Abstract
Immigrant Latinas may have different cultural attitudes toward menopause and aging, and may experience higher levels of distress associated with adaptation to their new environment. The purpose of this secondary analysis was to describe the frequency of depressive symptoms experienced by premenopausal Latinas (40–50 years of age) living in the United States and compare Latinas born in the US with immigrant Latinas on stress and sociodemographic factors that influence depressive symptom experience. Analysis was conducted on a subsample of 94 self-identified Latinas who participated in a longitudinal study and completed the Center for Epidemiological Studies-Depression (CES-D) scale at enrollment and 6 months. Immigrant Latinas had a significantly higher CES-D (14.4 ± 11.1) than US-born Latinas (10.0 ± 7.9) and the difference remained at 6 months. There was no difference in age, body mass index (BMI), self-report of general health, or perceived stress. Higher BMI, work-related stress, and insufficient income for essential daily needs were associated with depressive symptom scores in immigrant Latinas. High BMI and less education were associated with depressive symptom scores in the US-born Latinas.
Introduction
Latinos comprise the largest and fastest growing minority in the United States. The 2010 US census reports that 16% of the total population identifies as Latino (50.5 million), and approximately 48% are women.Citation1 The term Hispanic or Latino used in the 2010 census refers to a person of Cuban, Mexican, Puerto Rican, South or Central American, or other Spanish culture or origin regardless of race.Citation1 Latinas in the US are a heterogeneous group, differing by country of origin, immigration history, geographical location, religion, cultural beliefs, education, and level of acculturation. These factors have a profound effect on the health and lifestyle of Latinas in the US. More than two-thirds of Latinas living in the US are of Mexican origin, with smaller proportions from Central America, South America, and the Caribbean. Almost half of US Latinas are foreign-born.Citation2 Many key indicators demonstrate that Latinas in the US are disadvantaged by limited English proficiency (45% of Latinas), less formal education, living below the federal poverty level, and having no health insurance.Citation2,Citation3
Voluntary immigration to the US involves physical relocation that is often preceded by complicated decision making. Studies find that the health status of immigrant Latinos is better than other adults living in the US. However, these benefits are believed to diminish as their time in the US increases. Changes in Latinos’ health status are associated with stress from traumatic components of the immigration experience, separation from family, environmental shifts, and disruptions of their cultural milieu. Studies in several Western countries report adverse consequences in the mental health of their immigrants and refugees; extensive changes during immigration and resettlement can have a deleterious effect on immigrants and their health, placing them at high risk for health disparities.Citation4–Citation8
The Center for Disease Control and Prevention (CDC) reported that an estimated 9% of adults living in the US reported experiencing depressive symptoms in 2006 and 2008.Citation9 Women were significantly more likely to report major depression (10.2%) than men (8%). Research indicates that adults, in addition to females, are more likely to meet the diagnostic criteria for depression if they are middle-aged, never married, or have less than a high school education.Citation3
Epidemiological and clinical data support the notion that hormonal changes across the female reproductive life cycle can bring physical and emotional disturbances in women, resulting in poor health and lower quality of life. A growing number of clinical studies demonstrate that midlife women, defined as between 40 and 60 years of age, are at risk for depressive symptoms, making mental health a significant issue for aging women.Citation10,Citation11 However, researchers have not focused specifically on the late premenopausal reproductive stage in this age group. Women between 40 and 60 years of age can be either late premenopausal, perimenopausal or menopause transitional (with variation in menstrual cycle length and fluctuations in ovarian hormones), or postmenopausal, which refers to the 5 years after the final menstrual period.Citation12
A wide variety of symptoms experienced throughout the transition to menopause require researchers to look beyond the decline of estrogen during menopausal transition and consider psychosocial links between depressive symptoms and significant life stressors, such as ethnicity, lifestyle, education, language, exercise, and obesity – all of which are associated with experiences during menopausal transitional.Citation12,Citation13
This research was guided by the Theory of Symptom Management,Citation14 in which symptoms are perceived and experienced through the interaction of the person, the person’s environment and the person’s health status. For this study, the “persons” are healthy women in the late premenopausal stage of reproduction prior to cessation of menses. Their environment includes Latino heritage, perceived stress, and immigration status. Health status for this study is specific to depressive symptom experiences.
The purpose of this secondary analysis is to examine the frequency of depressive symptoms measured by self-report responses on the Center for Epidemiological Studies Depression scale (CES-D)Citation15 in a subsample of Latinas who participated in a larger longitudinal study of menopausal transition that also included other ethnic groups. At enrollment there were 94 Latinas with regular menstrual cycles and low follicle stimulating hormone (FSH) levels. This Latina sample remained late premenopausal throughout the first year of the study. In this Latina sample, 57 were born in the US and 37 had immigrated to the US from Mexico (n = 24) or Central American countries that included El Salvador (n = 5), Guatemala (n = 5), Nicaragua (n = 2), and Costa Rica (n = 1). To be eligible for enrollment, they had to be comfortable with the English language and have lived in the US for at least 15 years. We hypothesized that the Latina immigrants would differ on many demographic characteristics, report more stress, and have higher CES-D depressive symptom scores than Latinas born in the US.
Methods
Participants
In the larger study,Citation11 a convenience sample of healthy women was recruited from community settings in the San Francisco Bay Area if they self-described as Caucasian, Black, or Latina; spoke English; and had lived in the US for at least the past 15 years. To meet inclusion criteria, women were enrolled if they were still having regular menstrual cycles; were between 40 and 50 years of age; had no major health problems; and were not currently taking hormones, pregnant, or planning a pregnancy.
This particular analysis focuses on the 94 Latina participants from the larger study.Citation11 The Latina participants were solicited through Spanish and English public advertisements, including relevant cultural flyers in community-based locations, public announcements on English and Spanish radio and television stations, and personal recruitment contacts using age, gender, and ethnic-appropriate matched recruiters. As seen in , this sample from the San Francisco Bay Area was representative of the demographic profile for California’s Latino population.Citation16 Comparisons for physical activity and anthropometric characteristics between the Latinas and non-Hispanic White women have been reported by Juarbe et al.Citation17
Table 1 Sociodemographic characteristics of Latina participants (n = 94)
Procedures
Data were collected after receiving approval from the Committee on Human Research (CHR) at the University of California, San Francisco, USA. The study was explained to each participant and they gave informed consent. After receiving each participant’s informed written consent in English, an individual screening appointment was scheduled. Trained bilingual (English–Spanish) research assistants helped each participant with the completion of the English-language questionnaires as needed, particularly for literacy issues or for symptoms that may not be part of everyday conversation. Demographic data were collected at enrollment and updated on an annual basis; data on symptoms and menstrual cycles were collected by telephone every 2 months and laboratory and questionnaire data were obtained every 6 months.
Measures
For this secondary analysis, data from the larger studyCitation11 included demographic characteristics, as well as attitudes toward aging and menopause, self-reported stress perception, and CES-D scores at enrollment (Time 1) and 6 months (Time 2). At each 6-month time point, height and weight were obtained at a face-to-face visit and menopausal status was monitored by measures of urinary FSH levels in conjunction with self-reported regularity of their menstrual cycles.
Based on the Theory of Symptom Management,Citation14 self-reporting is the gold standard for measuring symptoms. The 20-item CES-D scaleCitation15 was administered in English to estimate the frequency of depression symptoms. Respondents rated how often each symptom was experienced during the past week on a 4-point scale of “rarely or none of the time (0)” to “most or all of the time (3).” Scores range from 0 to 60, with a score of 16 or above indicating a high level of depressive symptoms. Although this cut-point corresponds to the 80th percentile of scores in community samples, studies with Mexican Americans and other Latinos have demonstrated higher mean depression scores, possibly attributed to lower economic status and exposure to chronic stress.Citation18,Citation19
Attitude toward menopause was measured with the Attitudes Toward Menopause (ATM) checklist created by Neugarten et al.Citation20 The instrument consists of 35 items rated on a 4-point Likert scale from strongly agree (1) to strongly disagree (4). Internal consistency reliability was adequate (Cronbach’s alpha = 0.80) and concurrent validity between the ATM and Bowles’ Menopause Attitude Scale was sufficient (Pearson’s r = 0.63).Citation20 The Attitude Toward Aging (ATA) scale was used to measure attitude toward aging.Citation21 The ATA has 22 items rated on a 4-point Likert scale from strongly agree (1) to strongly disagree (4). The ATA combines items from other instruments that have demonstrated adequate content validity and high reliability coefficients reported elsewhere in similar community based samples.Citation21 Higher score indicates a more positive attitude for both scales.
Stress perception was measured using four items developed by our research team to address specific sources of stress in women’s lives. Participants were asked to rate their level of stress for four specific dimensions of their life: work, family, personal, and health. Responses were on 5-point Likert scale from very stressful (1) to not at all stressful (5) during the past month. This 5-item stress perception scale was internally consistent at the initial assessment (Cronbach’s alpha = 0.60) and remained adequate (Cronbach’s alpha > 0.65) at each time point. Concurrent validity was obtained when compared to scores on the 10-item Perceived Stress Scale Citation22 that assesses general stress during the past month (Pearson’s r = 0.65).
Analysis
The data for sociodemographic characteristics and health-related variables were analyzed by descriptive statistics including frequencies and measures of central tendency using SPSS version 20 (IBM Corporation, Chicago, IL, USA). Relationships between continuous variables were tested with Pearson’s correlation coefficients. Group differences in sociodemographics, stress, and CES-D scores were tested with Chi-square for categorical data or with unpaired t-tests for continuous data. A two-tailed significance level was set at P < 0.05. To account for the variance in depressive symptoms by group, multiple linear regression models included sociodemographic, health, and stress as independent variables that were analyzed in separate models for the US-born Latinas and the immigrant Latinas.
Results
Sociodemographic differences
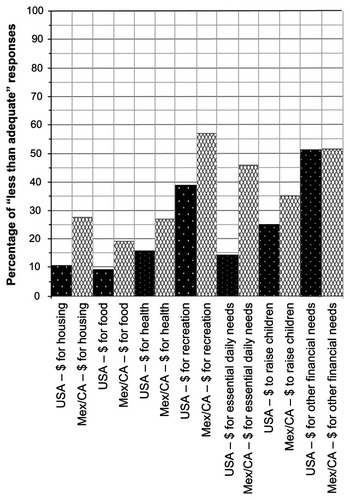
There were no significant group differences in age, BMI, marital status, or self-reported annual family income (). However, when asked about the adequacy of their income, more foreign-born Latinas described having inadequate income to meet their needs for housing, food, essential daily needs, and raising children. They did not differ on income adequacy for health care needs ( and ). Significantly more women were mothers in the immigrant Latinas group (97%) compared to US born women (59%). There was no difference between the two groups for rate of employment outside the home; however, there was a significant difference in the type of employment ().
Figure 1 Responses for “less than adequate income to meet needs” reported by Latinas born in the US and Latinas born in Mexico or Central America.
Stress, depressive symptoms, and other health measures
The two groups of late-stage premenopausal women did not differ on attitudes toward menopause. However, compared to the immigrant Latinas, the US-born Latinas had a more negative attitude toward aging (), reported more specific stress in relation to work, and reported less specific stress in relation to family issues. The two groups did not differ on perceived stress or specific stress related to physical health or personal issues.
Table 2 Self-report health measures
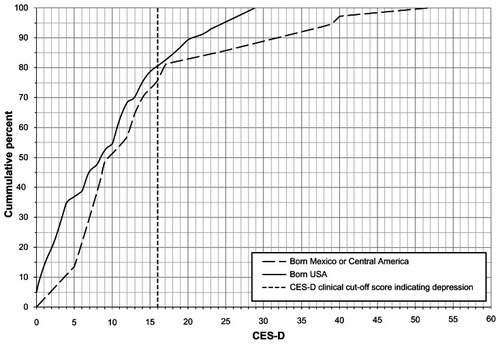
The two groups differed significantly on CES-D scores. On average, CES-D scores in this sample of Latinas were below the clinical cutoff score of 16 at both time points. However, as seen in and , the mean CES-D score was significantly higher for the immigrant group compared to the US-born Latinas at enrollment, and this difference was similar at 6 months (data not shown).
Figure 2 Comparison of CES-D scores for Latinas born in the US and Latinas born in Mexico or Central America.
Higher CES-D scores were correlated with less overall family income (r = −0.278, P = 0.007) and inadequate income for essential daily needs (r = −0.370, P < 0.001). Higher CES-D scores were significantly correlated with lower level of education (r = −0.369), higher BMI (r = 0.317), worse general health perception (r = 0.365), and more negative attitudes toward aging (r = −0.358) and menopause (r = −0.312). CES-D scores were positively related to all measures of stress, including physical health stress (r = 0.469), family stress (r = 0.303), personal stress (r = 0.453), and perceived stress (r = 0.461).
In multiple regression models, different sociodemographic variables accounted for the variance in CES-D scores for the US-born women compared to the immigrant women. For the US-born Latinas, the overall model was significant (F[6,55] = 4.68, P = 0.001) and accounted for 32% of the variance in CES-D scores; low income (P = 0.009), no partner (P = 0.025), and high total stress scores (P = 0.001) were significant predictors. BMI, education, and attitudes toward aging did not reach statistical significance when sociodemographic variables and stress scores were controlled. For the immigrant Latinas, the overall model was also significant (F[6,36] = 4.89, P = 0.002) and accounted for 44% of the variance in CES-D scores; high total stress scores explained most of the variance (P < 0.001), and high BMI (P = 0.07) approached significance before controlling for the other five variables.
Discussion
Results of this secondary analysis provide preliminary insight into the differences within groups of midlife Latinas by immigration history. The high CES-D scores in this sample are congruent with the epidemiological evidence from Soares,Citation13 indicating that the late premenopausal stage in transition to early menopause stage can be a time of vulnerability associated with an increased risk of depressive symptoms. The notion of depressive symptoms being purely biological is not supported by research,Citation23 and theoretical proposals for explaining this “window of vulnerability”Citation13 point to multiple factors that can impact vulnerability for premenopausal depressive symptoms, including neuroendocrine aberrations, psychosocial underpinnings, history of mood disorder, personality traits, history of psychological trauma, and demanding social roles.Citation23,Citation24
For example, environmental factors are conceptualized to include the social, physical and cultural context in which the symptoms occur. Immigrant Latinas may be affected by their social reality of family separation, limited English proficiency, limited access to resources (such as health care), and other acculturation factors that can contribute to their experience of depressive symptoms.Citation8,Citation25 The concept of person in the theoretical model is expressed by variables such as gender and stage of development. Therefore measuring depressive symptoms just prior to onset of a woman’s menopausal transition can shed light on the ways in which physiological, psychological, sociocultural, and behavioral variables interact and activate one another in influencing a midlife woman’s depressive symptom experience.
Golding et alCitation19 also examined ethnic and immigration status differences in CES-D scores in a sample of over 4000 Mexican American males and females. Gender was controlled in their comparisons, but no report of actual gender differences was included. Higher depressive symptom scores were reported among those Mexican Americans who were born in the US compared to immigrants but the authors concluded that ethnic and immigration differences for individual CES-D symptom items did not account for differences in mean scores. There were ethnic differences in CES-D items. Mexican-Americans where more likely to report symptoms reflecting lack of positive affect (hopeful, happy, enjoy) than non-Hispanic Whites, suggesting that that these items in the CES-D may have limited cross-cultural validity as an indicator of depressed mood. They did not detect any immigration bias between Mexican Americans born in Mexico and those born in the US. The difference in immigration status was consistent across symptoms, reflecting the core constructs of depression.
The CES-D depression scale and other measures were administered in English with the assistance of the same Spanish-speaking data collector for all Latinas in the study at Time 1. Although the inclusion criteria for the study included being English-speaking, nearly 30% of US-born Latinas and 47% of immigrant Latinas reported reading and speaking Spanish better than English (). The level of English proficiency of these Latinas could be a confounding factor. The interpretation of the CES-D questions could vary by a systematic difference, where the instrument semantic equivalence (the way the words and sentences are translated) and conceptual equivalence across cultures (the concept being measured is the same across cultural groups) are affected and not equivalent.Citation26 The measurement of depressive symptoms also needs cultural relevance and sensitivity. Although the CES-D is widely used in research with racial/ethnic minorities, a recent meta-analysisCitation27 demonstrated that the original four factors in the CES-D (depressed affect, positive affect, somatic symptoms, and interpersonal problems) varied substantially between ethnic groups, suggesting that depressive symptoms may present in unique ways for different racial and ethnic groups.Citation17,Citation27
In the sample we have analyzed in this paper, attitudes toward menopause were similar for the two groups, but attitudes toward aging were more positive for US-born Latinas than for immigrant Latinas. Although some researchers report a relationship between symptom experiences and attitudes toward aging or menopause,Citation28 ethnic and cultural values do not support the increased risk for depressive symptoms experienced by immigrant Latinas.Citation14 Multiethnic and cross-cultural studies of the menopausal symptoms have found that Latinas do not often discuss their menopausal symptoms, choosing instead to remain optimistic, perceiving menopausal changes as a part of life, and Latinas try to manage the symptoms by “tolerating, ignoring, normalizing and minimizing.”Citation29
For our sample of Latinas, stress variables were significantly correlated with depressive symptom scores. The stress related to family issues was significantly higher for Latinas born outside the US, and work stress was significantly higher for US-born Latinas. Immigrant Latinas may experience higher levels of stress related to adaptation to a new environment, legal immigration pressures, institutional patterns of oppression, societal xenophobia, racism, lack of economic mobility, and economic insecurity.Citation7,Citation8 These stressors can trigger depressive symptoms regardless of age. Socioeconomic and environmental factors, as well as the documented physical changes during menopause transition, place immigrant Latinas at an increased risk for depression and may account for the higher CES-D scores for immigrant Latinas compared to US-born Latinas of the same age in our healthy community-based sample of women in the decade prior to the onset of menopause.
Limitations
Although the social, economic, and educational diversity of US-born and immigrant Latinas in our convenience sample was representative of the Latina population in California, this analysis was limited by a small sample of Latinas from the San Francisco Bay Area, and may not fully represent all Latinas living in California or the US. However, findings from this secondary analysis shed light on possible reasons for the higher risk of depressive symptoms in midlife Latinas and that this higher risk occurs even prior to the onset of menopause.
Conclusion
Health care providers are often faced with challenges surrounding the care of multiethnic and multicultural women. Minority women and immigrants are reported to suffer higher rates of health disparities. Efforts to reduce health disparities outlined in the new objectives of the US Department of Health and Human Service’s Healthy People 2020 initiative includes screening midlife women for depressive symptoms and other mental health disorders.Citation29 Based on our findings from this secondary analysis, depressive symptoms may be alleviated by strategic interventions that consider stress and the interactions between person, environment, and health. This analysis aims to examine how depressive symptoms in midlife US Latinas vary from symptoms of immigrant Latinas.
Studies that compare minority midlife women living in the US can inform health care providers of differences and similarities in their symptom experiences. Attention to their perceptions and experiences can contribute to efforts to assess the extent in which different menopausal symptoms might be prevalent in ethnic minorities.Citation30 Furthermore, qualitative data can provide potential directions for culturally congruent menopausal symptom management in multiethnic societies.Citation31
Social, political, economic, and cultural forces that impact women’s health needs should always be considered, particularly during transitions such as pregnancy or menopause.Citation24 The use of specific, culturally and linguistically appropriate screening and diagnostic tools for depressive symptoms in Latinas can assist health care providers with early detection and clinical management. Treatment strategies should be tailored; resources should be included and available to reduce the significant burden and functional impairment associated with depressive symptoms in midlife Latinas even prior to the onset of menopause when additional symptom management issues will need to be addressed.
Acknowledgments
The research was funded by the National Institutes of Health: R01 NR04259 (Dr K A Lee) and a T32 NR07088 traineeship (Dr R M Sternberg).
Disclosure
The authors report no conflicts of interest in this work.
References
- United States Census Bureau [webpage on the Internet]Overview of race and Hispanic Origin: 2010 Census Briefs32011 Available from: http://www.census.gov/prod/cen2010/briefs/c2010br-04.pdfAccessed July 28, 2012
- FrostJJDriscollAKSexual and Reproductive Health of US Latinas: A Literature ReviewOccasional Report No 19New York, NYAllan Guttmacher Institute2006
- HeilemannMSVCoffey-LoveMFrutosLPerceived reasons for depression among low-income women of Mexican descentArch Psychiatr Nurs20041818519215529284
- LassetterJHCallisterLCThe impact of migration on the health of voluntary migrants in western societiesJ Transcultural Nursing20092093104
- Hsin-Chun TsaiJImmigrant vulnerability: does capitalism in the United States matter?ChesnayMAndersonBACaring for the Vulnerable. Perspectives in Nursing Theory, Practice, and Research2nd edSudsbury, MAJones and Bartlett2008277286
- RevolloHWQureshiACollazozFValeroSCasasMAcculturative stress as a risk factor of depression and anxiety in the Latina American immigrant populationIntern Rev Psychiatry2011238492
- MarsigliaFFKulisSGarcia PerezHParsaiMHopelessness, family stress, and depression among Mexican-heritage mothers in the SouthwestHealth Soc Work201136171821446605
- SternbergRMBarryCTransnational mothers crossing the border and bringing their health care needsJ Nurs Scholarsh201143647121342426
- US Department of Health and Human Services. Centers for Disease Control and PreventionRevised estimates for depression in the USMMWR-Morbidity and Mortality Weekly Report20105912291235Accessed on November 15, 201120881934
- DennersteinLSoaresCNThe unique challenges of managing depression in mid-life womenWorld Psychiatry2008713714218836580
- GillissCLeeKGutierrezYTaylorDRecruitment and retention of healthy minority women into community-based longitudinal researchJ Womens Health Gend Based Med200110778511224947
- NoseckMKennedyHPBeyeneYTaylorDGillisCLeeKThe effects of perceived stress and attitudes toward menopause and aging on symptoms of menopauseJ Midwifery Womens Health20105532833420630359
- SoaresCNCan depression be a menopause-associated risk?BMC Medicine201087921122126
- HumphreysJLeeKACarrieri-KohlmanVTheory of symptom managementSmithMJLiehrPMiddle Range Theory for NursingNew York, NYSpringer2008145158
- RadloffLThe CES-D scale: a self-report depression scale for research in the general populationAppl Psychol Meas19771385401
- California Department of Health Services. Office of Women’s Health2007California Women’s HealthSacramento, CA Available from: http://www.dhs.ca.gov/director/owhAccessed on February 12, 2012
- JuarbeTCGutiérrezYGillisCLLeeKADepressive symptoms, physical activity, and weight gain in premenopausal Latina and white womenMaturitas20055511612516846703
- PedenARRayensMKHallLAA community–based depression prevention intervention with low-income single mothersJ Am Psychiatr Nurses Assoc2005111825
- GoldingJMAneshenselCSHoughRLResponses to depression scale items among Mexican-Americans and non-Hispanic whitesJ Clin Psychol19914761742026780
- NeugartenBLWoodVKrainesRJLoomisBWomen’s attitude toward the menopauseVita Hum Int Z Lebensalterforsch1963614015113938146
- PatsdaughterCAThe Mother-Daughter Relationship in Menopause and the Aging Process [dissertation]Seattle WAUniversity of Washington1989
- CohenSWilliamsonGPerceived stress in a probability sample of the United StatesSpacapanSOskampSThe Social Psychology of HealthNewbury Park, CASage1988 Available from: http://www.ncsu.edu/assessment/resources/perceived_stress_scale.pdfAccessed May 20, 2013
- SomersetWNewportJDRaganKStoweZNDepressive disorders in women: from menarche to beyond menopauseKeyesCLMGoodmanSHWomen and DepressionNew York, NYCambridge20066288
- AndristLMcPhersonKIConceptual models for women’s health research: reclaiming menopause as an exemplar of nursing’s contributions to feminist scholarshipAnnu Rev Nurs Res200119296011439785
- HeilemannMSVCopelandDSources of emotional help sought by low-income women of Mexican descentIssues Ment Health Nurs20052618520415966112
- Center for Aging in Diverse Communities, Measurements ad Methods Core, University of California, San Francisco2010Guidelines for translating surveys in cross-cultural research Available from: http://medicine.ucsf.edu/cadc/cores/measurement/methods.htmlAccessed December 10, 2012
- KimGDeCosterJHuangCHChiribogaDARace/ethnicity and the factor structure of the center for epidemiologic studies depression scale: a meta–analysisCultur Divers Ethnic Minor Psychol20111738139621988578
- PitkinJCultural issues and the menopauseMenopause Int201016415616121156853
- US Department of Health and Human ServicesHealthy People 2020: Keeping the Nation Healthy Available from: http://www.thecommunityguide.org/mentalhealth/collab-care.htmlAccessed June 17, 2012
- MelbyMKSievertLLAndersonDObermeyerCMOverview of methods used in cross-cultural comparison of menopausal symptoms and their determinants: Guidelines strengthening the reporting of menopause and aging (STROMA) studiesMaturitas2011709910921840143
- ImEOLeeBICheeWDormireSBrownAA national multiethnic online forum study on menopausal symptom experienceNurs Res2010591263320010042