
Abstract
The purpose of this study was to describe a case of necrobiotic xanthogranuloma scleritis in a 53-year-old male with unilateral progressive visual loss, scleritis, prolonged fever, and multiple mononeuropathy. Scleral biopsy showed necrosis with small abscess, and the pathological tissues revealed submucosal infiltration of mononucleated foamy histiocytes (xanthoma cells), hemosiderin-laden macrophages, neutrophils, lymphocytes, plasma cells, and erythrocytes without Touton giant cells or cholesterol clefts. Serum protein electrophoresis showed polyclonal gammopathy. All infectious investigations were negative. Afterward, this patient was diagnosed with granulomatosis with polyangiitis based on granuloma found in scleral tissue, vasculitis seen in sural nerve biopsy and positive serologies (C-ANCA and anti-PR3 antibody). He was treated with high-dose corticosteroid and later with intravenous cyclophosphamide monthly. He responded well to treatment, both eye and systemic conditions. Necrobiotic xanthogranuloma scleritis could be an early presentation of granulomatosis with polyangiitis.
Case report
In 2016, a 53-year-old man for the first time was admitted in Phramongkutklao Hospital. He had suffered from progressive visual loss and redness for 2 months in the left eye without any photophobia, ocular pain, or discharge. His right eye was not affected. The visual acuity was 20/20 in the right eye and hand movement in the left eye. The examination of the left eye showed generalized ciliary injection with whitish scleral nodule at inferotemporal area. Anterior segment examination revealed anterior chamber cell 3+, seclusio pupillae. Fundus examination showed vitreous haze with unclear retinal details. Intraocular pressure was 18 in both the eyes. The right eye was normal when examined.
Ocular ultrasonography showed hypohyperechogenicity, membrane-like lesion in intravitreous cavity without retinal detachment, fluid collection, or any mass. Nodular scleritis and chronic panuveitis in the left eye was the initial diagnosis.
Scleral exploration, phacoemulsification with intraocular lens implantation, and diagnostic vitrectomy left eye were performed. In intraoperative, we found scleral necrosis with small abscess () at inferotemporal area. The fundus showed dense yellowish turbid vitritis (), retinal and perivascular infiltration, retinal edema, and shallow subretinal fluid at inferior retina. A vitreous sample was sent to the laboratory to perform polymerase chain reaction (PCR) for tuberculosis, herpesvirus family, gram stain, potassium hydroxide (KOH), culture for bacteria and fungus, and cytology for malignancy.
Figure 1 (A) and (B) show generalized diffuse scleritis with scleral abscess inferotemporal area.
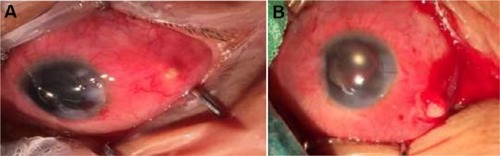
Figure 2 Turbid yellowish vitreous fluid from diagnostic vitrectomy.

The left eye was treated as infectious scleritis and endophthalmitis by using intravenous cefazolin and amikacin for 2 weeks followed by oral augmentin, topical cefazolin, and amikacin which were later changed to vancomycin and ceftazidime, 3 times of sclera debridement, and intravitreous vancomycin and ceftazidime injection. After the treatment for 2 weeks, the findings on his left eye showed no improvement.
The investigations included scleral and vitreous gram stain, KOH, culture for bacteria, fungus, mycobacteria, PCR for herpes 7 types, and tuberculosis which were all negative. The pathology of scleral biopsy presented necrobiotic xanthogranulomatous inflammation of sclera with severe acute and chronic inflammation and mycobacteria and fungus were also negative. He was diagnosed with necrobiotic xanthogranulomatous scleritis with panuveitis in the left eye. Then, topical 1% prednisolone acetate eye drop 4 times a day and oral prednisolone 1 mg/kg/day were prescribed. The clinical injection and sclera necrosis, was much improved that included the decrease of anterior chamber cells from 3+ to 1+ after the administration of steroids; however, the visual acuity was still hand motion. After that, steroids were slowly tapered.
After 5 months, the patient was admitted to internal medicine service for prolonged fever. He had low-grade fever without chills for 6 weeks. No source of infection was identified after thorough evaluation including blood culture, urine culture, bone marrow aspiration, echocardiogram, and chest film. He was treated with ceftriaxone and doxycycline for 7 days with no improvement and was later switched to meropenem for 7 days without resolution of fever. During this admission, he developed bilateral foot drop and numbness in both hands.
This time of admission, besides fever, foot drop and numbness, he complained of transient visual loss duration of 1 minute 5–6 times a day in his right eye. Physical examination found high blood pressure 150/100 mmHg and body temperature of 39°C. The visual acuity was 20/70 in the right eye and light projection in the left eye. The right eye presented dot and blot hemorrhage at posterior pole of fundus. The left eye was not injected and showed quiet anterior chamber with occlusio pupillae. He had no rash or cervical lymphadenopathy. Heart, lung, and abdominal examinations were normal. Neurological examination confirmed weakness of ankle flexion, bilaterally and numbness in both hands. It consisted with pathology in common peroneal nerve and median nerve, respectively which were consistent with multiple mononeuropathy.
Initial work-up found hemoglobin of 8.3 mg/dL, white blood cell count of 11,400 cell/mL, platelet of 107,000/mL, erythrocyte sedimentation rate (ESR) 31 mm/h, creatinine 1.0 mg/dL, blood urea nitrogen 1.3 mg/dL, aspartate aminotransferase 17 IU/L, alanine aminotransferase 20 IU/L, total bilirubin 0.5 mg/dL, direct bilirubin 0.2 mg/dL, TG 78 mg/dL, cholesterol 194 mg/dL, high-density lipoprotein 86 mg/dl, and low-density lipoproteins 114 mg/dL. Peripheral blood smear revealed normochromic microcytic red blood cells, normal morphology of WBC, and platelet. Both direct and indirect Coombs tests were negative. Urine analyses found no proteinuria, red blood cell 3–5 cell/HPF, white blood cell 0–1 cell/HPF, and no red blood cast. Serum protein electrophoresis showed polyclonal gammopathy with albumin 36.5%, alpha1 8.2%, alpha2 14.9%, beta1 6.1%, beta2 5.2%, gamma 29.1%.
Infectious work-up were negative including HIV, hepatitis B virus, hepatitis C virus, Quantiferon TB gold test, treponema pallidum hemagglutination, and venereal disease research laboratory test.
Immunologic studies found positive antinuclear antibody 1:80 speckle pattern. Anti-ds-DNA and antiextractable nuclear antibody was negative. Anti-neutrophilic cytoplasmic antibody (ANCA) found cytoplasmic pattern and later confirmed that anti-proteinase 3 (PR3) positive 3+, IgG4 was 4.60 g/L. Chest X-ray was normal. Nerve conduction study and electromyography found asymmetrical axonal sensory motor polyneuropathy. Left sural nerve biopsy confirmed mild medium-sized vasculitis.
This patient was diagnosed with granulomatosis with polyangiitis based on granuloma found in scleral tissue, vasculitis seen in sural nerve biopsy and serologies (C-ANCA and anti-PR3 antibody).
This patient was treated with high-dose dexamethasone and later switched to prednisolone (1 mg/kg/day) and intravenous cyclophosphamide monthly as well as antihypertensive drugs. He responded well to treatment, ankles flexion improved and numbness of both hands was reduced. Regarding the transient visual loss, the computed tomography angiography was done and no filling defect was reported. The amaurosis fugax was diagnosed and suspected from vasculitis. He did not develop recurrent transient visual loss. At the final visit, the visual acuity was 20/20 in the right eye and no light perception in the left eye. Both eyes were not injected and quite anterior chamber. The left eye presented early phthisis bulbi.
This case report was approved by the Institutional Review Board, Royal Thai Army Medical Department. Written informed consent was obtained from the patient to have the case details and for any accompanying images published.
Pathology
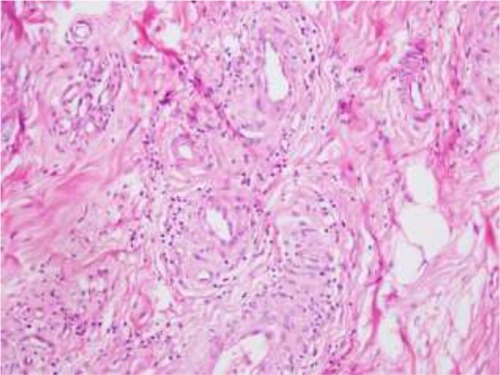
Multiple scleral biopsies were performed, and the findings revealed erosive scleral mucosa with submucosal infiltration by sheets of mononucleated foamy histiocytes (xanthoma cells), accompanied by variable degree of fibrosis with necrobiosis of collagen ( and ). Variable numbers of dispersed hemosiderin-laden macrophages, neutrophils, lymphocytes, plasma cells, and erythrocytes without Touton giant cells, or cholesterol clefts were scattered among these xanthoma cells. These infiltrating xanthoma cells often have small, round nuclei, and abundant clear or vacuolated cytoplasm (). Some of these histiocytes show hemophagocytic activity (). Despite the absence of Touton giant cells and cholesterol clefts, the findings previously confirmed were favorable of necrobiotic xanthogranulomatous inflammation of the sclera.Citation1 Left sural nerve biopsy confirmed small- and medium-sized vasculitis by lymphocytic and neutrophilic infiltrate in wall of subcutaneous vessels ().
Figure 3 A scleral tissue biopsy showing mucosal erosion and submucosal fibrosis with necrobiosis of collagen and sheets of mononucleated foamy histiocytes (xanthoma cells), infiltrating the submucosal fibrous tissue, accompanied by variable numbers of dispersed lymphocytes and plasma cells (hematoxylin-eosin; original magnification: ×40).
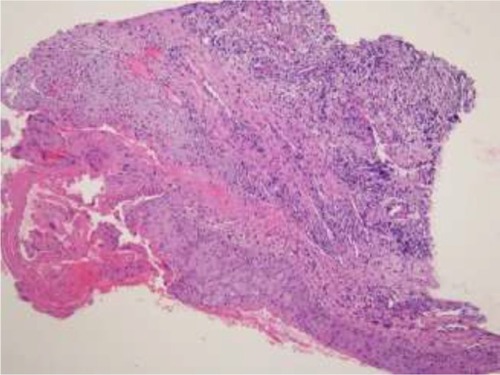
Figure 4 Another scleral tissue biopsy predominantly containing fibrosis with necrobiosis of collagen and scattered necrotic cellular debris of inflammatory cells (hematoxylin-eosin; original magnification: ×200).
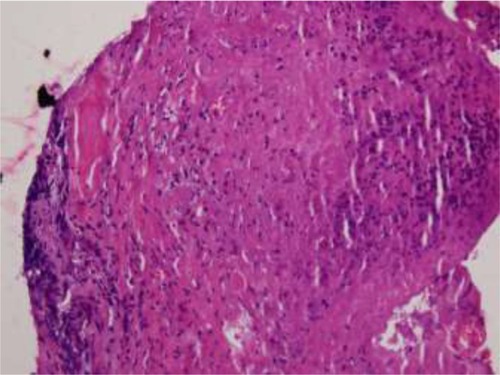
Figure 5 Sheets of xanthoma cells and scattered hemosiderin- laden macrophages, neutrophils, lymphocytes, plasma cells, and erythrocytes. The xanthoma cells have small, round nuclei and abundant clear or vacuolated cytoplasm (hematoxylin-eosin; original magnification: ×400).
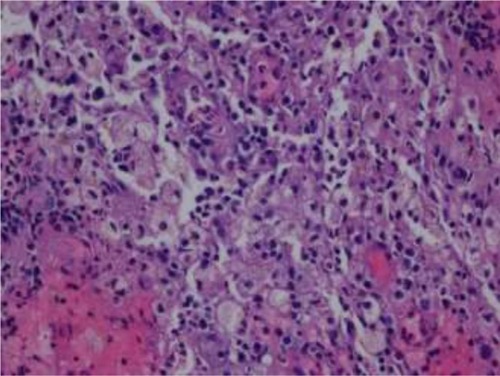
Figure 6 Some of infiltrating histiocytes show hemophagocytic activity characterized by intracytoplasmic nuclear debris (hematoxylin-eosin; original magnification: ×400).
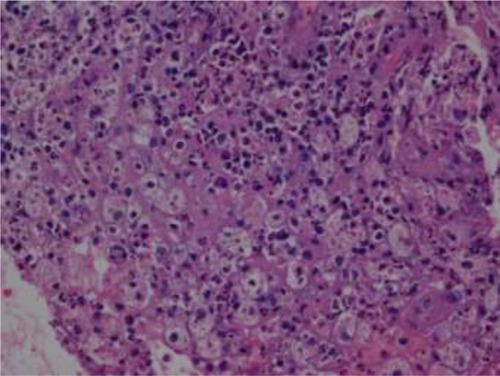
Figure 7 Small- and medium-sized vasculitis characterized by lymphocytic and neutrophilic infiltrate in wall of subcutaneous vessels obtained from sural nerve biopsy (hematoxylin-eosin; original magnification: ×200).
Discussion
Scleritis is a destructive ocular inflammation mostly associated immune-mediated cause with or without systemic collagen vascular disease. It is very important in differentiating between infectious and noninfectious scleritis by using predisposing factors, clinical sign, symptoms, and diagnostic tools.Citation1 The two diseases most often associated are granulomatosis with polyangiitis and rheumatoid arthritis.Citation2 The others were inflammatory bowel disease, relapsing polychondritis, systemic lupus erythematosus, polyarteritis nodosa, giant cell arteritis, Behçet’s disease, seronegative spondyloarthropathies, sarcoidosis, systemic sclerosis, IgA nephropathy, and gout.Citation3,Citation4 Watson et alCitation5 classified the scleritis disorder into anterior and posterior types based upon the anatomical distribution of the disease. Anterior scleritis is further subdivided into diffuse, nodular, necrotizing with and without inflammation by ocular examination. However, scleral biopsy could give the clinician more useful information for the correct diagnosis such as in this case. Scleral biopsy showed necrobiotic xanthogranulomatous inflammation.
Xanthogranulomas are granulomas, in which histiocytes are filed with a lipid yellow material,Citation6 both clinically for superficial lesions and on gross specimens examination of resected specimens. Necrobiotic xanthogranuloma was first described by Kossard and WinkelmannCitation7 in 1980. They found 8 patients who had multiple xanthomatous plaques and subcutaneous nodules in periorbital area, flexures, and trunk. All patients had dysproteinemia, mostly a monoclonal IgG paraprotein. Laboratory abnormalities commonly included monoclonal gammopathy, increased erythrocyte sedimentation rate, and leukopenia. After that, in 1991 Rose et alCitation8 reported three patients presented with proptosis and subcutaneous nodule at eyelid. Histopathological finding revealed foamy cytoplasm, giant cell, and lymphocytic infiltration. These were characteristics of xanthogranulomatous inflammation, which represent the necrobiotic type.
Since then, many literaturesCitation9–Citation11 have described this problem and classified it into 4 following subtypes from histopathological findings, laterality, systemic associations, and prognosis: 1) adult onset xanthogranuloma which is often associated with hematological disorder, 2) adult onset asthma and periocular xanthogranuloma which is rare and associated with asthma, 3) necrobiotic xanthogranuloma which is often associated with paraproteinemia, multiple myeloma or lymphoproliferative disorders, and 4) Erdheim–Chester disease which is associated with vital organ involvement resulting in death. One common thing in all subtypes is xanthoma cells which are mononucleated foamy histiocytes with or without Touton giant cells. In addition, the earlier literatures reported disorder only in orbit and eyelid.
Later on, the literatures have begun to report that a group of patients with necrobiotic xanthogranuloma had decreased vision, proptosis, scleritis, and uveitis. Some patients had no systemic causes,Citation12,Citation13 while some patients had paraproteinemiaCitation14 and leukemia.Citation15 Ugurlu et al reported a large series of necrobiotic xanthogranuloma with ocular and systemic involvement.Citation16 They found that 81% had lesions of the ocular adnexa, 90% were bilateral, that included eye lids, skin lesions, proptosis, abnormal epibulbar tissue, episcleritis, keratitis, blepharoptosis, and restricted ocular motility. Approximately 23% were not related with any systemic disease.
One interesting case report by Alkatan and Al-Abdullah,Citation17 a case of necrobiotic xanthogranuloma with bilateral scleritis and orbital involvement was first diagnosed as Wegener’s granulomatosis. Necrobiotic xanthogranuloma was definitely diagnosed after clinical and histopathological reviews later. This means both diseases have something similar that includes clinical or histopathological findings.
Granulomatosis with polyangiitis (GPA) or Wegener’s granulomatosis has classic triads including vasculitis of respiratory tract, glomerulonephritis, and systemic or necrotizing vasculitis. Eye involvement is found in 15% of patients at the first manifestation and in up to 50% of patients during active disease.Citation18,Citation19 The most common eye problem is orbital involvement (45%–70%), followed by scleritis (40%), retinal vasculitis (20%), uveitis (10%), and uncommon ischemic optic neuropathy.Citation20,Citation21 The diagnosis requires tissue biopsy, chest x-ray, urinalysis unstable angina, ESR, C-reactive protein test and ANCA. A positive biopsy is very useful to confirm the diagnosis of GPA. The histological features of GPA are granulomatous foci, tissue necrosis, plasma cells, and infiltration with neutrophils and eosinophils, small vessels vasculitis, and microabscess.Citation22–Citation25
To the best of our knowledge, this case report first identified the relationship between necrobiotic xanthogranuloma scleritis and granulomatosis with polyangiitis. Early diagnosis of GPA is very important as it enables the appropriate treatments such as immunosuppressive therapy for reducing the risk of progression of the disease early and the involvement of other vital organs which could possibly deteriorate the prognosis dramatically.
Conclusion
Necrobiotic xanthogranuloma scleritis is an uncommon finding; however, it could be an early presentation of granulomatosis with polyangiitis. The multidisciplinary team is useful and important for taking care of these patients.
Disclosure
The authors report no conflicts of interest in this work.
References
- MurthySIReddyJCSharmaSSangwaVSInfectious scleritisCurr Ophthamol Rep20153147157
- SmithJRMackensenFRosenbaumJTTherapy insight: scleritis and its relationship to systemic autoimmune diseaseNat Clin Pract Rheumatol20073421922617396107
- TappeinerCWalscheidKHeiligenhausADiagnosis and treatment of episcleritis and scleritisOphthalmology20161139797810
- DubordPJChalmersAScleritis and episcleritis: diagnosis and managementFocal Points: Clinical Modules for OphthalmologistSan FranciscoAmerican Academy of Ophthalmology1995 module 9
- WatsonPGHayrehSSAwdryPNEpiscleritis and scleritisBr J Ophthalmol19685232782795650814
- CozzuttoCCarboneAThe xanthogranulomatous process. Xanthogranulomatous inflammationPathol Res Pract1834395402
- KossardSWinkelmannRKNecrobiotic xanthogranuloma with paraproteinemiaJ Am Acad Dermatol1980332572707451693
- RoseGEPatelBCGarnerAWrightJEOrbital xanthogranuloma in adultsBr J Ophthamol199175680684
- Sivak-CallcottJARootmanJRasmussenSLAdult xanthogranulomatous disease of the orbit and ocular adnexa: new immunohistochemical findings and clinical reviewBr J Ophthalmol200690560260816622091
- GuoJWangJAdult orbital xanthogranulomatous disease: review of the literatureArch Pathol Lab Med2009133121994199719961259
- RaynerSADuncombeASKeefeMTheakerJMannersRMNecrobiotic xanthogranuloma occurring in an eyelid scarOrbit200827319119418569827
- PeymanAWalshNGreenPDoreyMWSeamoneCPasternakSNecrobiotic xanthogranuloma associated with necrotizing scleritisAm J Dermatopathol201234664464722814320
- LavricAAgrawalRPavesioCA case of necrobiotic xanthogranuloma presenting as bilateral posterior scleritisJ Immunol Inflamm201613
- WilhelmusKRYenMTRiceLFontRLNecrobiotic xanthogranuloma with posterior scleritisArch Ophthalmol20061245
- MohseninASinardJHuangJJNecrobiotic xanthogranuloma and chronic lymphocytic leukemia of the conjunctiva masquerading as scleritis and uveitisClin Ophthalmol201262045204723271884
- UgurluSBartleyGBGibsonLENecrobiotic xanthogranuloma: long-term outcome of ocular and systemic involvementAm J Ophthalmol2000129565165710844059
- AlkatanHMAl-AbdullahAEAOrbital necrobiotic xanthogranuloma: a case reportInt J Pathol Clin Res201512
- HoffmanGSKerrGSLeavittRYWegener’s granulomatosis: an analysis of 158 patientsAnn Intern Med199211664884981739240
- IsmailovaDSNovikovPIGrushaYOAbramovaYVBulanovNMMakarovEAThe frequency of ophthalmologic manifestations of granulomatosis with polyangiitis (Wegener’s) and their relationship to systemic diseasesTer Arkh20178956973
- UrseaRNussenblattRBRonaldRBWegener’s granulomatosis, a patient education monograph prepared for the American Uveitis Society22003
- PakrouNSelvaDLeibovitchIWegener’s granulomatosis: ophthalmic manifestations and managementSemin Arthritis Rheum200635528429216616151
- AhmedMNiffeneggerJHJakobiecFADiagnosis of limited ophthalmic Wegener granulomatosis: distinctive pathologic features with ANCA test confirmationInt Ophthalmol200828354617589807
- IsaHLightmanSLuthertPJRoseGEVerityDHTaylorSRHistopathological features predictive of a clinical diagnosis of ophthalmic granulomatosis with polyangiitis (GPA)Int J Clin Exp Pathol20125768468922977665
- MullerKLinJHOrbital granulomatosis with polyangiitis (Wegener granulomatosis): clinical and pathologic findingsArch Pathol Lab Med201413881110111425076302
- KalinaPHLieJTCampbellRJGarrityJADiagnostic value and limitations of orbital biopsy in Wegener’s granulomatosisOphthalmology19929911201241741123