
Abstract
Purpose
To report a case of filamentary keratitis occurring in the cornea hidden under the eyelids by squint surgery.
Methods
A 69-year-old female patient with a history of amblyopia was referred for intractable filamentary keratitis in the left eye. The strabismus angle was 35Δ hypertrophic, and ocular motility was within the normal range. Slit-lamp examination of her left eye revealed filamentary keratitis in more than one-third of the upper cornea behind the upper eyelid. Her right eye was diagnosed as supranuclear double elevator palsy. We performed strabismus surgery on her right eye, including inferior rectus muscle recession (5 mm) in combination with superior rectus muscle resection (5 mm) under local anesthesia. Following surgery, the left eye squint angle was improved. The filamentary keratitis of the left eye disappeared, and there was no recurrence over the following 5 years.
Conclusion
The squint surgery of paralyzed right eye decreased the strabismus angle, subsequently resulting in the disappearance of the filamentary keratitis in the left eye via the resolution of the relative blepharoptosis. Although the squint operation performed was not for the purpose of improving binocular function, we want to conclude that it can treat the filamentary keratitis behind the eyelid.
It has been reported that eyelid surgery can effectively treat filamentary keratitis that occurs on the area of the cornea located behind the eyelid.Citation1 In general, squint-related surgeries can be used to improve binocular function. However, here we report a case of intractable filamentary keratitis that occurred on the upper cornea at the area behind the upper eyelid, which was successfully treated by a squint operation performed on the contralateral eye.
Case report
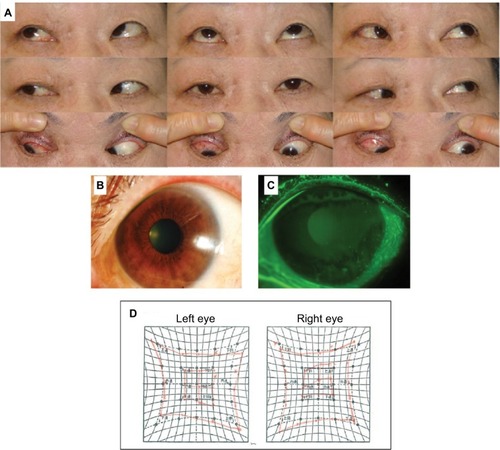
A 69-year-old female patient with a history of amblyopia in her left eye was referred to our department in January 2012 for intractable filamentary keratitis in the left eye. Upon examination, we found that the uncorrected visual acuity in her right eye was 0.6 in decimal and the best-corrected visual acuity was 0.8, −0.5 diopter (D) for myopia and −0.5 D for astigmatism with 135° axis. Both uncorrected and corrected visual acuities in her left eye were 0.08, which was uncorrectable. In her left eye, the strabismus angle was 35Δ hypertrophic and ocular motility was within the normal range. Her right eye was the dominant eye, with imperfect upper rotation at the inside and outside transposition () and positive Bell’s phenomenon. Hence it was diagnosed as supranuclear double elevator palsy (DEP). Slit-lamp examination of her left eye revealed filamentary keratitis in more than one-third of the upper cornea behind the upper eyelid (). An upward restriction of right eye was shown using Hess chart (). The patient explained that she had experienced a long history of severe pain in that eye, and that it had been resistant to a variety of topical treatments. On March 2012, we performed strabismus surgery on her right dominant eye, including inferior rectus muscle recession (5 mm) in combination with superior rectus muscle resection (5 mm) under local anesthesia. Following surgery, the left eye squint angle was improved to 5Δ hypertrophic (). As a combination therapy, a bandage soft contact lens was applied for 2 weeks on her left eye and eye drops containing 0.5% levofloxacin and 0.1% fluorometholone were instilled twice daily in that eye for 3 months post operation, and then discontinued. The filamentary keratitis of the left eye disappeared, and there was no recurrence over the following 5 years (). After the surgery, uplift limit of right eye was improved ().
Figure 1 Preoperative findings.
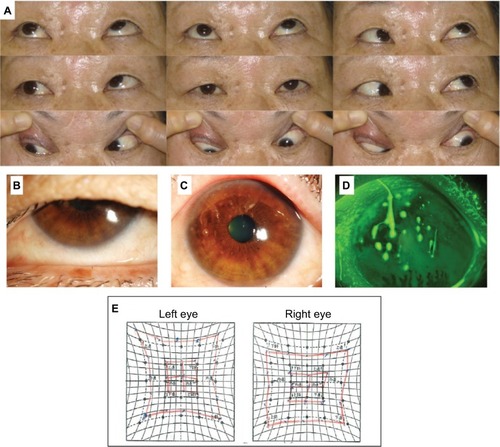
Figure 2 Postoperative findings.
Written informed consent was obtained from the patient to publish this case report and the accompanying images.
Discussion
Filamentary keratitis is a chronic corneal disease characterized by the adherence of filamentous material to the corneal surface.Citation2 It has been suggested that the mechanism of this disease is associated with tear abnormalities such as increased mucin in the tear film due to aqueous tear deficiency or facilitated evaporation of tears, or lid abnormalities such as blepharoptosis or sustained eyelid closure. Corneal filaments are reportedly composed of strings of corneal epithelial cells that form the core of the filamentous structure and that are surrounded by mucin, inflammatory cells, and conjunctival epithelial cellsCitation3 that are formed in association with the increased friction between the cornea and eyelid during blinking.Citation4 To date, there is no effective treatment for the filament itself. However, it has been reported that eyelid surgery is effective for treating cases of filamentary keratitis associated with blepharoptosis.Citation1 It has been reported that filamentary keratitis can occur at the area of the cornea hidden behind the eyelids due to strabismus,Citation5 yet there are no reports of filamentary keratitis associated with strabismus being successfully treated by strabismus surgery alone. DEP is hypotropia with imperfect upper rotation at the inside and outside transposition. In cases of paralysis eye fixation, the strabismus angle is known to generally become more severe by the Hering’s law of equal innervation.Citation6 By paralyzed eye surgery, it was expected that the effect will be stronger. Thus, we presumed that the larger angle hyperopia in our patient’s left eye resulted in the relative blepharoptosis which led to the filamentary keratitis via increased friction. We carried out a paralytic right eye surgery on the supra-nuclear ophthalmoplegic eye, with the intention of reducing the strabismus angle. If the operation of non-paralyzed left eye was carried out, the effect could be insufficient. The squint surgery of paralyzed right eye decreased the strabismus angle, subsequently resulting in the disappearance of the left eye filamentary keratitis via the resolution of the relative blepharoptosis.
Acknowledgments
The authors wish to thank John Bush for reviewing the case report.
Disclosure
The authors report no conflicts of interest in this work.
References
- KitazawaKYokoiNWatanabeAEyelid surgery for refractory filamentary keratitisNihon Ganka Gakkai Zasshi20111158693698 Japanese21882586
- HamiltonWWoodTOFilamentary keratitisAm J Ophthalmol19829344664697072810
- ZaidmanGWGeeraetsRPaylorRRFerryAPThe histopathology of filamentary keratitisArch Ophthalmol19851038117811814026649
- TaniokaHYokoiNKomuroAInvestigation of the corneal filament in filamentary keratitisInvest Ophthalmol Vis Sci20095083696370219443713
- GoodWVWhitcherJPFilamentary keratitis caused by corneal occlusion in large-angle strabismusOphthalmic Surg1992231661574277
- ZIFFERAMonocular elevation deficiency (Double elevator palsy) and Monocular depressor deficiency (Double depressor palsy)RosenbaumALSantiagoAPClinical Strabismus Management, Principle and Surgical TechniquePhiladelphiaW.B. Saunders Company1999