
Abstract
Objective
To report a patient with severe Chrysosporium keratitis successfully treated by voriconazole.
Method
Case report.
Results
A 37-year-old healthy male presented with irritation, pain and reduced vision in his left eye after mud contamination. Examination demonstrated corneal stromal infiltration, endothelial plaque and hypopyon. Corneal scrapings demonstrated numerous septate hyphae, and specimen cultures were positive for Chrysosporium sp. The lesion did not respond to aggressive topical 5% natamycin, 0.15% topical amphotericin B and oral itraconazole. The patient was then treated by topical 1% voriconazole every hour. Intracameral and intrastromal voriconazole injections (50 μg/0.1 mL) were also undertaken. The keratitis was significantly improved after voriconazole.
Conclusion
To the best of the authors’ knowledge, this is the first report on the use of voriconazole for Chrysosporium keratitis. Voriconazole may be an effective alternative to conventional antifungal agents in some cases of fungal keratitis. It should be considered before shifting to therapeutic keratoplasty.
Introduction
Chrysosporium is an unusual filamentous fungus commonly isolated from soil and occasionally encountered in the laboratory as contaminants of cutaneous and respiratory specimens.Citation1 Although human infection is very rare, it can lead to either serious systemic or ocular diseases.Citation2–Citation4 In the literature review, there were only two case reports on ocular infection. Both cases did not respond to aggressive medical treatment and ended up with surgical interventions.Citation3,Citation4 The authors herein report a first case with severe Chrysosporium keratitis successfully treated with voriconazole. The patient has signed written informed consent for the case details and accompanying images to be published.
Case report
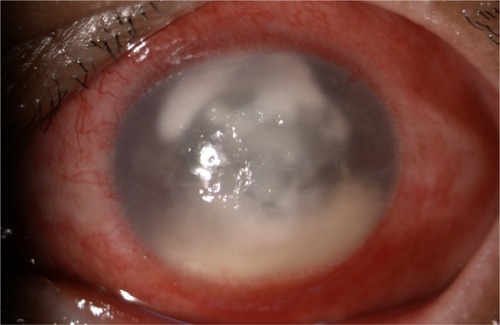
A 37-year-old male presented with irritation, pain and reduced vision in the left eye after mud contamination. On examination, his best-corrected visual acuity in the left eye was hand movements and the right eye was 6/6. The left eye revealed a central, irregular, 6.8×7.4 mm infiltration with a feathery edge and satellite lesions. The hypopyon level was about 2–3 mm (). Corneal scraping revealed numerous septate hyphae. The patient was first treated with topical 5% natamycin, 0.15% amphotericin B eye drops hourly and oral itraconazole 200 mg daily. Intracameral and intrastromal amphotericin B (5 μg/0.1 mL) injections were also undertaken. However, there was no significant clinical improvement. Three days after presentation, infiltration began to deteriorate.
Figure 1 Biomicroscopic photograph of left eye demonstrating central corneal infiltration with hypopyon.
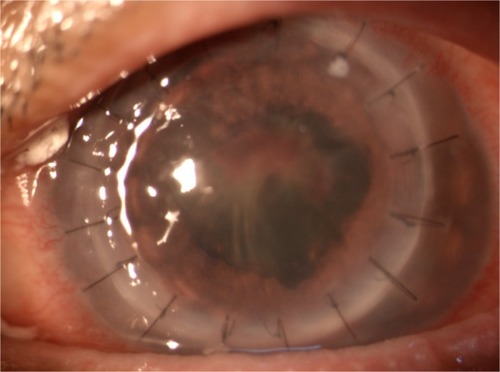
The patient was then treated with topical 1% voriconazole every 1 h, and topical natamycin was discontinued. Additionally, intracameral and intrastromal injections of voriconazole (50 mg/0.1 mL) were given. Two days after treatment, slit-lamp examination showed marked improvement with a decreased corneal infiltrate and hypopyon. Chrysosporium sp. was identified by corneal cultures 3 days later. After 7 days of voriconazole treatment, the corneal infiltration was decreased to 5.4×6.2 mm surrounded by corneal scarring, and no hypopyon was detected. The topical and systemic medications were continued and tapered according to clinical findings. Finally, the lesion healed to be corneal scar and visual acuity was 4/60. One month later, the patient underwent penetrating keratoplasty for corneal scar (). Immediate postoperative visual acuity in his left eye was 6/36 and final best-corrected visual acuity was 6/18 at 3 months after the procedure.
Figure 2 Biomicroscopic photograph of left eye after penetrating keratoplasty for corneal scar.
Discussion
Chrysosporium is classified in Kingdom Fungi, Phylum Ascomycota, Class Eurotiomycetes, Order Onygenales and Family Onygenaceae. It is a keratinophilic filamentous fungus commonly isolated from soil and occasionally encountered in the laboratory as contaminants of cutaneous and respiratory specimens.Citation1 Although human infection is very rare, it can lead to either serious systemic or ocular diseases.Citation2–Citation4 Among ocular infections, there were only two reports, which were keratomycosis and endophthalmitis from literature search. Medical failure has been reported, and surgical debridements, penetrating keratoplasty and pars plana vitrectomy were required in both cases.Citation3,Citation4
For the keratomycosis case, corneal infiltration was deteriorating and perforation was detected after natamycin eyedrops treatment. Emergency penetrating keratoplasty was undertaken.Citation3 In this study, the fungus did not respond to topical natamycin, which corresponded to previous report. In the endophthalmitis case, diluted intravitreal amphotericin B (1 mg/0.1 mL) was injected after pars plana vitrectomy with topical antibiotics, intravenous antibiotics and oral itraconazole.Citation4 To the best of the authors’ knowledge, this is the first report on the successful treatment of Chrysosporium keratitis with voriconazole.
Information about in vitro studies of antifungal agents for Chrysosporium sp. is limited. In one study that is included, the strains of Chrysosporium zonatum infection of lung and bone showed that the organism is susceptible to amphotericin B but moderately resistant to itraconazole and fluconazole, whereas 5-fluorocytosine was not effective.Citation1 These data have suggested that current azoles may not be clinically active against the organism. The patient in this study, however, did not respond to either amphotericin B or itraconazole treatment.
Voriconazole is increasingly used as a first-line treatment for ocular fungal infections because of excellent in vitro activity against a wide range of keratitis isolates.Citation5 Eventhough the evidence shows that natamycin is more effective than voriconazole in the treatment of fungal ulcers,Citation6,Citation7 voriconazole has been reported to be an alternative option in some cases such as drug-resistant fungal keratitis or rare fungal species causing keratitis.Citation8,Citation9
In the present case, the ulcer was successfully treated with voriconazole eyedrops including adjunctive intracameral and intrastromal injections. This may be explained by the lower minimum inhibitory concentrations of voriconazole against numerous mould isolates causing fungal keratitis.Citation9 In addition, voriconazole concentrations in the aqueous humor after topical 1% voriconazole eyedrops are above the minimum inhibitory concentrations, which is sufficient to eradicate most fungal species.Citation5 Furthermore, from our observations, the injections can expedite the healing process.
Conclusion
In conclusion, voriconazole may be an alternate option for some fungal species causing keratomycosis. Due to the high rate of complications after penetrating keratoplasty in active fungal keratitis, voriconazole may be considered before radical surgery is scheduled. Moreover, natamycin may not be more effective than voriconazole in all fungal keratitis cases. Standardized susceptibility testing methods using ocular strains may be required for future decisions and management. Clinical correlation, however, is still the most important clue for the treatment.
Acknowledgments
The authors would like to thank Prof James A Will (University of Wisconsin, USA) for editing the manuscript via Publication Clinic KKU, Thailand, and Dr Wathanee Sripawadkul (Department of Ophthalmology, Faculty of Medicine, Khon Kaen University) for her assistance in manuscript preparation.
This study was approved by the Khon Kaen University Ethics Committee for Human Research at the Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand.
Disclosure
The authors report no conflicts of interest in this work.
References
- RoilidesESiglerLBibashiEKatsifaHFlarisNPanteliadisCDisseminated infection due to Chrysosporium zonatum in a patient with chronic granulomatous disease and review of non-Aspergillus fungal infections in patients with this diseaseJ Clin Microbiol199937118259854057
- AnsteadGMSuttonDAGraybillJRAdiaspiromycosis causing respiratory failure and a review of human infections due to Emmonsia and Chrysosporium sppJ Clin Microbiol20125041346135422259200
- WagonerMDBadrIAHidayatAAChrysosporium parvum keratomycosisCornea199918561662010487440
- ShekharHGogiaVVashishtNEndogenous endophthalmitis by Chrysosporium: an opportunistic pathogenOcul Immunol Inflamm201422215816024564480
- NeohCFLeungLChanEThe Absorption and Clearance of Voriconazole 1% eye drops–an open label studyAntimicrob Agents Chemother2016 pii: AAC.00683-16
- FlorCruzVEvansJRMedical interventions for fungal keratitisCochrane Database Syst Rev20154CD004241
- PrajnaNVKrishnanTMascarenhasJThe mycotic ulcer treatment trial: a randomized trial comparing natamycin vs voriconazoleJAMA Ophthalmol2013131442242923710492
- ChengSCLinYYKuoCNLaiLJCladosporium keratitis–a case report and literature reviewBMC Ophthalmol20151510626286482
- ShobanaCSMythiliAHomaMIn vitro susceptibility of filamentous fungi from mycotic keratitis to azole drugsJ Mycol Méd2015251444925541256