
Abstract
An ectopic kidney is a rare congenital defect that is often asymptomatic, but can be incidentally discovered during imaging examinations. Moreover, the morphological characteristics and laboratory features of ectopic kidneys are nonspecific, which may lead to misleading diagnostic approaches, particularly when there are additional factors, such as infection, obstruction, or other anomalies. A 43-year-old female presented with a mass in the left adnexal area. She had septate uterus and a history of congenital urinary incontinence. Ultrasound and MRI findings indicated that the mass was a cyst originating from the ovary. However, it is possible that the lump was derived from the urinary system. To confirm the diagnosis, laparoscopy was performed, followed by pathological examination, which confirmed the presence of an ectopic kidney with a single-system ectopic ureter. The patient underwent nephroureterectomy, and her symptoms successfully resolved, leading to a favorable prognosis. This case report highlights a rare case involving an ectopic kidney with a vaginal ectopic ureter that initially presented as an adnexal cyst and caused urinary dribbling. This case emphasizes the importance of early recognition and accurate diagnosis in women with similar symptoms.
Introduction
The incidence of ectopic kidney disease is estimated to be 1:500–1:1200.Citation1 It occurs due to failure of normal ascent or medial rotation of the kidney during embryogenesis.Citation2 Ectopic kidneys can be found in various positions, such as the pelvis (1:2200–1:3000), iliac fossa, abdomen, thoracic cavity, and contralateral positions.Citation3 The presence of a pelvic kidney indicated a defect in the ascension of the ureteric bud to the renal fossa. Ectopic kidneys are typically asymptomatic and are often discovered incidentally. However, the imaging findings were atypical. In cases where they are associated with other conditions such as infection, calculi, or malignancy, abnormal positioning of the kidney may cause nonclassical symptoms, leading to a more challenging diagnosis.Citation4–6
Ectopic ureters occur in approximately in 1:1900 persons. The female-to-male ratio was greater than 2:1.Citation2 More than 80% of the cases involve ureteral duplication, whereas single-system ectopic ureters are less common.Citation7 In female, ectopic openings can be located in the urethra, vagina, uterus, or fallopian tubes. Vaginal ureter opening accounts for 25% of all cases, and is usually associated with congenital urinary dribbling. Ectopic ureters are frequently combined with renal maldevelopment.Citation8 However, as the patient ages, various causes of urine incontinence are increasing, thus the diagnosis of ectopic ureter is overlooked, especially when the ectopic orifice is hidden.Citation9
Cases of ectopic kidneys that interfere with gynecological diagnosis have rarely been described.Citation3 In this article, we present an unusual case of a female patient whose ectopic pelvic kidney led to a presentation similar to that of an adnexal cyst, along with an ectopic vaginal ureter resulting in urine incontinence. We also summarized the related literature. This case was reported in accordance with SCARE criteria.Citation10 Institutional review board/ethics committee approval was obtained for this study (reference number: 2023–94), and written informed consent was obtained from the patient.
Case Report
A 43-year old female, G4P2, presented with transvaginal ultrasound reported pelvic mass for 5 months, consulted our hospital for surgery. Ultrasonography revealed a 69×36 × 26 mm cyst on the upper left side of the uterus, which could be an encapsulated effusion; however, the mass might also be originated from urinary system. Doppler studies have also suggested the presence of septate uterus.
The patient had a history of dull pain in the lower abdomen for more than 10 years, unrelated to menstrual cycle. She was diagnosed as chronic pelvic infection in a local hospital, and was administered intravenous antibiotics. After that, the pain relieved. She also reported involuntary urinary leakage from the vagina in childhood. Urine leakage was continuous and had no definite cause. The patient used two sanitary napkins per day to collect urine.
The patient underwent abdominal surgery for a pelvic mass in 2009 during the second trimester of pregnancy. However, the surgery ended after intraoperative exploration without removal of the mass because of the difficulty in achieving hemostasis. The origin of pelvic masses is unclear. Postpartum ultrasonography did not reveal any cysts. In addition, she underwent 2 cesarean sections, 2 induced abortions, and 1 cholecystectomy.
The patient began to menstruate regularly at 14 years of age at intervals of 26 days, for a period of 7 days, without dysmenorrhea. The patient had no history of chronic medical illness. She also reported that she had been diagnosed with “solitary kidneys” since childhood.
To investigate the cause of the patient’s urine leakage, we examined whether she had vesicovaginal fistula or stress urinary incontinence. However, no visible fistula opening was observed during the vaginal examination. Ultrasonography of the urinary system revealed a normal right kidney and ureter but failed to visualize the left side. CT urography revealed normal images of the right kidney, right ureter, and bladder. However, there was a possibility of an ectopic left kidney with an ectopic ureter opening on the left side (). Magnetic resonance imaging (MRI) of the pelvic region revealed a septate uterus. Additionally, a benign cyst measuring 42×64 mm was found in the left adnexal area and there was a physiologic right ovarian cyst measuring 49×32 mm. A lesion near the uterine, which could potentially be a dysplastic ureter, was also observed (). However, no obvious vesicovaginal fistula was detected during vaginoscopy. For further investigation, we conducted a methylene blue test by injecting methylene blue solution from the urethra into the bladder. No blue liquid was discharged from the vagina, and the patient did not report any blue staining in her sanitary napkin. The urodynamic test showed a normal voiding pattern and no leakage when intra-abdominal pressure was increased. However, analysis of laboratory and imaging data was insufficient to determine whether it was an adnexal mass or a urological mass.
Figure 1 Images of computerized tomography urography (CTU). There were no abnormalities in the shape and position of the right kidney, and no dilation of the right ureter. No normal kidney was found in the left renal area (A). An ectopically dysplasia kidney with peripheral enhancement could be seen anterior to fifth lumbar vertebra (B). Spotted contrast media was demonstrated around the ectopic kidney (thick arrow, (B). However, an enlarged uterus can be seen (C) and the thick-walled dysplasia kidney resembles an ovarian cyst (thick arrow, (D).
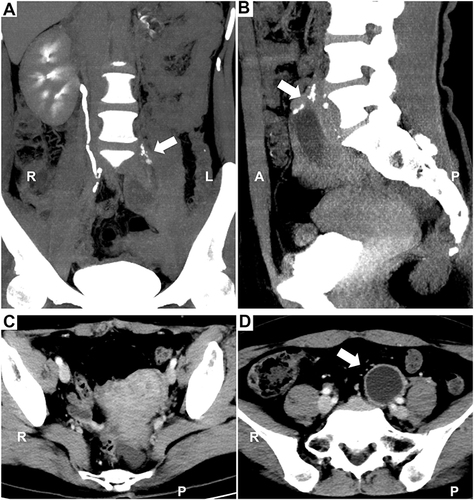
Figure 2 Images of MR. Sagittal turbo spin-echo (TSE) T2-weighted imaging (T2WI) (A-C), coronal T2WI (D-E), and axial T2WI with fat suppression (F). Sagittal and coronal T2WI showed an oval cyst in the right ovary (A and D). Another oval-shaped cystic lesion is observed above the uterus, with a long tubular tortuous downward extension on the left side of the pelvic cavity (B and E). However, careful examination revealed a maldeveloped ureter accompanying the uterus, the end of which was fused with the vagina (C and F). (Arrow: ectopic kidney; dotted line box: ectopic ureter).
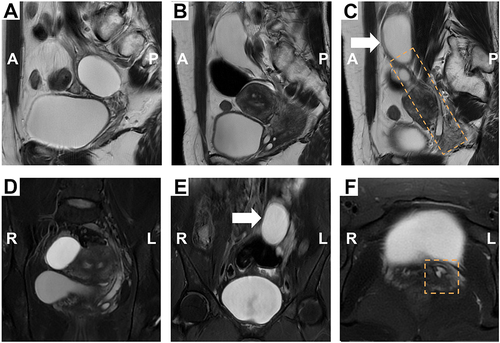
Figure 3 Intraoperative endoscopic data. (A) (a) Laparoscope showed septate uterus. A retroperitoneal cyst was dissociated from left ovary and fallopian tube. (b) The mass, probably be an ectopic kidney (arrow), was separated from surrounding tissue, and the distal end extended to nearby bladder. (B) Cystography imaging showed right ureter opening (dotted box) in bladder (a), but detected no left ureter opening (b).
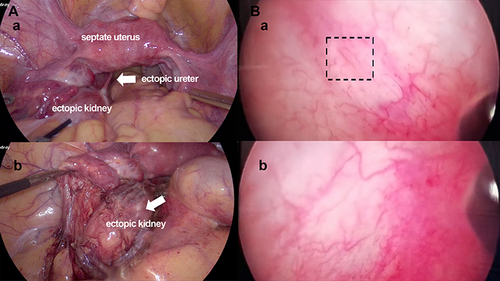
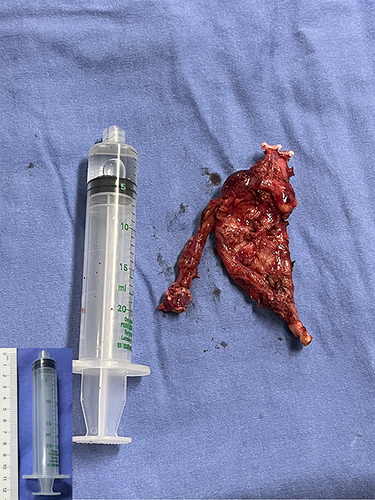
Figure 4 Gross of dysplasia ectopic kidney. Photograph shows the excised kidney with single system ureter.
The patient underwent laparoscopy to achieve the following objectives: 1) investigate the pelvic mass, 2) remove it if necessary and perform a pathological diagnosis, and 3) explore potential causes of urinary dribbling.
Laparoscopy revealed a cystic mass in the left retroperitoneum extending close to the bladder and posterior to the left infundibulopelvic ligament. The mass was highly likely to be an ectopic kidney (). Cystoscopy confirmed the normal positioning of the right ureteral orifice; however, the left orifice was absent(). A dysplastic ectopic kidney with an ectopic ureter draining into the vagina was strongly suspected.
The patient underwent left nephroureterectomy () and experienced complete restoration of urinary continence and disappearance of abdominal pain postoperatively. A pathological specimen confirmed the presence of a pelvic kidney and hydroureter with chronic inflammation. Hypogastric pain could potentially be attributed to ureteritis.
Discussion
In this case, the ectopic kidney was near the left adnexal area, and was very similar with an ovarian cyst on imaging. Because she was misdiagnosed as “solitary kidney” since childhood, over the years, her abdominal pain and urinary incontinence had not been related to congenital urogenital malformations by clinicians. Pelvic kidney is the major type of ectopic kidney.Citation11 Our literature review revealed several cases in which pelvic ectopic kidneys posed diagnostic challenges, as summarized in .Citation12–20 Calculi and pyelonephritis in ectopic kidneys can manifest as lower abdominal pain, fever, nausea, and vomiting, similar to the typical symptoms of acute appendicitis. Additionally, appendicitis can also cause dysuria and positive urine microscopy when the appendix is in close proximity to the bladder, and inflammation spreads.Citation18–20 A hydronephrotic ectopic kidney may be mistaken for a pelvic tumor.Citation13,Citation15,Citation17 In most of the literatures we reviewed, the ectopic kidney was diagnosed by noninvasive examinations and received appropriate treatment. CT and MRI aid in determining the origin of the mass; however, in certain cases, the diagnosis is confirmed during surgery.Citation13,Citation16 Atypical symptoms, signs, and examination of ectopic kidneys often result in misdiagnosis. Small ectopic renal tissues are often mistakenly identified as renal agenesis during ultrasonic evaluation.Citation21
Table 1 Summary of Previous Publication of Ectopic Pelvic Kidney Mimicking Other Diseases
Reports of ectopic vaginal drainage of the ureters combined with ectopic kidneys are rare. We reviewed similar cases in .Citation7,Citation8,Citation21–29 Due to the close embryological interaction between the uropoetic and genital systems, congenital genital tract abnormalities are frequently associated with malformations of the vagina and uterus.Citation21 Similarly, in the present case, the patient had a septate uterus. Surgical correction is crucial for eliminating symptoms and improving the quality of life. Nephroureterectomy is the most common management method in current literature. Clinicians emphasize the importance of considering renal function, associated anomalies, and ectopic ureteral location in decision-making. In case of a non-dysplastic, well-functioning ectopic kidney with a single-system ureter, kidney preservation is possible. Amenu performed re-implantation of the ectopic ureter to the bladder wall,Citation8 which was also reported by Kraft in an earlier study.Citation25 In our specific case, the patient experienced recurring abdominal pain, which may have been caused by recurrence of the urinary tract inflammation. The complete relief of symptoms after the operation and the pathological findings of the hydroureter with chronic inflammation support this hypothesis. Therefore, nephroureterectomy was performed.
Table 2 Reports of Ectopic Kidney Combined with Ectopic Vaginal Ureter Causing Female Urinary Incontinence
Additionally, the patient initially claimed to have been diagnosed with unilateral renal agenesis, which led to the misinterpretation of the imaging results. This serves as a reminder of the importance of carefully collecting and screening medical history. Furthermore, the diagnosis of ectopic ureter can be confirmed by identifying the ureteral orifice within the vaginal mucosal fold. However, despite thorough examination using vaginoscopy, we did not find any ectopic openings within the vagina.
The presence of an ectopic kidney and a single vaginal ectopic ureter in a patient with septate uterus is a rare occurrence that has seldom been reported in the literature. It is important to consider the possibility of the pelvic kidney masquerading as an adnexal mass, as this can be a potential differential diagnosis. Although ultrasound, CT, and MRI can provide valuable imaging data, they may not always yield complete diagnostic information. Therefore, it is essential to consider additional techniques, such as intravenous pyelography, cystourethroscopy, and vaginoscopy, to assist in diagnosis, rule out other potential causes, and avoid unnecessary dilemmas during surgery. Furthermore, 3D-CT imaging can be particularly useful for localizing ectopic ureter into the vagina.Citation27
Our report aims to enrich the clinical experience and raise awareness about the possibility of renal ureteral ectopia in cases with an undistinguishable pelvic mass or unexplained urinary incontinence. “Solitary kidney”, congenital urogenital malformations, urinary incontinence might be hints of ectopic kidney and ureter. In cases in which a female patient presents with recurring abdominal pain and a pelvic mass of unknown origin, it is important to consider the differential diagnosis, particularly focusing on the possibility of an ectopic kidney, especially when urogenital malformations are also present.
Ethics Committee Approval
Institutional review board/ethics committee approval was obtained for this study (reference number: 2023-94). Institutional approval for the publication of the case details was not required.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Disclosure
The authors have no conflicts of interest in this work.
Data Sharing Statement
Data used in the study are available from the corresponding author on request.
Additional information
Funding
References
- Barakat AJ, Rushton HG. SpringerLink. Congenital Anomalies of the Kidney and Urinary Tract: Clinical Implications in Children. 1st ed. Cham: Springer International Publishing: Imprint: Springer; 2016.
- Mikuz G. Ectopias of the kidney, urinary tract organs, and male genitalia. Pathologe. 2019;40(Suppl 1):1–8. doi:10.1007/s00292-018-0505-z
- Cinman NM, Okeke Z, Smith AD. Pelvic kidney: associated diseases and treatment. J Endourol. 2007;21(8):836–842. doi:10.1089/end.2007.9945
- Eid S, Iwanaga J, Loukas M, Oskouian RJ, Tubbs RS. Pelvic Kidney: a Review of the Literature. Cureus. 2018;10(6):e2775. doi:10.7759/cureus.2775
- van den Bosch CM, van Wijk JA, Beckers GM, van der Horst HJ, Schreuder MF, Bokenkamp A. Urological and nephrological findings of renal ectopia. J Urol. 2010;183(4):1574–1578. doi:10.1016/j.juro.2009.12.041
- Yilmaz E, Simsek Y, Karaer A, et al. Ectopic Pelvic Kidney Mimicking Adnexal Mass: a Case Report. J Turkish Soc Obstetric Gynecol. 2012;9(3):170–172. doi:10.5505/tjod.2012.14238
- Hussen NB, Kumsa ID, Gebreamlak AL. Detection and management of a case of single system ectopic ureteral insertion to vagina with atrophic ectopic kidney. Int J Surg Case Rep. 2023;106:108234. doi:10.1016/j.ijscr.2023.108234
- Amenu D, Asmare A, Siraj A. Congenital ureterovaginal fistula: a rare case of single-system ectopic ureter with ipsilateral ectopic kidney managed by vaginal approach: a case report. J Med Case Rep. 2021;15(1). doi:10.1186/s13256-021-03157-x
- Demir M, Ciftci H, Kilicarslan N, et al. A case of an ectopic ureter with vaginal insertion diagnosed in adulthood. Turk J Urol. 2015;41(1):53–55. doi:10.5152/tud.2014.81567
- Agha RA, Franchi T, Sohrabi C, Mathew G, Kerwan A, Group S. The SCARE 2020 Guideline: updating Consensus Surgical CAse REport (SCARE) Guidelines. Int J Surg. 2020;84:226–230.
- Orlandi G, Toscano P, Gabrielli O, et al. Prenatal Diagnosis of an Intrathoracic Left Kidney Associated with Congenital Diaphragmatic Hernia: case Report and Systematic Review. J Clin Med. 2023;12(11):3608. doi:10.3390/jcm12113608
- Infante JR, Gonzalez FM, Vallejo JA, Torres M, Pacheco C, Latre JM. False-positive results of a gastrointestinal bleeding study caused by an ectopic kidney. Clin Nucl Med. 2000;25(8):645–646. doi:10.1097/00003072-200008000-00024
- Malhotra N, Roy KK, Garg PK, Takkar D. Ectopic hydronephrotic kidney masquerading as an ovarian cyst during pregnancy. Eur J Obstet Gyn R B. 2001;97(2):239–240. doi:10.1016/S0301-2115(00)00516-9
- Reddy MP, Malik A, Zamani R, Lilien DL. Obstructed ectopic kidney mimicking Chilaiditi syndrome on F-18 FDG imaging. Clin Nucl Med. 2003;28(8):687–690. doi:10.1097/01.rlu.0000079660.49548.cf
- Pryma DA, Akhurst T. Hydronephrotic ectopic pelvic kidney simulates sacral metastasis from breast cancer. Clin Nucl Med. 2005;30(4):244–245. doi:10.1097/01.rlu.0000156373.03235.92
- Blackmon KN, Rao AG. Ectopic kidney mimicking a Meckel’s diverticulum on Tc-99m pertechnetate scan. Clin Nucl Med. 2011;36(12):e228–30. doi:10.1097/RLU.0b013e31821c9ae9
- Yadav R, Kataria K, Balasundaram P, Karak AK. Mucinous cystadenocarcinoma arising in an ectopic kidney simulating a retroperitoneal dermoid cyst: a rare tumour presenting as a diagnostic dilemma. Malay J Pathol. 2013;35(1):95–98.
- Taylor D, Steen C. Unilateral ectopic kidney mimicking acute appendicitis: a case study. ANZ J Surg. 2019;89(11):1520–1521. doi:10.1111/ans.14970
- Xu YE, Hendahewa R. A rare presentation of an ectopic kidney with pyelonephritis mimicking appendicitis. J Surg Case Rep. 2019;2019(11):rjz342. doi:10.1093/jscr/rjz342
- Manglik A, Tomar L, Akash A. Pyelonephritis of an ectopic right kidney pretending as acute appendicitis: an unusual case. Int J Surgery Case Rep. 2022;98.
- Chen S, Zhu L, Yang S, Tan J. Y-type partial duplication of a vaginal ectopic ureter with ipsilateral hypoplastic pelvic kidney and bicornuate uterus. Singapore Med J. 2013;54(6):e135–7. doi:10.11622/smedj.2013116
- Gharagozloo AM, Lebowitz RL. Detection of a poorly functioning malpositioned kidney with single ectopic ureter in girls with urinary dribbling: imaging evaluation in five patients. AJR Am J Roentgenol. 1995;164(4):957–961. doi:10.2214/ajr.164.4.7726056
- Ng JW, Yeung CK, Liu KK. Laparoscopic excision of pelvic kidney with single vaginal ectopic ureter. J Pediatr Surg. 1998;33(11):1731–1732. doi:10.1016/S0022-3468(98)90643-1
- Sameshima H, Nagai K, Ikenoue T. Single vaginal ectopic ureter of fetal metanephric duct origin, ipsilateral kidney agenesis, and ipsilateral rudimentary uterine horn of the bicornuate uterus. Gynecol Oncol. 2005;97(1):276–278. doi:10.1016/j.ygyno.2004.12.012
- Kraft KH, Molitierno JA, Kirsch AJ. Ten-year-old girl with crossed-fused ectopic kidney and ectopic ureter to vagina. Urology. 2007;70(6):1220–1221. doi:10.1016/j.urology.2007.09.063
- Kumar S, Mandal A, Acharya N, Jain V, Kalra J, Singh S. Congenital vesicovaginal fistula with transverse vaginal septum and ectopic ureter opening in proximal vagina: case report and brief review. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18(8):959–961. doi:10.1007/s00192-006-0258-8
- Iwatsuki S, Kojima Y, Imura M, Mizuno K, Kohri K, Hayashi Y. Detection of ectopic ureteral insertion to vagina with hypoplastic ectopic kidney by three-dimensional computed tomography. Urology. 2009;73(3):505–506. doi:10.1016/j.urology.2008.09.012
- Lin VC, Weng HC, Kian-Lim E, Lin IC, Yu TJ. An atrophic crossed fused kidney with an ectopic vaginal ureter causing urine incontinence. Urology. 2010;76(1):55–56. doi:10.1016/j.urology.2009.09.042
- Zhang A, Zeng X, Woo JJ, Morrell M, Xu D. An unusual case of Herlyn-Werner-Wunderlich syndrome with a complete septate uterus and complicated urinary tract with rare ectopic ureteral opening. Int J Gynaecol Obstet. 2018;143(2):248–250. doi:10.1002/ijgo.12578