment categories. The percentages of benign and malignant lesions were determined by pathological examination of surgically removed specimens. A correlation was sought between preoperative imaging assessment and the final diagnosis. The complications associated with the procedure were also recorded.
Results
A total of 151 biopsies were carried out, of which 80 were performed under mammographic guidance and 71 were performed under ultrasound guidance. The mean age of the patients was 51.89 years. The overall malignancy rate was 25.16%. Of 93 cases reported radiologically as malignant, 60 turned out to be malignant, and of the 58 cases reported as benign on imaging, three proved to be malignant on histopathology. The sensitivity of imaging findings was 95% and the specificity was 62%. The malignancy rate was 5% for benign lesions and 64% for malignant lesions, respectively. There were no complications related to wire localization, and only two patients had minor complications following surgical excision, giving a complication rate of 1.32%.
Conclusion
Hook wire localization biopsy is a safe and effective procedure for definitive diagnosis of suspicious lesions on imaging, and is more helpful if the imaging findings are suspicious.
Introduction
Breast cancer is the second leading cause of death among women in the United States.Citation1 The increasing use of mammography and increased awareness of breast cancer among women has resulted in early detection of localized breast cancer. This has led to marked improvement in the cure rate for the disease, which is rapidly increasing in incidence. The benefits of screening mammography have been documented in a number of studies, including the Breast Cancer Detection Demonstration Project and Health Insurance Plan of New York.Citation2,Citation3 The sensitivity of mammography for detection of breast cancer is variable, and 9%–63% of all abnormalities reported on mammograms are ultimately diagnosed as malignant.Citation4–Citation6 Needle localization followed by open surgical biopsy was introduced in 1965 as a way of obtaining a histological diagnosis of such lesions. This technique involves placement of a radiopaque wire percutaneously into or near the lesion either under ultrasound or mammography guidance preoperatively by a radiologist. The exact position of the wire relative to the lesion either placed under ultrasound or mammographic guidance is verified by a mammogram. The wire and mammogram guides the surgeon to the exact site of the lesion and avoids unnecessary removal of a large volume of tissue in the event of a benign lesion. On the other hand, it is important to obtain a wide tumor-free resection margin if the lesion turns out to be malignant on histopathology. Preoperative needle localization offers an opportunity to make a rapid and accurate excision with minimal trauma and the least tissue damage.Citation7–Citation9 The cosmetic results assume great importance, considering that about 69% of these lesions are benign.Citation10 The only drawback of this method is that it may lead to inadequate removal of an unexpected cancer, therefore requiring a second operation to achieve a clear margin. Preoperative diagnostic procedures that give a surgeon an idea regarding the possibility of a malignant lesion are radiological imaging (mammography, ultrasound, magnetic resonance imaging), image-guided fine needle aspiration cytology, image-guided core needle biopsy, and needle localization followed by open surgical biopsy. Needle localization followed by open surgical biopsy is considered to be the most accurate procedure today. This is achieved with minimal complication rates.
We conducted this study to evaluate the usefulness of hook wire localization biopsy under imaging guidance for nonpalpable breast lesions, to assess the correlation between preoperative imaging assessment and final diagnosis, and to determine its usefulness in making a final diagnosis and any associated complications.
Materials and methods
This was a descriptive retrospective study conducted in the Department of Radiology, Aga Khan University Hospital. All patients undergoing needle localization biopsy of a breast lesion under mammographic or ultrasound guidance between January 2009 and December 2010 were included. Patients with incomplete medical records were excluded. All patients underwent mammography followed by ultrasound examinations in the event of equivocal findings. All patients’ mammograms and ultrasound examinations were categorized using Breast Imaging-Reporting and Data System (BI-RADS®) assessment categories. Needle localizations were performed either under ultrasound guidance if the lesion was seen on ultrasonography or by stereotactic mammographic guidance for suspicious mammographic abnormalities (). All ultrasound-guided needle localizations were performed using a 5 cm 20G Kopan’s hook wire needle.
Figure 1 True Lateral View of mammogram right breast showing Kopan’s 20G 9cm needle localizing a soft tissue nodule (Black circle).

After the needle localization was done, two mammographic views were taken in order to provide a road map to the breast surgeon for specimen removal, and the position of the needle was also shown by a line diagram in the patient’s confidential file. Mammographic stereotactic localizations were done using a 9 cm 20-gauge Kopan’s hook wire needle, and the procedure was performed using a Mammomat 3000 Nova Siemens mammography machine.
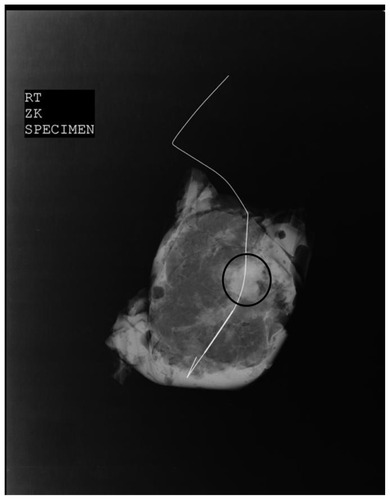
After the procedure, all patients were bandaged and immediately sent to the operating theater for the definitive procedure. The excised specimen was then subjected to ultrasound in case of ultrasound-guided needle placement or a magnified mammographic view () if the localization was done using stereotactic mammographic guidance to confirm adequate removal of the localized specimen. The specimen was then sent to histopathology for a definitive diagnosis. The percentages of benign and malignant lesions were determined by pathological examination of the surgically removed specimen. A correlation was sought between the preoperative imaging assessment and the final diagnosis made. Complications associated with the procedure were also recorded.
Figure 2 Magnified view of excised breast specimen showing the localized soft tissue density nodule (Black Circle) with Kopan’s wire in situ.
Results
The mean age of the patients was 51.89 ± 11.75 years. A total of 151 mammograms were included, of which 75 were done for screening and 76 for diagnostic purposes. On mammography, the parenchymal patterns were fatty, fibroglandular, heterogeneously dense, and dense in 10, 62, 65, and 14 patients, respectively. The locations of the breast lesions in 52, 20, 21, 25, and 23 were in the upper outer quadrant, lower outer quadrant, upper inner quadrant, lower inner quadrant, and retroareolar area, respectively. A total of 151 biopsies were carried out, with 80 performed under mammographic guidance and 71 performed under ultrasound guidance. Of 80 needle localizations, 54 were done for microcalcifications and 26 were performed for a suspicious mammographic soft tissue density or architectural distortion with or without microcalcifications. Localizations done under ultrasound guidance were performed for sono-graphically detected suspicious solid lesions. The overall malignancy rate was 25.16%. Of 93 cases reported as malignant, 60 turned out to be malignant and of the 58 cases reported as benign, three were reported to be malignant on histopathology (). The final histopathological outcome is given in . The sensitivity of the imaging modalities was 95% and the specificity was 62%. The malignancy rate was 5% for benign lesions and 64% for malignant lesions, respectively. The imaging and pathological findings were concordant in 63.95% of malignant lesions and 95% of benign lesions. Needle localization biopsy was able to make the diagnosis in 100% of cases. There were no major complications related to wire localization, eg, hematoma formation or migration of the localization wire. Two patients had minor complications following surgical excision in the form of hematoma at the site of excision, and both were treated conservatively. There was complete resolution of the hematoma at the 15-day follow-up visit, giving a complication rate of 1.32%.
Table 1 Summary of final outcome according to BI-RADS® category
Table 2 Summary of histopathological outcome for needle-localized lesion
Discussion
Treatment of breast cancer has progressed from radical mastectomy to a more minimally invasive approach of breast-conserving surgery. While marked improvement has been achieved in the management of breast cancer over recent years, early detection remains the best way to achieve a favorable outcome. The best method available to date for preoperative localization of a nonpalpable breast lesion detected on imaging is the hook wire localization technique described by Frank et al.Citation11 This method was used in our study, and lesions detected on ultrasound or mammogram were subjected to ultrasound and stereotactic mammographically-guided needle localizations, respectively. In our study, needle localizations were also performed for lesions that were reported as benign, but with a strong family history of breast cancer or breast cancer diagnosed or treated in the contralateral breast.
The malignancy rate for a benign lesion was only 5%, whereas the malignancy rate for lesions reported as malignant on imaging was much higher at 62%. However, the overall malignancy rate in our study was 25.16%, which is comparable with a study by Morrow et alCitation12 who reported a malignancy rate of 24%. In their study, a total of 1852 abnormalities in 1550 consecutive patients were prospectively categorized for the level of cancer risk and underwent stereotactic core needle biopsy or diagnostic needle localization and surgical excision. The malignancy rate was between the 19% and 32.2% reported by Denning et alCitation13 and Schwartz et al,Citation14 respectively. Denning et alCitation13 studied 100 patients whereas Schwartz et alCitation14 studied 469 patients, so the number of patients included in the study might have affected the overall malignancy rate, because our study had 151 patients, which is in between the number of patients studied by Denning et alCitation13 and Schwartz et al.Citation14
The concordance rate between the imaging findings and histopathology was 95% for benign lesions and 63.95% for malignant lesions, which is similar to that in the study by Jortay et al,Citation15 who reported a concordance of 98% and 64% for benign and malignant lesions, respectively. Jortay et alCitation15 studied the contribution of wire localization breast biopsy to the pathological diagnosis of mammographic lesions. Their study included 152 patients with nonpalpable breast lesions; however, all patients were subjected to mammography and all then underwent needle localization and excision biopsy of a localized lesion followed by histopathology.
Needle localization followed by open surgical biopsy is safe, with a negligible minor complication rate of 1.3%. The complications did not occur during the needle localization procedure, with two patients developing hematomas after open surgical biopsy. Both patients were managed conservatively. Furthermore, the biopsy results strongly influence the algorithm for evaluation of suspicious lesions.Citation16
There are a few limitations to our study. The sample size was small, so any conclusions cannot be generalized. It was also a retrospective study, and all patients who underwent needle localizations during the study period were included. Perhaps if the study had been conducted prospectively, more stringent patient selection could have been adopted, thus affecting the final outcome. Needle localization was done in all patients coming for screening as well as for diagnostic study, eg, in a patient with known malignancy in one breast and having a suspicious lesion on the opposite side. Localization biopsy was planned to rule out a second malignant lesion on the contralateral side and this might have affected the malignancy rate in lesions appearing benign on imaging.
Conclusion
The study shows that hook wire localization biopsy under imaging guidance for nonpalpable breast lesions is a useful procedure in making the final diagnosis. It is a safe and effective procedure for definitive diagnosis of suspicious lesions on imaging, thus being more helpful if the imaging findings are suspicious.
Disclosure
The authors report no conflicts of interest in this work.
References
- American Cancer SocietyCancer facts and figures Available from: http://www.cancer.org/Research/CancerFactsFigures/CancerFactsFigures/indexAccessed June 5, 2012
- LangNPTalbertGEShewmakeKBThe current evaluation of non-palpable breast lesionsArch Surg1987122138913913689114
- ShapiroSVenctWStraxPSelection, follow-up, and analysis in the health insurance plan study: a randomized trial with breast cancer screeningNatl Cancer Inst Monogr19856765744047153
- KwongACheungPSWongAYThe acceptance and feasibility of breast cancer screening in the EastBreast200817425017720500
- ErnstMFAvenariusJKSchuurKHRoukemaJAWire localization of non-palpable breast lesions: out of date?Breast20021140841314965704
- Della RovereGQBensonJPMorganMWarrenRPatelALocalization of impalpable breast lesions – a surgical approachEur J Surg Oncol1996224784828903489
- BigelowRSmithRGoodmanPAWilsonGSNeedle localization of non-palpable breast massesArch Surg198512055655693985797
- SymmondsRERobertsJWManagement of non palpable breast abnormalitiesAnn Surg198720555205283579400
- GisvoldJJMartinJKPrebiopsy localization on nonpalpable breast lesionsAJR198414334774816331724
- MarkopoulosCKakisisJKouskosSManagement of nonpalpable, mammographically detectable breast lesionsWorld J Surg19992343443810085389
- FrankHAHallFMSteerMLPreoperative localization of non palpable breast lesions demonstrated by mammographyN Engl J Med1976295259260934190
- MorrowMVentaLStinsonTBennettBCProspective comparison of stereotactic core biopsy and surgical excision as diagnostic procedures for breast cancer patientsAnn Surg200123353754111303136
- DenningDPFashaGJMcBoyleMFRole of needle localization of nonpalpable lesionsAm J Surg19871545935963425800
- SchwartzGFFeigSARosenbergALPatchefskyASLocalization and significance of clinically occult breast lesions: experience with 469 needle-guided biopsiesRecent Results Cancer Res1984901251326701369
- JortayAMDaledHFaverlyDContribution of hook-guided breast biopsy to the pathological diagnosis of mammographic lesionsActa Chir Belg199999262910090960
- ImranaMShaistaAGulnazSComparison of stereotactic core breast biopsy and open surgical biopsy results at a tertiary care hospital in PakistanInt J Womens Health2011319319621792341