
Abstract
Congenital infiltrating lipomatosis of the face (CILF) is a rare lipomatous lesion, commonly seen in childhood, and it is characterized by collections of mature, unencapsulated adipose tissues that infiltrate facial soft and hard tissues. The lesion is seen as an overgrowth of bone and soft tissue and is generally present clinically as slow-growing painless masses. In this case report, we described one case of CILF, which is one of the first cases reported in Ghana and Africa as a whole, along with a literature review on the diagnosis and current treatment strategies.
Introduction
Congenital infiltrating lipomatosis of the face (CILF) is a very rare lipomatous lesion with <60 reported cases in literature.Citation1–Citation3 CILF is nonhereditary and usually seen in childhood, causing unilateral facial skeletal hyperplasia, and it is histologically characterized by collections of mature, unencapsulated adipose tissues that infiltrate facial soft and hard tissues.Citation1,Citation4–Citation7 The primary concern in CILF is usually esthetics and the high rate of recurrence after surgical excision, as patients present with normal psychomotor development, and there is no sex predilection.Citation7,Citation8 In this case report, we present an additional case of CILF, which is one of the first cases reported in Ghana and Africa as a whole, along with a discussion on the diagnosis and treatment of CILF, with the aim of providing information toward the management of this rare condition.
Case report
A 9-year-old male patient presented with a painless right facial swelling, which had been present since birth and had progressively been increasing in size. Examination revealed facial asymmetry with a right hemifacial swelling spanning from the lower border of the right mandible to the inferior right lower eyelid measuring ~10×15 cm. There was enlargement of the right ear and a bulge on the right parietal scalp. The lesion was soft, non-tender and mobile with hyperpigmentation of the postauricular skin. There was deviation of the lip and nose to the left with obliteration of the right nasolabial sulcus indicating a right facial palsy. Oral examination revealed right-sided lip and tongue enlargement, right palatal bulge, right-sided dental anarchy with anterior open bite and calculus deposition.
Computed tomography (CT) of the head region showed a large lipomatous transformation of the right side of the face, involving the subcutaneous layer and the right parotid gland, with extension into the right masticator space. The tragus of the right ear also showed lipomatous infiltration. The lesion covered an area of ~13.8×8.5 cm. Evidence of significant hyperplasia of the right mandible was found with the width of the body of the mandible been 1.9 cm, while the contralateral side had a width of up to 0.9 cm. The lateral plate of the right pterygoid bone was also significantly hyperplastic, having a width of up to 0.9 cm compared to 0.2 cm of the contralateral side. The right maxilla was also significantly hyperplastic with a width of up to 2 cm compared to 1 cm on the contralateral side. There was also asymmetry of the face with disorganized dentition on the right side. No other asymmetric parts of the body were involved.
Written informed consent was obtained from the parent to have the case details and accompanying images published.
Discussion
Congenital infiltrating lipomatosis rarely affects the face and has been reported to have a predilection for the trunk and extremities.Citation9 The term congenital infiltrating lipomatosis of the face was initially proposed by Slavin et al,Citation7 who were the pioneers to report on proliferating and infiltrating lesions of lipocytes that involved only the facial region. The main characteristics of CILF elucidated by Slavin et al included: 1) nonencapsulated tumors containing mature lipocytes; 2) fat infiltration of adjacent muscles and soft tissues; 3) absence of malignant characteristics; 4) absence of lipoblasts; 5) presence of fibrous elements and increased number of nerve bundles and vessels and 6) adjacent bone hypertrophy. CILF is classified under lipoma, and it is distinguished from liposarcoma by the absence of mitosis, lipoblastic proliferation and pleomorphism.Citation7 In CILF, mature lipocytes invade into adjacent tissues in the facial region, manifesting as hypertrophy of both hard and soft structures on the affected side of the face and usually presenting clinically as slow-growing painless masses.Citation1,Citation4–Citation7 The manifestation is always unilateral, and reported cases that described the site of the facial mass have shown that ~64% occur on the left.Citation10 In CILF patients who present for treatment at the adult stage, the condition progresses with gradual hyperplasia, while there is extensive hyperplasia in childhood patients (≤1 year of age).Citation11
Several studies have traced the etiology of CILF to postzygotic mutation, as pluripotent cells of embryonic origin are known to precipitate somatic defect under the influence of trauma, muscle metaplasia, hormones and irradiation.Citation12–Citation16 This triggers and accelerates the lipomatous change seen in CILF. The postzygotic mutation occurs in the PIK3CA gene in the affected tissues, as PI3K, which is encoded by PIK3CA, plays a critical role in regulating cell survival, motility, adhesion and proliferation.Citation17 A study done by Maclellan et alCitation17 showed that subcutaneous adipose tissue from affected areas of patients with CILF contains somatic activating mutations in PIK3CA. A further study that sought to determine if the overgrowth in subjects with CILF was caused by a postzygotic mutation in only the subcutaneous adipose tissue (one tissue type) or by the presence of mutant cells in each of the subject’s overgrown tissues also reported that all tissues (including stroma, adipose, muscle, bone, nerves, etc.) on the side of the face affected with CILF contained PIK3CA mutations.Citation18
It must however be noted that the same postzygotic mutations have been identified in vascular malformations, cancers and other disorders with overgrowth, collectively termed together with CILF as PIK3CA-related overgrowth spectrum (PROS), hence not surprising that several mosaic disorders are in the differential diagnosis of CILF.Citation19 Conditions like Parry–Romberg syndrome (progressive hemifacial hyperplasia atrophy) and hemifacial microsomia, which cause contralateral hypoplasia, need to be considered.Citation20 In addition, although hemifacial hyperplasia does not involve mucosal neuromas and mature lipocytic infiltration, it shares common features with CILF and must be noted.Citation19,Citation20 In conditions like facial angioma and angiolipoma, cutaneous capillary brush implicated in some patients with CILF has also been found.Citation21,Citation22 Lymphangioma has also been associated with diffuse swelling in the facial and neck area, although this is easily resolved with an MRI scan.Citation20,Citation22 Encephalocra-niocutaneous lipomatosis (ECCL) and proteus syndrome also have infiltrating lipomatosis as a feature. However, CILF unlike proteus syndrome usually presents at birth and does not involve areas outside the head and neck region. ECCL on the other hand manifests in the central nervous system in contrast to CILF.Citation22 Well-differentiated liposarcoma and lipoblastomatosis that involve fat tissue infiltration also need to be ruled out. Liposarcoma is associated with the presence of lipoblastic proliferation and large number of cell mitosis and pleomorphism, with lipoblastomatosis having the presence of fetal adipose tissue, which is absent in the histopathological examination of CILF tissue.Citation7,Citation22–Citation24 Facial location, congenital presentation, early eruption of deciduous and permanent teeth, macrodontism, adjacent dentoskeletal manifestations, proliferation of parotid gland on the affected side, macroglossia and specific histological features are possible results for CILF.Citation7,Citation23,Citation25–Citation27
The diagnosis of CILF in our case was based on the patient’s medical records, clinicopathological manifestations and imaging features from CT (–). The CT scan was particularly useful in demonstrating the lipomatous nature of mass, osseous changes and their exact anatomic location and relationship to surrounding structures prior to surgery. Diagnosis of CILF was however confirmed by histopathology. The lesion was histologically characterized by sheets or lobules of mature normal adipocytes infiltrating trabecular bone, muscle fibers and salivary glands.Citation28,Citation29
Figure 1 Lipomatous infiltration of the right side of the face, including the parotid gland and masticator space.
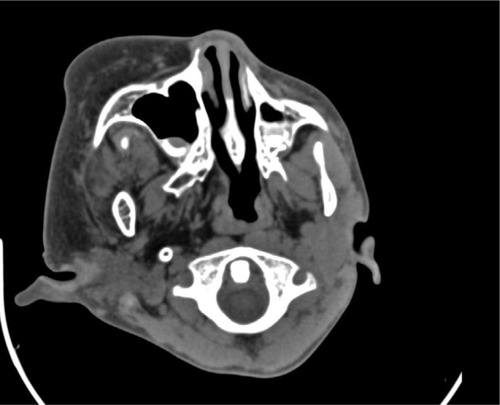
Figure 2 CT scan showing the enlarged pterygoid.
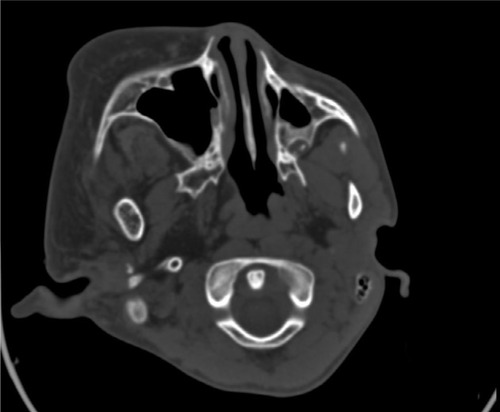
Figure 3 CT scan showing the enlarged right mandible.

Figure 4 CT scan showing the enlarged maxilla.

Figure 5 Volume rendering technique showing radiolucent fat and facial deformity.

Bone changes reported in CILF cases include hypertrophy of the skull, hypertrophy of the zygomatic bone, cervical vertebrae, acceleration of dentoskeletal growth, hemimandibular hypertrophy and sclerosis.Citation30–Citation33 These changes in bone appear to be associated with periosteal irritation associated with the overlying mass, regional malformation of mesenchyme affecting bone and soft tissues or increased vascularity.Citation30,Citation33,Citation34 Li et alCitation35 in their review of 59 reported cases of CILF noted that the bony asymmetry appears to increase with age, with the adipose tissue infiltrating into surrounding tissues and causing pterygoid gland and muscles (such as pterygoid plate and massetter and temporalis muscles) involvement, as reported in our cases.
The major concern in the treatment of CILF is the high rate of recurrence after surgical excision although the tumor is benign, with a recent study reporting as high as 79% rate of recurrence.Citation1,Citation8,Citation35 As a result, multiple surgeries are needed for cosmetic reasons, and when necessary, osseous reduction operations of the maxilla and mandible are performed.Citation21,Citation35,Citation36 Based on the esthetic requirement of the patient, a multidisciplinary approach that involves surgeons, clinicians, dentists, psychologists and geneticists may be ideal.Citation22,Citation29,Citation37 The high rate of recurrence may be the result of incomplete resection, as these fatty lesions are histologically benign, and as such, the value of aggressive extirpation needs to be weighed against the facial nerve damage and the likelihood of the resultant deformity.Citation38
Tracy et al in 2013 reported a conservative approach involving targeted chemotherapy and surgical resection in the management of CILF. The use of celecoxib and imatinib in personalized targeted chemotherapy was associated with improved facial symmetry without evidence of disease progression, thus paving the way for the exploration of this synergistic approach toward the management of this rare condition.Citation41 Conservative approach has also been reinforced by several authors on the backdrop of the benign nature and critical location of CILF despite the associated high rate of recurrences.Citation23,Citation28,Citation39
A recent study in 2017 by Kalantary et alCitation40 proposed a new multistep surgical approach toward the management of CILF. This involves initial debulking to correct the soft tissue asymmetry, followed by orthognathic surgery to correct the skeletal asymmetry, dental problems and associated malocclusion, cautioning however that each patient needs to be evaluated for this additional surgery on the bony level before carrying out this step, and finally bimaxillary procedure and genioplasty. The surgery was successfully performed when the patient was 14 years (after puberty), with no record of clinical recurrence at the time of publication (patient was 18 years then).
In addition, considering the implication of PIK3CA gene mutation in the pathogenic theory of CILF, inhibitors of PI3K, which are currently been used in clinical trials involving cancer patients, may play a role in CILF patients.Citation17 PI3K inhibitors may therefore be tested for CILF patients in clinical trials in the near future.Citation35
An area of contention in the treatment of CILF is the timing of surgical excision. Slavin et alCitation7 in their earlier studies encouraged early aggressive surgery in a bid to improve facial appearance and control the overgrowth. Van Wingerden et alCitation41 disagreed with this approach on the basis of possible risk to nerve, which is compounded by multiple procedures and the likelihood of recurrence. They however admitted that the postponement of surgery may make the procedure more extensive, along with associated psychosocial issues. They further argued that the delay in surgery lowers the chances of damaging the facial nerve, may require fewer procedures and there will be more mature contralateral cheek for comparison during the procedure. Padwa and MullikenCitation21 also sided with Van Wingerden et al, observing that growth hormone most probably has a role in recurrences and that any effort to reduce the mass before the end of adolescence is bound to fail due to recurrences. Based on our study, we advocate that extensive resection should be delayed as long as possible, with due consideration to psychosocial issues. Elevation of the ptotic upper lip, liposuction and the excision of mucosal neuromas are among the temporary measures that can be taken to improve asymmetry in young patients with minimal risk.Citation21
Conclusion
CILF is a rare congenital disorder, histologically characterized by sheets or lobules of mature normal adipocytes infiltrating trabecular bone, muscle fibers and salivary glands. The proximity of vital anatomic structures and the diffuse nature of the disease pose a greater challenge to surgical resection. In this article, we reported an additional case of CILF and did an extensive review of the diagnosis and treatment of the condition, providing information toward the management of this rare disorder.
Disclosure
The authors report no conflicts of interest in this work
References
- RajeswaranRMurthyJChandrasekharanAJosephSCase Report: Congenital infiltrating lipomatosis of faceIndian J Radiol Imaging200818430619774187
- KamalDBretonPBouletreauPCongenital infiltrating lipomatosis of the face: Report of three cases and review of the literatureJ Craniomaxillofac Surg201038861061420338773
- UrsABAugustineJKumarPAroraSAggarwalNSultanaNInfiltrating lipomatosis of the face: A case seriesJ Nat Sci Biol Med20134125225723633877
- EnzingerFMWeissSWBenign lipomatous tumorsSoft Tissue Tumors199St Louis, MOCV Mosby1983
- KeramidasTLagogiannisGVlachouVKatsikerisNCongenital infiltrating lipomatosis of the face with associated involvement of the TMJ structures. Case report and review of the literatureJ Craniomaxillofac Surg2012408750756622425497
- Flores-SarnatLCongenital infiltrating lipomatosis of the face: recognition and pathogenesisNeuropediatrics2012430634634823129437
- SlavinSABakerDCMccarthyJGMufarrijACongenital infiltrating lipomatosis of the face: clinicopathologic evaluation and treatmentPlast Reconstr Surg19837221581646192455
- HeymansORonsmansCCongenital infiltrating lipomatosis of the faceEur J Plast Surg2005283186189
- ScherlMPSomPMBillerHFShahKRecurrent infiltrating lipoma of the head and neck. Case report and literature reviewArch Otolaryngol Head Neck Surg198611211121012123755996
- LiYChangGSiLCongenital Infiltrating Lipomatosis of the Face: Case Report and Literature ReviewAnn Plast Surg20188018328846548
- KangNRossDHarrisonDUnilateral hypertrophy of the face associated with infiltrating lipomatosisJ Oral Maxillofac Surg19985678858879663580
- GörkenCAlperMBilkayUÇelikNSongürECongenital infiltrating lipomatosis of the faceJ Craniofac Surg199910436536810686886
- HaloiAKDitchfieldMPeningtonAPhillipsRFacial infiltrative lipomatosisPediatr Radiol200636111159116216953375
- ChenCMLoLJWongHFCongenital infiltrating lipomatosis of the face: case report and literature reviewChang Gung Med J200225319420012022741
- DonatiLCandianiPGrappoliniSKlingerMSignoriniMCongenital infiltrating lipomatosis of the face related to cytomegalovirus infectionBr J Plast Surg19904311241262155681
- PatelRVGondaliaJSCongenital infiltrating lipomatosis of the faceBr J Plast Surg1991442157158
- MaclellanRALuksVLViveroMPPIK3CA activating mutations in facial infiltrating lipomatosisPlast Reconstr Surg2014133112e19e25942115
- CoutoJAKonczykDJViveroMPSomatic PIK3CA mutations are present in multiple tissues of facial infiltrating lipomatosisPediatr Res201782585085428665924
- Keppler-NoreuilKMRiosJJParkerVEPIK3CA-related overgrowth spectrum (PROS): diagnostic and testing eligibility criteria, differential diagnosis, and evaluationAm J Med Genet A2015167A228729525557259
- KamalDBretonPBouletreauPCongenital infiltrating lipomatosis of the face: report of three cases and review of the literatureJ Craniomaxillofac Surg201038861061420338773
- PadwaBLMullikenJBFacial infiltrating lipomatosisPlast Reconstr Surg200110861544155411711926
- KimJEGottschallJABachmanRPNemzerLPuligandlaBSchauerGFacial infiltrating lipomatosis: physical, radiological, and histopathological findingsArch Otolaryngol Head Neck Surg2010136330130320231652
- MalikAJagmohanPThukralBBKhannaGRajniCongenital infiltrating lipomatosis of the face and neckActa Radiol200445555656015515519
- ÜnalOCirakBBekereciogluMKutluhanAUgraşSTaliTCongenital infiltrating lipomatosis of the face with cerebral abnormalitiesEur Radiol200010101610161311044934
- de RosaGCozzolinoAGuarinoMGiardinoCCongenital infiltrating lipomatosis of the face: report of cases and review of the literatureJ Oral Maxillofac Surg198745108798833309227
- KeramidasTLagogiannisGVlachouVKatsikerisNCongenital infiltrating lipomatosis of the face with associated involvement of the TMJ structures. Case report and review of the literatureJ Craniomaxillofac Surg201240875075622425497
- Flores-SarnatLCongenital infiltrating lipomatosis of the face: recognition and pathogenesisNeuropediatrics201243634634823129437
- ShenoyARNairKKLingappaAShettyKSCongenital infiltrating lipomatosis of face: case report and review of literatureJ Indian Soc Pedod Prev Dent201533215625872637
- Pires FragaMFMelloDJorgeDPerinLFHeleneAFragaMFCongenital infiltrating lipomatosisJ Plast Reconstr Aesthet Surg20096212e561e56419124289
- BollingerBBone changes in diffuse congenital lipomatosisNeuroradiology19872911043822095
- BouletreauPBretonPFreidelMCongenital infiltrating lipomatosis of the face: case reportJ Oral Maxillofac Surg200058780781010883699
- MacmillanAROliverAJReadePCMarshallDRRegional macrodontia and regional bony enlargement associated with congenital infiltrating lipomatosis of the face presenting as unilateral facial hyperplasia. Brief review and case reportInt J Oral Maxillofac Surg19901952832862124599
- WylieEJKendallBCranio-vertebral bony changes in a case of congenital lipomatosisNeuroradiology19893143523532797429
- LachmanRSFinklesteinJMehringerCMMaenzaRCongenital aggressive lipomatosisSkeletal Radiol1983942482546867775
- LiYChangGSiLCongenital Infiltrating Lipomatosis of the Face: Case Report and Literature ReviewAnn Plast Surg20188018328846548
- KangNRossDHarrisonDUnilateral hypertrophy of the face associated with infiltrating lipomatosisJ Oral Maxillofac Surg19985678858879663580
- MahadevappaARaghavanVHRavishankarSManjunathGVCongenital infiltrating lipomatosis of the face: a case reportCase Rep Pediatr2012201213
- HaTVKleinmanPKFraireAMR imaging of benign fatty tumors in children: report of four cases and review of the literatureSkeletal Radiol19942353613677939836
- TracyJCKlementGLScottARInterdisciplinary management of congenital infiltrating lipomatosisInt J Pediatr Otorhinolaryngol201377122071207424035641
- KalantarySvan de CasteeleENadjmiNCongenital Infiltrating Lipomatosis of the Face: Case Report With Presentation of a New Multistep Surgical ApproachJ Oral Maxillofac Surg20187661334134329128477
- van WingerdenJJErlankJDBeckerJHLiposuction for congenital infiltrating lipomatosis of the facePlast Reconstr Surg19888169893375369