
Abstract
Background
The problem of maternal mental health is a priority issue of global concern. Dyadic coping refers to the co-managing and making decisions between two parties in response to a joint stressful event. At present, china has limited focus on dyadic coping for pregnant women during pregnancy. This study aimed to investigate different categories and characteristics of dyadic coping in pregnant women throughout pregnancy and to analyze the factors that influence these categories.
Methods
This study was a cross-sectional, and 376 pregnant women who visited the obstetric clinic at a tertiary hospital in Sichuan province from June to September 2023 were interviewed face-to-face using convenience sampling. Data were collected using a sociodemographic questionnaire, dyadic coping scale, and family adaptability and cohesion evaluation scale. The data were imported into excel and exported to spss 27.0 to analyze the potential characteristics of pregnant women’s dyadic coping during pregnancy and to explore the effects of this using univariate analysis and multifactorial logistic regression.
Results
A total of 376 valid questionnaires were collected. The results of the potential profile analysis showed that the dyadic coping of pregnant women during pregnancy could be categorized into three different groups: the “low coping group” (21.3%), the “general coping group” (67.5%), and the “high coping group” (11.2%). Multiple logistic regression analyses revealed that low monthly family income, early pregnancy, primipara, family adaptability and cohesion were the factors influencing the dyadic coping of pregnant women during pregnancy.
Conclusion
During pregnancy, pregnant women exhibit moderate levels of dyadic coping. Three different categories of dyadic coping patterns were exhibited: low coping group, general coping group, and high coping group, with significant heterogeneity. Therefore, there is a need to focus on the dyadic coping status of various categories of pregnant women and implement targeted couple and family-wide interventions.
Introduction
The health of women during pregnancy, childbirth, and the newborn period is essential for the future of families and societies. The global population is aging markedly, and the total fertility rate is declining steadily.Citation1 The same situation exists in China.Citation2 With the liberalization of China’s fertility policy and shifts in families’ perceptions of parenthood, the clinical characteristics and stressful situations experienced by pregnant women have become more intricate.Citation3 Consequently, the mental health of pregnant women deserves greater attention. Pregnancy is a significant period and particular stage in a woman’s life, bringing joy to the family and a series of challenges. Due to physical, psychological, and work-family conflicts, pregnant women often experience stress during pregnancy, which can lead to negative emotions such as psychological distress, anxiety, and depression.Citation4 According to the World Health Organization (WHO), nearly 1 in 5 women experience mental health problems during pregnancy, with depression being the most prominent and neglected issue.Citation5 Globally, the prevalence of prenatal depression among pregnant women ranges from 15% to 65%.Citation6 The prevalence of prenatal anxiety ranges from 6% to 57%.Citation7 A study in China showed that the prevalence of prenatal depression, anxiety, and depression combined with anxiety were 25.2%, 27.9%, and 18.6%, respectively.Citation8 Inappropriate coping with these negative emotions not only affects the health status of the pregnant woman, but also poses a risk to the health of the offspring,Citation9 the relationship of the couple,Citation10 and the functioning of the family.Citation11 Research has shown that lack of family support and spouse support are risk factors for prenatal depression and anxiety,Citation12,Citation13 while good family relationships are protective factors for prenatal depression.Citation14
Dyadic coping is a novel concept in the field of psychological stress research, with significant implications for mental health,Citation15 marital relationship,Citation16 and overall quality of life.Citation17 According to the Systemic Interaction Model, the process by which couples jointly manage stress when faced with a joint stressful event is known as dyadic coping.Citation18,Citation19 Dyadic coping consists of two forms: positive and negative coping. Positive dyadic coping includes supportive, delegation, and joint coping, while negative dyadic coping includes ambivalent and hostile coping. During the particular period of pregnancy, dyadic coping between couples is a complex process that may be affected by various factors. Liu et alCitation3 summarized that gender, education level, economic status, marital satisfaction, age at marriage, whether it is the first marriage, and cultural background can influence the dyadic coping of pregnant couples. Family factors are critical factors affecting dyadic coping.Citation20 Family is an important environment that influences an individual’s physical and mental development, and family functioning will affect the level of dyadic coping, mental health, and quality of life of couples.Citation21,Citation22 In China, family relationships are emphasized more than in Western countries. However, it is unclear whether support from parents and other family members influences pregnant women’s dyadic coping. Therefore, this study will investigate whether family relationships in China play a role in influencing pregnant women’s dyadic coping.
Research indicates that women tend to express stress more frequently than men during pregnancy.Citation16 Pregnant women often feel that they offer more dyadic coping support but receive inadequate support in managing stress jointly.Citation23 Early research found that men tended to focus on problem-centered coping strategies, while women tended to prefer emotion-centered coping.Citation24 Therefore, it is crucial to investigate pregnant women’s perceptions of dyadic coping, particularly when the level of support and coping provided by their spouse differs from what they expect.
Currently, there is insufficient attention paid to dyadic coping among pregnant women in China, and the current status of dyadic coping is unclear. Existing assessments of dyadic coping levels in pregnant women primarily rely on overall scale scores, overlooking the individual differences within groups of pregnant women. Latent profile analysis groups individuals with similar responses into the same category to determine latent characteristics based on the responses of different categories on scale entries and provide insight into the distribution of different categories in the entire dataset. Therefore, with the pregnant women population as the research object, this study aims to analyze the categories of dyadic coping, explore the relationship between different types of dyadic coping groups and various sociodemographic factors, as well as explore the relationship between family adaptability and cohesion to provide theoretical references to improve the dyadic coping ability of pregnant women and to adopt scientific and practical individualized intervention measures.
Materials and Methods
Design
This study utilized a cross-sectional design and was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Study Population
The convenience sampling method was used for the study. During the study period from June 2023 to September 2023, pregnant women who attended prenatal checkups at the outpatient obstetric clinic of a tertiary general hospital in Chengdu, Sichuan Province. The inclusion criteria for this study population were as follows: 1) no previous history of mental illness and clear mental state; 2) 18 years or older; 3) informed consent and voluntary participation. The exclusion criteria were as follows: 1) significant physical and psychological trauma during pregnancy; 2) individuals with severe pregnancy complications or high-risk pregnancies; and 3) incomplete questionnaire information.
Sampling
This study 19 research variables were formulated based on the literature review. The sample size was calculated by taking 10 to 15 times the number of research variablesCitation25 and considering 20% of invalid questionnaires; the total sample size was determined to be at least 228 to 342 cases.
Variables
Dependent variables
Dyadic Coping.
Independent Variables
Sociodemographic characteristics include age, education level, employment status, current residence, monthly per capita family income, pregnancy status, gestational week, whether pregnancy is planned or not, marital status, marrying age, marital harmony, and presence of co-morbidities.
Family Adaptability and Cohesion Evaluation Scale
Operational Definition
Dyadic Coping.
Dyadic coping refers to the process of jointly managing and making decisions by both partners in response to shared stressful events (eg, pregnancy and childbirth).Citation9,Citation10
Instruments
Sociodemographic Questionnaire
The study was designed by the researcher and included the following variables: age, education level, employment status, current residence, monthly per capita family income, pregnancy status, gestational week, whether pregnancy is planned or not, marital status, marrying age, marital harmony, and presence of co-morbidities.
Dyadic Coping.
Bodenmann et alCitation26 developed the scale in 2008 and adapted it for Chinese culture by Chinese scholars Xu et alCitation27 in 2016. This Chinese version has demonstrated good reliability and validity, making it suitable for evaluating the coping abilities of Chinese couples when dealing with stress.The scale includes six dimensions of stress communication, supportive coping, delegated coping, joint coping, negative coping, and coping quality evaluation, with 37 items. The four dimensions of stress communication, supportive, delegated, and negative coping, encompass individual-perceived self-coping and spousal coping. The joint coping dimension includes joint coping as perceived by both spouses. The study utilized a 5-point Likert scale, with “rarely” to “very frequently” assigned values of 1 to 5 points. Negative coping was scored inversely, and the two entries for coping quality evaluation dimensions were excluded from the total score. The scale’s total score ranged from 35 to 175, with a higher score indicating a higher level of dichotomous coping. The critical scores for dyadic coping are categorized as follows: dyadic coping with a low average (total score: <111), dyadic coping in the mid-level range (total score: 111–145), and dyadic coping with a high average (total score: >145). The Cronbach’s alpha coefficient of the scale in this study was 0.928.
Family Adaptability and Cohesion Evaluation Scale, Second Edition.
The scale was compiled by Olson et alCitation28 in 1982. Chinese scholars Fei et alCitation29 adapted it into Chinese in 1991. This Chinese version has demonstrated good reliability and validity, making it suitable for assessing the adaptability and closeness of Chinese families. The scale was divided into two subscales, family closeness, and family adaptability, with 30 items. A 5-point Likert scale was utilized, with 1 to 5 indicating “never” to “always”, resulting in a total score ranging from 30 to 150. Higher scores indicate a greater sense of closeness and adaptability among family members. The Cronbach’s alpha coefficient of the scale in this study was 0.925.
Ethical Considerations
This study was reviewed by the Ethics Committee of Sichuan Academy of Medical Sciences-Sichuan Provincial People’s Hospital (2023–318). The study adheres to the Declaration of Helsinki. All participants will receive information about the study from the informed consent form and sign it after agreeing to participate.
Data Collection and Quality Control
The research team interviewed pregnant women undergoing prenatal examinations at the obstetric clinic. Before starting the formal survey, the research team contacted the head of the hospital’s obstetric clinic to explain the survey’s purpose and obtain their consent. Subsequently, the two research team members responsible for data collection and supervision received one day of training on the data collection process and handling. Before starting the survey, the two researchers conducted face-to-face interviews with the participants to explain the study’s purpose, significance, methodology, and confidentiality principles. After obtaining informed consent from the study participants, two research team members instructed the participants to complete three questionnaires: the Sociodemographic Questionnaire Scale, the Dyadic Coping Scale, and the Family Adaptability and Cohesion evaluation scale. To ensure data completeness and consistency, two research team members will review and check the collected data at the time of questionnaire collection, and incomplete questionnaires will be excluded. Valid questionnaire data will be entered into Excel by two researchers and verified for accuracy by a third researcher to ensure data completeness and consistency.
Data Analysis
Mplus 8.3 software was utilized to conduct potential profile analysis. The fit metrics for the potential profile model included the following: Information evaluation metrics such as the Akaike Information Criterion (AIC), the Bayesian Information Criterion (BIC), and the Adjusted Bayesian Information Criterion (aBIC) were used to assess the model fit. Smaller statistical values indicate a better fit. Classification evaluation metrics: The accuracy of the classification was assessed using information entropy (Entropy), which ranges from 0 to 1. The value of ≥ 0.80 indicates that more than 90% of the cases were correctly classified, demonstrating high classification accuracy and a good model fit. In addition, the closer the value is to 1, the more accurate the classificationCitation30 is. (iii) Likelihood ratio test: The Lomondale-Ruben corrected likelihood ratio test (LMR) and the Bootstrap-based likelihood ratio test (BLRT) were used to compare the goodness of fit of k-1 and k-class models. A P-value of less than 0.05 for LMR and BLRT indicates that the k-category model outperforms the k-1-category model.Citation31 In this study, the findings of each model were summarized to identify the best model. The evaluation of the above metrics was solely used as a reference for making profile decisions. It is also essential to consider the interpretability of each category when determining the best model.
SPSS 27.0 software was utilized for data analysis. Measurement information was presented as mean ± standard deviation and one-way ANOVA was employed for group comparisons. Count information was presented using frequency and percentage, and group comparisons were conducted using the chi-square or rank-sum tests. Unordered multicategorical logistic regression analysis was conducted using the variables found to be statistically significant by one-way analysis as independent variables and potential profiles as dependent variables. The test’s significance level (α) was set at 0.05 for all two-sided tests, and differences were considered statistically significant at P < 0.05.
Results
Participant Characteristics
Four hundred pregnant women participated in this survey, and 376 questionnaires were successfully recovered, resulting in an effective recovery rate of 94%. Most pregnant women (45.2%) fell within the 26–30 age range out of 170 cases. Regarding education, 132 cases (35.1%) were from college, and 167 (44.4%) were from bachelor’s degree programs. The dominant work unit was enterprise units, accounting for 105 cases (27.9%). The percentage is shown in , and the remaining information is also presented there.
Table 1 Description of Demographic Data(N=376)
Table 2 Characteristics of Studies on Potential Profiles of Dyadic Coping in Pregnant Women During Pregnancy (N = 376)
Table 3 Average Attribution Probability of Individuals Across Various Potential Categories (%)
Table 4 Demographic and Characteristics by Latent Profile (N=376)
Table 5 Multifactor Analysis of Potential Categories of Binary Coping in Pregnant Women During Pregnancy
Results of a Potential Characterization of Dyadic Coping in Pregnant Women During Pregnancy
The total dyadic coping score of pregnant women was (131.19 ± 16.72). An exploratory potential profile analysis was conducted by creating a 1–5 potential profile model using the standardized means of the five dimensions of the dyadic coping scale as exogenous indicators. The results are presented in . As the number of profiles increased, the Entropy value consistently exceeded 0.7. The AIC, BIC, and aBIC values of the models decreased gradually as the number of profiles increased, with the 5-category model having the smallest value, followed by the 4-category model. However, the LMR test values of the models from category 4 to 5 did not reach statistical significance (P > 0.05). Entropy values were highest at category 3, and both the LMR and BLRT test values were statistically significant (P < 0.05). The attribution probability matrix for the three potential profile categories indicates that the average probability of each potential category being attributed to the category is between 91% and 95.5%, suggesting that the model for the three potential categories is highly reliable (). Therefore, after considering the fit indices of the model and the actual clinical significance, we concluded that the potential profile model with three categories was the optimal model for dyadic coping in pregnant women during pregnancy. The potential profiles were plotted based on the results of the categorization into three potential categories and are shown in .
Figure 1 Characteristics of the three potential categories of dyadic coping in pregnant women during pregnancy.
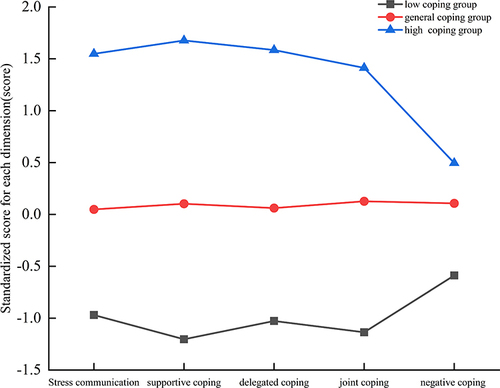
Upon analyzing the scores of each category, it was observed that the overall dyadic coping scores and the scores of each dimension increased progressively from Category 1 to Category 3. The overall score of each dimension in category 1 was lower than the other two groups, referred to as the low coping group, accounting for 21.3%. The overall score of each dimension in Category 2 fell between Category 1 and Category 3, with the scores of each dimension showing more stable fluctuations, referred to as the general coping group, accounting for 67.5%. The overall score of Category 3 was higher than the average and significantly higher than that of Category 1 and Category 2, referred to as the high coping group, accounting for 11.2%.
Univariate and Multifactorial Analysis of Potential Categories of Dyadic Coping in Pregnant Women During Pregnancy
The ANOVA and χ²-test showed statistically significant differences between the three profiles differed statistically in terms of per capita monthly family income, pregnancy status, gestational cycle, and family adaptability and cohesion, shows a summary of the results.
An unordered multicategorical logistic regression model was constructed for multifactorial analysis using ANOVA and χ² identified variables with statistically significant differences. The three potential categories of dyadic coping in pregnant women during pregnancy were used as dependent variables (“low coping group” was used as a reference) to find predictors associated with dyadic coping. As shown in , the study results indicated statistically significant differences among the three categories regarding per capita monthly family income, pregnancy status, pregnancy cycle, family closeness and adaptability (P < 0.05).
Discussion
The study found that pregnant women had a moderate level of dyadic coping during their pregnancy, with a score of 131.19 ± 16.72. This score is higher than other related studies have reported.Citation16,Citation32,Citation33 This may be attributed to the fact that this study included the entire group of pregnant women throughout their pregnancy, with a higher percentage in early and mid-pregnancy and fewer pregnant women with concurrent pregnancy complications, resulting in an overall better level of dyadic coping. The inconsistency in the analysis may be attributed to the fact that dyadic coping can be associated with the number of pregnancies and the different trimesters. Molgora et alCitation16 found that first-time pregnant women may exhibit lower dyadic coping in late pregnancy due to reasons such as fear of labour and delivery during their first delivery. Tan et alCitation32 mentioned that pregnant women in their second pregnancy may also exhibit lower couple coping skills due to low self-efficacy and pregnancy stress. In addition, the mental health status of pregnant women during pregnancy may also affect their dyadic coping ability. Li et alCitation33 showed that pregnant women with comorbid anxiety and depressive symptoms may exhibit lower dyadic coping ability. The dyadic coping ability of pregnant women during pregnancy is influenced by multiple factors, including the stage of pregnancy, number of pregnancies, and mental health status. Future research could further explore ways to enhance dyadic coping abilities in pregnant women to enhance maternal mental health and well-being during pregnancy.
Potential profile analysis revealed three different categories of dyadic coping: “low coping group”, “general coping group”, and “high coping group”, highlighting the individual heterogeneity of pregnant women during pregnancy. Among them, the low coping group accounted for 21.3%. This group of pregnant women was mainly characterized by having less than a tertiary education and being aged 30 years and above. This may be related to the fact that pregnant women with lower levels of education and their spouses have limited knowledge and a negative attitude toward health information during pregnancy. They also have less understanding of labor and delivery and tend to respond to problems negatively, increasing their fear of labor and delivery. Studies have shown that pregnant women with lower levels of education are more likely to experience fear of childbirth.Citation34 Additionally, fear of childbirth has been associated with poorer adjustment between couples,Citation35 leading to lower levels of coping. With the relaxation of China’s fertility policy, pregnant women aged 30 years or older are increasingly becoming multipara at an advanced age. Compared to pregnant women who are not seniors, senior pregnant women are more likely to experience pregnancy complications and comorbidities,Citation36 which increases the risk of psychological issues such as anxiety and depression.Citation37 Pregnant women with higher anxiety and depression scores are more likely to use negative coping strategiesCitation38 and have a lower level of adaptive coping. Secondly, the high coping group accounted for 11.2%, mainly characterized by higher education and higher family income. Higher levels of education and family income were associated with increased support for pregnant women.Citation32 This, in turn, led to a more scientific and rational approach to problem-solving and a greater tendency to adopt positive coping strategies, such as effective communication, ultimately enhancing their ability to cope.
The study found that lower per capita monthly family income is a risk factor for dyadic coping, which aligns with previous research.Citation39 This suggests that economic status may affect the coping ability of pregnant women. Low-income families may experience increased economic stress and limited resources, leading to pregnant women lacking the essential support and means to deal with the diverse challenges during pregnancy. Research shows that pregnant women with lower per capita monthly household income experience higher levels of stress than those with better financial situations.Citation40 Moreover, financial stress negatively affects positive spouses affect,Citation41 which reduces the ability to provide social and emotional support to spouse and increases destructive behaviors. This situation, in turn, leads to decreased supportive dichotomous coping provided by spouses. Additionally, research has shown that having more children and experiencing financial stress can also result in a decrease in supportive coping by the partner.Citation42 Therefore, low per capita monthly household income and financial strain are linked to dyadic coping strategies in couples. These findings highlight the importance of economic factors in the mental well-being of pregnant women and provide a valuable foundation for future research and intervention.
Logistic regression analysis found that women who were pregnant for primigravid were more likely to belong to the high-coping group during pregnancy. The possible reasons are as follows: Firstly, it could be related to the fact that primigravid are educated about the labor process and potential pain during pregnancy, which may make them better prepared to cope with labor. Several studies have shown that providing group psychoeducational interventions and simulation-based childbirth education can alleviate the fear of childbirth and increase self-efficacy in childbirth among primigravid.Citation43,Citation44 Additionally, high levels of dyadic coping primigravid may be associated with supportive spousal coping, which serves as a protective factor for couples dealing with stress.Citation45 Couples’ shared coping strategies during pregnancy can alleviate their stress, boost their confidence in parenting, and foster a deeper sense of trust and intimacy with each other.Citation16 Brandao et alCitation17 have discovered that spouse’ positive joint coping can enhance pregnant women’s marital satisfaction, subsequently leading to an improved quality of life for pregnant women. Secondly, family members are more likely to support parenting events than other illness-related stressors, especially for primigravid.Citation3 This support can benefit the couples’ relationship, coping skills, and resources. Therefore, it is important to emphasize spousal and family member support as high levels of support enable primigravid to cope more easily with the various challenges of pregnancy, better adapt to motherhood, and improve their coping abilities.
Our study found that early pregnancy is a risk factor for dyadic coping in pregnant women. Early pregnancy is considered a vulnerable period during which couples are challenged by shifting responsibilities, changing roles, and psychosocial distress.Citation46 Pregnant women are more likely to experience anxiety and depression in early pregnancy than in mid and late pregnancy due to factors such as changes in hormone levels, feelings of uncertainty and nervousness about the pregnancy, and concerns about the health of the fetus.Citation47 The mental health of the partner during pregnancy is closely related to this. Studies have found that pregnant women experiencing high levels of depression perceive themselves and their spouse as providing less supportive coping and more negative coping to each other.Citation38 Supportive spouse are central to women’s mental health during pregnancy.Citation48 Lack of support from a spouse, ineffective coping strategies, and intra-spousal conflict during pregnancy are significant factors that impact mental health during this time.Citation49 These factors may contribute to poor psychological adjustment and family stress. Therefore, it is crucial for pregnant women and their spouse in early pregnancy to establish a strong spousehip and provide timely mental health support to prevent and cope with mental health problems during pregnancy.
Finally, this study found that family adaptability and cohesion were protective factors for dyadic coping, consistent with other studies’ findings.Citation20 This suggests that a supportive family environment and positive family relationships can enhance pregnant women’s coping skills, potentially reducing the stresses and challenges they may encounter during pregnancy. This also highlights the significance of family support and close relationships in conjunction with individual factors affecting pregnant women, positively impacting their mental health and overall well-being. Pregnant women are in a stress-sensitive period during pregnancy, and both positive and negative family relationships can influence their stress levels. Family adaptability and closeness are crucial indicators of family functioning, reflecting the intimacy among family members and the family’s capacity to cope with critical events.Citation50,Citation51 Studies have shownCitation20 that family adaptability and closeness are positively correlated with dyadic coping, indicating that the better the relationship between family members, the greater the family adaptability and closeness, and the higher the level of dyadic coping; meanwhile, higher family support can reduce the fear of labor and delivery,Citation52 which is conducive to improving the adjustment between couples.Citation53 To enhance the psychological well-being of pregnant women, healthcare professionals should support them in building solid relationships with their spouses and other family members. Additionally, they should assist women in adjusting to their new roles and making psychological adaptations to promote healthy family dynamics. Family members, in turn, should offer understanding, care, and various forms of support, including material, emotional, and informational support, to pregnant women.
The Clinical Implication of this Study.
Against the backdrop of significant population aging and low fertility rates in China, along with changes in family attitudes toward child-rearing, pregnant women are encountering increasingly complex challenges and heightened levels of stress, making them more susceptible to negative emotions. The results of this study demonstrate different categorical characteristics in pregnant women’s dyadic coping abilities during pregnancy. This finding is valuable for medical professionals and family members in identifying the coping patterns and influencing factors among pregnant women in different pregnancy categories. It also emphasizes the need to integrate resources for effective coping into the assessment of pregnant women, particularly those with lower literacy levels and those in the early stages of pregnancy. This approach aims to offer more opportunities for relevant health education and to underscore the significance of mutual support between spouses in coping with pregnancy. Ultimately, it seeks to enhance the coping abilities of pregnant women.
Limitations
This study was conducted at a single tertiary general hospital in China using a convenience sampling method. However, it did not take into account the variations in economic development across different regions and hospital levels. This may have resulted in sample bias and limited the generalizability of the results. Therefore, future investigations should involve a multi-center sample. Moreover, all questionnaires were self-reported, which may lead to bias in self-reporting. Additionally, this study was a cross-sectional survey, which did not observe the dynamics of postpartum maternal coping strategies and did not explain the causal relationship. Therefore, a longitudinal study should investigate the changes in maternal dyadic coping throughout pregnancy and elucidate the causal relationship. This will provide a foundation and guidance for future intervention studies.
Conclusion
This study found that the overall dyadic coping of pregnant women during pregnancy was at a moderate level and was categorized into three potential categories: low coping group, general coping group, and high coping group. Low monthly family income and early pregnancy are risk factors for the low coping group, primipara is a protective factor for the high coping group, and family adaptability and cohesion are protective factors for both the general coping group and the high coping group.The findings offer a basis for investigating intervention strategies to enhance coping mechanisms among pregnant women during pregnancy. It is essential to pay more attention to the psychological well-being of pregnant women and the supportive factors provided by their spouses and families.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors report no conflicts of interest in this work.
Acknowledgments
We would like to thank the pregnant women who participated in this study for their time and patience. Without their participation, the project would not have been possible.
Data Sharing Statement
Data will be available from the corresponding author upon request.
Additional information
Funding
References
- Vollset SE, Goren E, Yuan CW, et al. Fertility, mortality, migration, and population scenarios for 195 countries and territories from 2017 to 2100: a forecasting analysis for the Global Burden of Disease Study. Lancet. 2020;396(10258):1285–1306.
- Qiao J, Wang Y, Li X, et al. A Lancet Commission on 70 years of women’s reproductive, maternal, newborn, child, and adolescent health in China. Lancet. 2021;397(10293):2497–2536.
- Liu MJ, Fang Y, Niu TC, et al. Research status and prospect of dyadic coping in pregnant women and their spouses. Chin Nurs Manag. 2023;23(02):303–307.
- Yang SY, Zeng TY, Li BB, et al. Research progress of maternal role transition. J Nurs Chin. 2023;38(20):126–129.
- World Health Organization. WHO guide for integration of perinatal mental health in maternal and child health services[EB/OL]. Available from: https://www.who.int/publicationsdetail-redirect/9789240057142. Accessed May 25, 2024.
- Dadi AF, Miller ER, Bisetegn TA, et al. Global burden of antenatal depression and its association with adverse birth outcomes: an umbrella review. BMC Public Health. 2020;20(1):173.
- Ma X, Wang Y, Hu H, et al. The impact of resilience on prenatal anxiety and depression among pregnant women in Shanghai. J Affect Disord. 2019;250:57–64.
- Yang H, Pan Y, Chen W, et al. Prevalence of and relevant factors for depression and anxiety symptoms among pregnant women on the eastern seaboard of China in the post-COVID-19 era: a cross-sectional study. BMC Psychiatry. 2023;23(1):564.
- Chhabra J, Li W, McDermott B. Predictive Factors for Depression and Anxiety in Men During the Perinatal Period: a Mixed Methods Study. Am J Mens Health. 2022;16(1):15579883221079489.
- Hamidia A, Kkheirkhah F, Faramarzi M, et al. Depressive symptoms and psychological distress from antenatal to postnatal period in women with high-risk pregnancy: a prospective study during the COVID-19 pandemic. Indian J Psychiatry. 2021;63(6):536–542.
- Pawlby S, Hay DF, Sharp D, et al. Antenatal depression predicts depression in adolescent offspring: prospective longitudinal community-based study. J Affect Disord. 2009;113(3):236–243.
- Roy U, Swain D. A prospective cohort study to assess the prevalence and risk factors of antepartum depression and its effect on maternal and fetal outcome. Asian J Psychiatr. 2024;91:103873.
- Kang YT, Yao Y, Dou J, et al. Prevalence and Risk Factors of Maternal Anxiety in Late Pregnancy in China. Int J Environ Res Public Health. 2016;13(5):468.
- Míguez MC, Vázquez MB. Risk factors for antenatal depression: a review. World J Psychiatry. 2021;11(7):325–336.
- Landolt SA, Weitkamp K, Roth M, et al. Dyadic coping and mental health in couples: a systematic review. Clin Psychol Rev. 2023;106:102344.
- Molgora S, Acquati C, Fenaroli V, et al. Dyadic coping and marital adjustment during pregnancy: a cross-sectional study of Italian couples expecting their first child. Int J Psychol. 2019;54(2):277–285.
- Brandão T, Brites R, Hipólito J, et al. Dyadic coping, marital adjustment and quality of life in couples during pregnancy: an actor-partner approach. J Reprod Infant Psychol. 2020;38(1):49–59.
- Bodenmann G. Dyadic coping: a systemic-transactional view of stress and coping among couples:theory and empirical findings. Eur Rev Appl Psychol. 1997;47(2):137–141.
- Bodenmann G. Dyadic coping and its significance for marital functioning.Couples coping with stress: emerging perspectives on dyadic coping. Am Psychol Assoc. 2005;33–49.
- Tang N, Jia Y, Zhao Q, et al. Influencing Factors of Dyadic Coping Among Infertile Women: a Path Analysis. Front Psychiatry. 2022;13:830039.
- Zhou ES, Kim Y, Rasheed M, et al. Marital satisfaction of advanced prostate cancer survivors and their spousal caregivers: the dyadic effects of physical and mental health. Psycho oncology. 2011;20(12):1353–1357.
- Song L, Tan X, Bredle J, et al. Psychometric properties of the FACT-G quality of life scale for family caregivers of cancer patients. Qual Life Res. 2020;29(8):2241–2252.
- Meier F, Milek A, Rauch-Anderegg V, et al. Fair enough? Decreased equity of dyadic coping across the transition to parenthood associated with depression of first-time parents. PLoS One. 2020;15(2):e0227342.
- Molgora S, Fenaroli V, Acquati C, et al. Examining the Role of Dyadic Coping on the Marital Adjustment of Couples Undergoing Assisted Reproductive Technology (ART). Front Psychol. 2019;10:415.
- Wei L, Zhang BY, Luo LP, et al. Potential profile analysis of social participation in elderly patients with chronic obstructive pulmonary disease in community. Mil Nurs. 2019;40(08):6–9.
- Gmelch S, Bodenmann G, Meuwly N, et al. Dyadic Coping Inventory (DCI): a questionnaire assessing dyadic coping in couples. Zeitschrift fur Familienforschung. 2008;20(2):185–202.
- Xu F, Hilpert P, K RA, et al. Validation of the Dyadic Coping Inventory with Chinese couples:factorial structure, measurement invariance, and construct validity. Psychol Assess. 2016;28(8):e127–140.
- Michael RPMD, Charles LWPD, Qijie SMD, et al. Comparison of schizophrenic patients’families and normal families in China, using Chinese versions of FACES-II and the Family Environment Scales. Fam Proc. 1998;37(1):95–106.
- Fei LP, Shen QJ, Zheng YP, et al. Preliminary evaluation of Family Intimacy and Adaptability Scale and Family Environment Scale: a comparative study of normal families and family members with schizophrenia. Chin Ment Health J. 1991;05:198–202+238.
- Wang M, Qiaowen D, Xiangyang BI, et al. Performance of the entropy as an index of classification accuracy in latent profile analysis: a Monte Carlo simulation study. Acta Psychologica Sinica. 2017;49(11):1473.
- Mai Y, Wu YJ, Huang Y. What Type of Social Support Is Important for Student Resilience During COVID-19? A Latent Profile Analysis. Front Psychol. 2021;12:646145.
- Tan Y. Analysis on dual coping and influencing factors of pregnant women with second child and their spouses. Dalian: Dalian Medical University. 2021.
- Li JH. The relationship between dualistic coping and anxiety and depression symptoms in patients with pregnancy complications and their spouses. Jinan: Shandong University. 2020.
- Isbir G G, Serçekuş P, Yenal K, et al. The prevalence and associated factors of fear of childbirth among Turkish pregnant women. J Reprod Infant Psychol. 2024;42(1):62–77.
- Molgora S, Fenaroli V, Prino LE, et al. Fear of childbirth in primiparous Italian pregnant women: the role of anxiety, depression, and couple adjustment. Women Birth. 2018;31(2):117–123.
- Dai L, Rong Z. Prediction and prevention of recurrent hypertensive diseases during pregnancy in elderly pregnant women. Chin J Appli Gynecol Obstetri. 2019;39(06):588–593.
- Zhao H, Zhai JL, Zhang Z, et al. Analysis of influencing factors of mental health and health care demand of elderly pregnant women with second child. Chin J Fam Plann. 2019;31(05):1036–1041.
- Stephanie A, Ana F, C CM, et al. Dyadic coping and dyadic adjustment in couples with women with high depressive symptoms during pregnancy. J Reprod Infant Psychol. 2018;36(5):504–518.
- Zhao L, Jl L, Wang J, et al. Analysis of duality coping status and influencing factors in young and middle-aged patients with type 2 diabetes. Chin J Nurs. 2022;57(05):576–581.
- Song LQ, Li JL, Tao ML. Investigation on pregnancy stress and its influencing factors. Chin J Nurs. 2013;48(09):808–811.
- Falconier MK, Wojda-Burlij AK, Conway CA, et al. The role of emotion regulation in couples’ stress communication and dyadic coping responses. Stress Health. 2023;39(2):309–322.
- Johnson MD, Horne RM, Galovan AM. The developmental course of supportive dyadic coping in couples. Dev Psychol. 2016;52(12):2031–2043.
- Pandey Bista A, Shrama C, Shrestha U, et al. Effect of Group Psycho-Educational Interventions on Child birth fear and Child birth Self-efficacy among Primiparous women. J Nepal Health Res Counc. 2023;20(4):846–851.
- Dai L, Shen Q, Redding SR, et al. Simulation-based childbirth education for Chinese primiparas: a pilot randomized controlled trial. Patient Educ Couns. 2021;104(9):2266–2274.
- Won SK, Seol KO. Actor and Partner Effects of Couple’s Daily Stress and Dyadic Coping on Marital Satisfaction. J Korean Acad Nurs. 2020;50(6):813–821.
- Qin X, Zhang W, Xu S, et al. Characteristics and related factors of family functioning in Chinese families during early pregnancy. Front Psychol. 2023;14:1102796.
- Ji WJ, Rao L, Zhou X, et al. Longitudinal study on mental health status and sleep quality during pregnancy. Chin J Gener Pract. 2019;21(09):1552–1555+1589.
- Redinger S, Pearson RM, Houle B, et al. Antenatal depression and anxiety across pregnancy in urban South Africa. J Affect Disord. 2020;277:296–305.
- Jonsdottir SS, Steingrimsdottir T, Thome M, et al. Pain management and medical interventions during childbirth among perinatal distressed women and women dissatisfied in their partner relationship: a prospective cohort study. Midwifery. 2019;69:1–9.
- Chaves C, Canavarro MC, Moura-Ramos M. The Role of Dyadic Coping on the Marital and Emotional Adjustment of Couples With Infertility. Fam Process. 2019;58(2):509–523.
- Donarelli Z, Salerno L, Lo Coco G, et al. From telescope to binoculars. Dyadic outcome resulting from psychological counselling for infertile couples undergoing ART. J Reprod Infant Psychol. 2019;37(1):13–25.
- Zhu CY, Jin FJ, Hu MM, et al. Research status of pregnancy stress in China. Chin J Gener Prac. 2020;18(08):1353–1357.
- Pazzagli C, Laghezza L, Capurso M, et al. Antecedents and consequences of fear of childbirth in nulliparous and parous women. Infant Ment Health J. 2015;36(1):62–74.