
Abstract
Walker–Warburg syndrome (WWS) is a disorder characterized by ocular and brain malformations, and congenital muscular dystrophy. Retinal malformations are common in WWS; however, bilateral retinal detachment is a rare occurrence. We present a case of a newborn baby delivered at 36+3 weeks, who was the first living child of consanguineous parents of Turkish origin. On antenatal anomaly scans, the fetus had hydrocephalus that had increased throughout pregnancy, and a diagnosis of hydrancephaly was made at 36 weeks of gestation. Hypotonia, cleft lip and palate, poor suck and absent gag reflex were noted at birth. Ophthalmic examination at the age of 2 days revealed bilateral funnel retinal detachment. B-scan ultrasonography confirmed these findings, and magnetic resonance imaging (MRI) of the brain was performed at the age of 13 days to establish a diagnosis. The MRI showed lissencephaly, hydrocephalus and thin rim of brain parenchyma, with a cobblestone appearance of the cortex and pontine and cerebellar hypoplasia, consistent with the diagnosis of WWS. The infant deteriorated and died at 39 days of age from complications associated with the brain anomalies. In summary, bilateral retinal detachment is extremely rare and in association with hydrocephalus and posterior fossa anomalies strongly suggests the diagnosis of WWS.
Introduction
Walker–Warburg syndrome (WWS) is a rare congenital muscular dystrophy (CMD) characterized by severe cranial and brain malformations and ocular abnormalities.Citation1 It is an autosomal recessive disease caused by mutations of glycoprotein enzymes important for muscle integrity and neuronal migration.Citation2,Citation3 WWS has a very poor prognosis, with a median life expectancy of only 9 months, mainly due to brain anomalies.Citation4 Ocular abnormalities associated with WWS are common and include corneal opacities, microphthalmia, buphthalmos, glaucoma, iridocorneal malformations, cataract and retinal malformations such as retinal dysplasia and detachment.Citation4–Citation7
Case report
We report the case of a newborn delivered by semi-elective cesarean section at 36+3 weeks. The infant was the first living child of consanguineous parents of Turkish origin. The family had one previous intrauterine death at 25 weeks of gestation and a medical termination of pregnancy at 14 weeks of gestation due to hydrocephalus.
On antenatal anomaly scans, the fetus had hydrocephalus that had increased throughout pregnancy, and a diagnosis of hydrancephaly was made at 36 weeks of gestation. The eyes had not been examined on antenatal ultrasound. The birth weight was 3125 g, and Apgar scores were 8 at 1 minute, 9 at 5 minutes and 10 at 10 minutes.
Hypotonia, cleft lip and palate, poor suck and absent gag reflex were noted at birth. A cranial ultrasound performed at birth revealed massive ventriculomegaly. Computed tomography scan of the head confirmed massive dilatation of lateral and third ventricles causing a mass effect on the posterior fossa which was consistent with hydrancephaly.
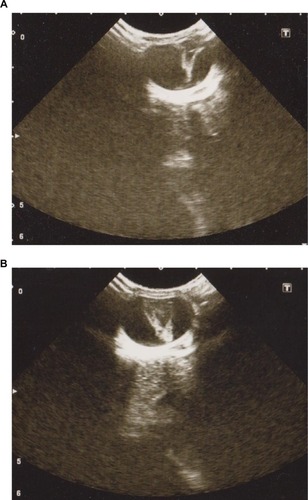
A routine ophthalmic examination was requested and performed at 2 days of age. Anterior segment examination revealed clear corneas of normal size. Indirect ophthalmoscopy showed bilateral funnel retinal detachment which was confirmed on B-scan ultrasonography ().
Figure 1 Ocular B-scan ultrasonography (transverse section) at 2 days of age showing funnel retinal detachment of right eye (A) and left eye (B).
Magnetic resonance imaging (MRI) of the brain performed at the age of 13 days confirmed the presence of bilateral retinal detachment () and showed marked enlargement of the lateral and third ventricles, deficiency of the septum pellucidum and thin rim of brain parenchyma with lissencephaly and a cobblestone appearance of the cortex and pontine and cerebellar hypoplasia ().
Figure 2 Axial T2-weighted image showing bilateral retinal detachment.
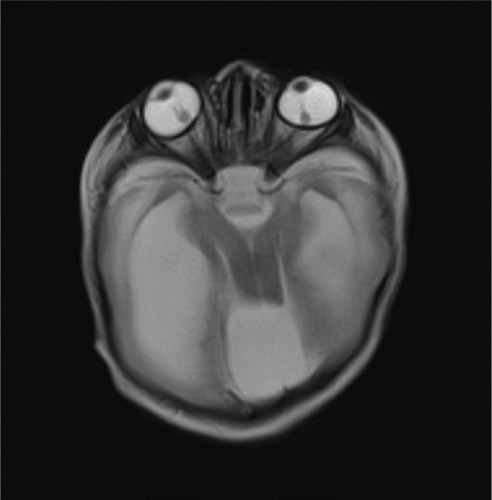
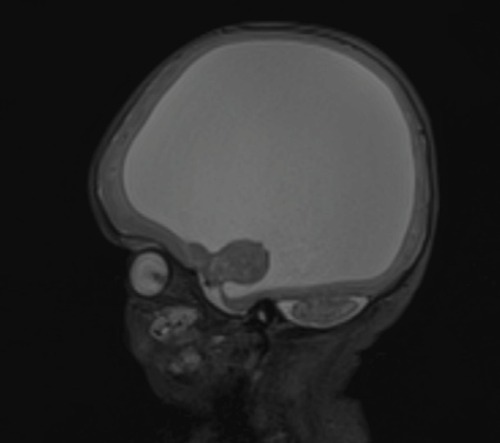
Figure 3 Sagittal T2-weighted image showing thin rim of brain parenchyma, with a cobblestone appearance of the cortex and pontine and cerebellar hypoplasia.
Comparative genomic hybridization with 60,000 probes did not detect any chromosomal imbalance. Due to the very poor prognosis, a ventriculo-peritoneal shunt was not considered appropriate. The infant deteriorated and died at 39 days of age. Postmortem examination was not performed.
Informed written consent was obtained from the patient’s guardian for publication of case details and images.
Discussion
WWS is an autosomal recessive disorder characterized by ocular abnormalities, brain malformations and CMD. The diagnostic criteria as described by Dobyns et al include type II lissencephaly, cerebellar malformations, retinal abnormalities and CMD.Citation1 WWS is caused by an abnormal glycosylation of alpha-dystroglycan.Citation3 Mutations of POMT1, POMT2, POMGnT1, FKRP, Fukutin and LARGE genes have been reported, but in many cases a genetic association is not found.Citation2 WWS has been reported in both consanguineous and non-consanguineous families.Citation8,Citation9 The occurrence in consanguineous families with none of the parents being affected is consistent with the autosomal recessive mode of transmission, despite no genetic defect being identified in our case.
In our report, a detailed ultrasound examination of the eyes had not been performed antenatally. The clinical appearance on indirect ophthalmoscopy of bilateral funnel retinal detachment was confirmed on B-scan ultrasonography and MRI of the brain. Ocular abnormalities associated with WWS are common, but bilateral retinal detachment is a rare occurrence. To our knowledge, only six cases of bilateral retinal detachment associated with WWS have been reported in the literature to date, all being diagnosed prenatally.Citation9–Citation14 These reports suggest that retinal detachment in WWS is visible on ultrasound as early as 24 weeks of gestation.Citation12 Unilateral retinal detachment was also reported in association with WWS.Citation5,Citation8,Citation15,Citation16 Previously reported histological studies have shown retinal structures in different stages of differentiation varying from well-developed rosettes to primitive photoreceptor outer segments.Citation5 A recent report of optical coherence tomography (OCT) in a case of retinal dysplasia associated with WWS showed the absence of the foveal pit, with laminar structure of the outer retinal layer and indistinct laminar structure of the inner retinal layer,Citation17 in accordance with previously described histology. Moreover, this OCT study suggested a degree of Müller cells dysplasia contributing to retinal dysplasia.Citation17
Conclusion
In summary, congenital retinal abnormalities are common in WWS, but bilateral retinal detachment is a rarer ocular manifestation, and it is identifiable on prenatal ultrasound as early as 24 weeks of gestation. The presence of hydrocephalus and posterior fossa anomalies should alert the diagnosis of WWS. Further studies are necessary for a better understanding of the range and mechanisms of retinal malformations associated with WWS.
Disclosure
The authors report no conflicts of interest in this work.
References
- DobynsWBPagonRAArmstrongDDiagnostic criteria for Walker-Warburg syndromeAm J Med Genet19893221952102494887
- Akasaka-ManyaKManyaHEndoTMutations of the POMT1 gene found in patients with Walker-Warburg syndrome lead to a defect of protein O-mannosylationBiochem Biophys Res Commun20043251757915522202
- van ReeuwijkJJanssenMvan den ElzenCPOMT2 mutations cause alpha-dystroglycan hypoglycosylation and Walker-Warburg syndromeJ Med Genet2005421290791215894594
- RhodesREHattenHPJrEllingtonKSWalker-Warburg syndromeAJNR Am J Neuroradiol19921311231261595429
- GerdingHGullottaFKuchelmeisterKBusseHOcular findings in Walker-Warburg syndromeChilds Nerv Syst1993974184208306359
- BornemannAPfeifferRBeinderEThree siblings with Walker-Warburg syndromeGen Diagn Pathol19961415–63713758780938
- RehanyUSegalZIRumeltSCongenital unilateral buphthalmos in Walker-Warburg syndrome: a clinicopathological studyEye (Lond)199913Pt 677878010707144
- DenisDGambarelliDLucianiAAyméSPhilipNSaraccoJBWalker-Warburg syndrome: a report of 3 casesOphthalmologica199320731131168278176
- Brasseur-DaudruyMVivierPHIckowiczVEurinDVerspyckEWalker-Warburg syndrome diagnosed by findings of typical ocular abnormalities on prenatal ultrasoundPediatr Radiol201242448849022002842
- FarrellSAToiALeadmanMLDavidsonRGCacoCPrenatal diagnosis of retinal detachment in Walker-Warburg syndromeAm J Med Genet19872836196243122570
- ChitayatDToiABabulRPrenatal diagnosis of retinal nonattachment in the Walker-Warburg syndromeAm J Med Genet19955643513587604843
- BlinGRabbéAAnsquerYMeghdicheSFloch-TudalCMandelbrotLFirst-trimester ultrasound diagnosis in a recurrent case of Walker-Warburg syndromeUltrasound Obstet Gynecol200526329729916082720
- StriginiFVallerianiACecchiMPrenatal ultrasound and magnetic resonance imaging features in a fetus with Walker-Warburg syndromeUltrasound Obstet Gynecol200933336336519222032
- ShenOZuckermanSCohenPRabinowitzRPrenatal sonographic diagnosis of retinal nonattachmentJ Ultrasound Med20143361095109724866619
- KhalafSSTareefRBWalker-Warburg syndromeJ AAPOS200610548648817070491
- ParkSHShinSYWalker-Warburg syndrome manifesting as leopard spot retinopathy, retinal detachment, and microphthalmiaJ Pediatr Ophthalmol Strabismus Epub2009102
- ManoNMitsutsujiTYoshikawaYOptical coherence tomography in an infant with Walker-Warburg syndromeCase Rep Ophthalmol20156221021526265907