
Abstract
Purpose
To present a successful case of single-staged total upper eyelid reconstruction after sebaceous gland carcinoma excision by using forehead galeal pericranial flap.
Observations
An 80-year-old female with a progressively enlarged left upper eyelid mass presented with ocular irritation, blurred vision, and gritty sensation despite topical antibiotics treatment. This multinodular mass involved the left total upper eyelid, compromised corneal surface integrity, and caused complete ptosis. Excisional biopsy confirmed advanced sebaceous gland carcinoma, which was followed by extensive excision. The resultant total upper eyelid defect was reconstructed by a forehead galeal pericranial flap accompanied by anterior and posterior lamellar grafts. For the 34-month follow-up period, patient remained symptom-free without tumor recurrence and achieved acceptable cosmetic outcome.
Conclusion
The forehead galeal pericranial flap appears to be effective as single-staged total upper lid reconstruction following extensive sebaceous gland carcinoma excision to restore eyelid function, avoid corneal exposure, and achieve acceptable cosmesis.
Introduction
Total eyelid defect caused by the loss of the full thickness of the eyelids from medial to lateral canthus commonly results from periocular tumor excision. Although rare but easily overlooked, sebaceous gland carcinoma is a highly malignant eyelid tumor that often results in extensive tumor excision.Citation1
It remains challenging to reconstruct the aforementioned total upper eyelid defect. Two-staged surgical treatment techniques, including Cutler–Beard,Citation2 Mustardè,Citation3 modified Hughes,Citation4 tarsoconjunctival rotational,Citation5 or advancement,Citation6 have been described. To reduce surgical sessions and decrease eyelid donor tissue morbidity, single-staged surgery utilizing frontalis muscle flapCitation7,Citation8 and forehead galeal pericranial flap have demonstrated promising results. Forehead galeal pericranial flap has been employed during medial canthus reconstruction,Citation9 subtotal and total upper lid reconstruction for tumor excision, and periorbital faciitis,Citation10 respectively. The galeal aponeurotica consists of dense connective tissue that originates on the occipital bone and inserts onto the frontalis muscle. These nonbulky flaps are viable to ensure good functional and morphological outcomes, avoid a second surgical session, preserve local tissues and innervations, and achieve satisfactory cosmesis. Herein, we reported a single case demonstrating how this procedure can be used as an effective reconstruction option for advanced sebaceous carcinoma following total upper lid excision.
Case report
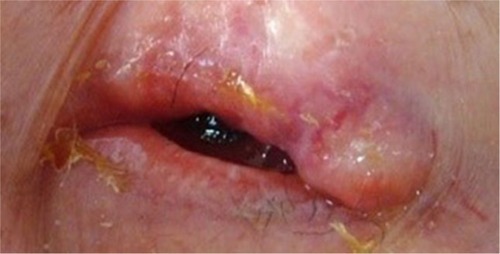
An 80-year-old female complained of a 1-year history of ocular irritation, blurred vision, and gritty sensation despite topical tetracycline 1% three times daily and erythromycin 0.5% twice a day for refractory blepharoconjunctivitis and recurrent chalazion in the left eye. On examination, her best-corrected visual acuity was 20/20 in the right eye and hand motion in the left eye. External examination revealed mild telangiectasia on the left upper eyelid with a mass consisting of multiple, firm, thickened, irregular nodules (). This mass was fixed to the underlying tissue and resulted in complete ptosis without any eyelid blinking. Consequently, the left eye exhibited a scanty tear meniscus, central corneal haze and neovascularization, and diffuse conjunctival injection.
Figure 1 An extensive left upper eyelid mass.
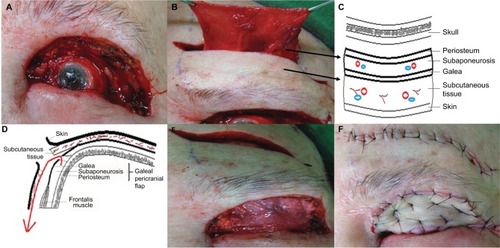
We obtained written informed consent from the patient to perform the following surgical procedures as well as consent to the publication of her case details and any accompanying images. We first performed incisional wedge of the left upper eyelid. Microscopic examination disclosed a poorly differentiated sebaceous carcinoma with infiltrative growth and pagetoid invasion of overlying eyelid epithelium and deep superficial orbicularis muscle. Then under general anesthesia, we performed total removal of the tumor in the left upper lid including superior conjunctival fornix and nearly total removal of levator muscle resulting in the full-thickness eyelid defect measuring 4.5×1.5 cm, extending from the medial and lateral canthi to the inferior eyebrow (). This defect was reconstructed by a hard palate graft secured to the remnants of the conjunctiva with 6–0 Vicryl (Polyglactin 910, Ethicon®, Somerville, NJ, USA) at the resection borders as posterior lamella. Then we obtained the galeal pericranial flap measuring 4×4.5 cm by an incision along the frontal skin crease above the eyebrow through the skin, and subcutaneous tissues, dissection above the frontalis muscle, and vertical relaxing incisions medially and laterally (, illustrated as 2C [coronal plane] or 2D [sagittal plane]). Blunt dissection along the soft tissues of the eyebrow and supraorbital margin was performed to create a tunnel to flip and slide the galeal pericranial flap to reach the previous upper lid margin. Because the levator muscle was nearly completely removed as a result of extensive tumor involvement, we were able to identify the remaining stump of the elevator aponeurosis and reanchor it to the flap to preserve some levator function. The upper margin of the galeal pericranial flap was sutured with 6–0 Vicryl to the remnant of the resected medial and lateral left upper eyelid borders (). Finally, a full-thickness skin graft was harvested from the patient’s inguinal area to cover the external surface of the galeal pericranial flap to reconstruct the anterior lamella ().
Figure 2 Surgical technique for single-staged total upper eyelid reconstruction after sebaceous gland carcinoma excision.
One month after surgery, ocular symptoms completely resolved and the flaps and grafts were viable with no evidence of necrosis. Partial forehead sensation remained intact and there was preservation of muscle tone. Patient had acceptable eyelid closure () and regained 3–4 mm eyelid opening (). Two months later, she developed tumor metastasis to the ipsilateral parotid gland lymph nodes and subsequently received adjuvant chemotherapy and local radiation therapy. Another month later, her left eye showed regressed corneal neovascularization, uninflamed conjunctiva, moderate tear meniscus, and improved visual acuity from hand motion to 20/400. No postoperative complications such as lid retraction, corneal erosion, or ulceration were observed. For a total follow-up period of 34 months, she remained symptom free without eyelid tumor recurrence and achieved acceptable cosmetic outcome.
Figure 3 Surgical outcome.

Discussion
Despite the numerous traditional two-staged reconstructive surgical methods reported over the years,Citation2–Citation6 total upper eyelid restoration remains complex and challenging owing to the limited neighboring tissue as well as the difficulty in preserving the highly specialized function of the upper eyelid. Although a two-staged procedure may be valuable, single-staged reconstructive surgery has gained considerable interest for simplifying procedures by avoiding lower lid disruption, minimizing donor tissue morbidity, and has proven worthy of joining the treatment options to ensure an optimal outcome. In accordance with recent single-staged surgical developments,Citation11–Citation13 herein we present a case of extensive sebaceous gland carcinoma excision followed by successful single-staged total upper eyelid reconstruction with forehead galeal pericranial flap. After the surgery, patient experienced complete symptom resolution, as well as improved corneal integrity and visual acuity. Consistent with previous report,Citation10 this case highlights single-staged reconstructive surgery with galeal pericranial flap as an effective treatment to restore eyelid function, avoid corneal exposure, and achieve satisfactory cosmesis.
Harvesting the galeal pericranium without complete disruption of the frontalis muscle helps preserve forehead sensation and motility during facial expression. In addition, harvesting hard palate and inguinal skin has minimal donor-site morbidity. While the thickness and potential scarring of a frontalis muscle flap may be less satisfactory for upper lid reconstruction in one studyCitation14 but not others,Citation7,Citation8 the fibrous sheet of galeal pericranial flap in this case is ideal owing to the thin but remarkably tough connective tissue to support anterior and posterior lamella grafts. In addition, the galeal pericranial flap serves as a good vascular supply to both the underlying tarsal graft and the overlying free skin graft.Citation15 Furthermore, the forehead horizontal wrinkle lines in the patient conceal the transverse incisions as the scar is hidden in the crease. Although the remaining levator muscle was nearly completely removed resulting in limited eyelid excursion, this technique avoids postoperative lid retraction or exposure keratopathy and allows reconstruction of not only large horizontal but also vertical defects. Collectively, the single-staged forehead galeal pericranial flap appears to be a reliable surgical option for total upper lid reconstruction.
Acknowledgments
The authors gratefully thank Dr. Scheffer C.G. Tseng for his guidance and great support.
Disclosure
The authors report no conflicts of interest in this work.
References
- MuqitMMFootBWaltersSJMudharHSRobertsFRennieIGObservational prospective cohort study of patients with newly-diagnosed ocular sebaceous carcinomaBr J Ophthalmol2013971475123117971
- CutlerNLBeardCA method for partial and total upper lid reconstructionAm J Ophthalmol19553911713218104
- MustardeJCMajor reconstruction of the eyelids: functional and aesthetic considerationsClin Plast Surg1981822272367273625
- MaurielloJAJrAntonacciRSingle tarsoconjunctival flap (lower eyelid) for upper eyelid reconstruction (“reverse” modified Hughes procedure)Ophthalmic Surg19942563743788090416
- KerstenRCAndersonRLTseDTWeinsteinGLTarsal rotational flap for upper eyelid reconstructionArch Ophthalmol198610469189223718318
- LeoneCRJrTarsal-conjunctival advancement flaps for upper eyelid reconstructionArch Ophthalmol198310169459486860211
- StewartCMTanLTJohnsonDNorrisJHKey Issues When reconstructing extensive upper eyelid defects with description of a dynamic, frontalis turnover flapOphthal Plast Reconstr Surg2016324249251
- JeanRDWongWWMartinMCSingle-stage frontalis muscle flap for full-thickness reconstruction of the upper eyelidJ Craniofac Surg20112251762176421959427
- LeatherbarrowBWatsonAWilcsekGUse of the pericranial flap in medial canthal reconstruction: another application for this versatile flapOphthal Plast Reconstr Surg2006226414419
- BrusatiRCollettiGRedaelliVUpper eyelid reconstruction with forehead galeal flapJ Plast Reconstr Aesthet Surg200962790190518472325
- ScuderiNRibuffoDChiummarielloSTotal and subtotal upper eyelid reconstruction with the nasal chondromucosal flap: a 10-year experiencePlast Reconstr Surg200511551259126515809583
- ToftPBReconstruction of large upper eyelid defects with a free tarsal plate graft and a myocutaneous pedicle flap plus a free skin graftOrbit20163511526636623
- PushkerNBatraJMeelRBajajMSChawlaBGhoseSLateral eyelid rotation flap: a novel technique for reconstruction of full thickness eyelid defectInt ophthalmol201535679379925673519
- KazanjianVHRoopenianAMedian forehead flaps in the repair of defects of the nose and surrounding areasTrans Am Acad Ophthalmol Otolaryngol195660455756613360821
- TseDTGoodwinWJJohnsonTGilbergSMeldrumMUse of galeal or pericranial flaps for reconstruction or orbital and eyelid defectsArch Ophthalmol199711579329379230844