
Abstract
Background
Congenital saccular cyst of the larynx is a very rare cause of respiratory obstruction in the neonatal period and in older children. It can be a potentially life-threatening condition. It can also present less dramatically later in childhood as a voice disorder. Early diagnosis and treatment are very important to avoid the high mortality associated with undiagnosed cases.
Subjects and method
I report here two cases of laryngeal saccular cyst with different clinical scenarios. The first patient presented immediately after birth with respiratory problems and the second presented later at an older age. Both patients were managed with endoscopic excision.
Conclusion
Congenital saccular laryngeal cyst remains an important cause of respiratory obstruction in the neonate albeit being rare. It is amenable to treatment with minimally invasive procedures.
Introduction
Saccular cyst of the larynx is a very rare condition. When literature is reviewed, most of the articles are either case reports or limited case series.Citation1–Citation6 It could be congenital and present with symptoms immediately after birth or later during infancy and childhood or it can be acquired and present during adult life.Citation3,Citation7 Symptoms include respiratory obstruction, stridor, or change of voice.Citation3,Citation6 Here I report two cases of laryngeal saccular cyst with different clinical scenarios.
Case 1
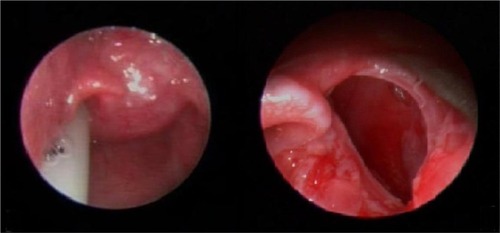
A full-term male neonate who was born by cesarean section at 39 weeks was noticed to have stridor immediately after birth. He was put on continuous positive airway pressure at age 45 minutes. At age 4 hours, he was intubated with endotracheal tube and put on mechanical ventilatory support because of worsening respiratory distress. The ENT was consulted 1 day after the patient birth. Examination revealed a morphologically normal looking neonate weighing 2.99 kg. Diagnostic bronchoscopy revealed a right supraglottic compressible cystic mass obstructing the view of both vocal cords with normal subglottic area (). CT scan showed a right laryngeal cystic mass which was 2.2 × 1.5 × 1.3 cm in dimension compromising the aerodigestive tract. The patient failed repeated attempts of weaning from mechanical ventilator and extubation of varying lengths throughout the 13 days following his birth. Informed consent was obtained and the patient was operated on at age 13 days. At operation, the patient was positioned and an operating laryngoscope was inserted and suspended. Xylocaine 1% with adrenaline 1:200000 was infiltrated around the cyst. Small incision was made using a round knife and then the cyst was completely enucleated using a blunt hook. The cavity was partially closed using vicryl 5/0. The baby was successfully extubated 48 hours after the procedure and remained stable thereafter with mild stridor. However, 2 weeks later the patient developed worsening stridor and became desaturated. He was reintubated and taken to the operation theater again. To our surprise the cyst appeared to have recurred. Re-excision of the newly formed cyst was done using the same procedure. The patient recovered well this time and he was extubated 2 days after the procedure. He was discharged from the hospital 2 weeks later. Follow-up as outpatient continued for more than 1 year and the baby remained symptom-free.
Figure 1 The saccular cyst before and after the first excision in case 1.
Case 2
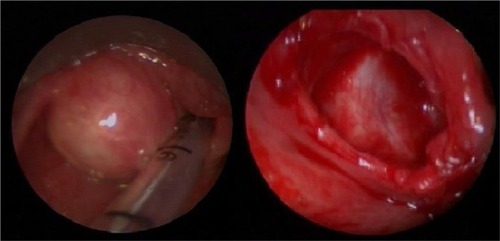
A 4-year-old girl was referred to our clinic with a history of dysphonia and stridor since infancy associated with occasional attacks of sudden arousal from sleep. Her parents were anxious because their daughter’s socialization appeared to be affected by this problem. Clinical assessment revealed an otherwise normal child with a clearly hoarse deep voice. Fiber-optic nasopharyngoscopy was done for her, which showed a rounded mass at the hypopharynx with normally looking mucosa obscuring the left vocal fold (). CT scan showed a 3 × 2.5 × 2.2 cm cystic lesion in the right side of the larynx. The patient underwent successful endoscopic excision of the cyst using the same technique as in case 1 under general anesthesia. Follow-up for more than 2 years showed complete resolution of the symptoms without any recurrence.
Figure 2 The cyst before and after excision in case 2.
Discussion
Congenital strider and respiratory obstruction can be caused by several conditions. These could be supraglottic, glottis, or subglottic conditions. Laryngomalacia is the commonest condition.Citation8 Other laryngeal causes include subglottic stenosis, vocal cord paralysis, laryngeal webs, hemangiomas, papillomas, and laryngeal clefts. Saccular cyst of the larynx remains a very rare cause of respiratory obstruction.Citation3 Diagnosis could be delayed due to the large array of causes of respiratory obstruction in neonates. Kristensen and Tveterås claim that almost 50% of the reported cases are diagnosed at autopsy.Citation9 In another study, Holinger found that the mean length of time from onset of symptoms to determination of the correct diagnosis by endoscopy was 4 months, varying from 1 day to 16 months.Citation10 That is a long time for the diagnosis and hence treatment of a potentially life-threatening condition. Our first case went through a period of endotracheal intubation and ventilatory support for 13 days interrupted with failed trials of extubation of varying lengths before surgical intervention.
Several epidemiological studies targeted the pediatric population to detect the incidence of dysphonia among them.Citation11–Citation14 A prevalence ranging from 6%–12% was reported by these studies. It is often caused by voice abuse.Citation15 The most commonly diagnosed lesions in the laryngoscopic examinations were vocal cord nodules and epidermal cysts.Citation15 Congenital causes of dysphonia account for only 7%.Citation16 Saccular cyst of the larynx remains a rare cause of dysphonia, in spite of the fact that dysphonia could be a common presenting symptom for it, especially in older children. In case 2, the child was brought to our clinic after her parents noticed a significant effect of the problem on their daughter’s socialization. This aspect of the problem was noted by some studies.Citation17,Citation18 It includes spectrum of psychosocial problems like sadness, anger, frustration, embarrassment, and negative perception by others.
Different procedures are being used to treat saccular cysts. Endoscopic needle aspiration, marsupialization, endoscopic extended ventriculotomy, and endoscopic radiofrequency ablation are all used in the treatment of this condition.Citation3,Citation19 Needle aspiration remains a temporary measure in life-threatening respiratory obstruction as recurrence is very high after this procedure.Citation6,Citation20 Prowse and Knight concluded that single-stage endoscopic marsupialization is an effective means of treatment after treating a mix of ten patients with ductal and saccular cyst.Citation21 CO2 laser is used effectively for marsupialization and vaporization of the cyst lining.Citation4,Citation22,Citation23 Kumar et al used radiofrequency ablation with success in a series of six cases.Citation24 Kirse et al successfully treated a series of four patients aged 1–7 weeks with endoscopic extended ventriculotomy.Citation19 An external approach is also used especially for large cysts protruding through the thyrohyoid membrane.Citation23 The best method of treatment is controversial as there are no studies comparing the different approaches, probably due to the rarity of cases. We managed our two patients with endoscopic excision. The first patient developed recurrence within a surprisingly very short time. It is difficult to conclude whether recurrence was related to the particular procedure that was used or to any other unforeseen factor.
Conclusion
Congenital saccular laryngeal cyst remains an important cause of respiratory obstruction in the neonate albeit being rare. It can be treated with minimally invasive procedures. Dysphonia in children should be well investigated and laryngoscopy should be regularly included in its assessment.
Ethical approval and consent
Written informed consent was obtained from the parents of both patients for publication of this case report and accompanying images. Ethical approval for the publication of this case was also obtained from the ethical committee of the Faculty of Medicine, Jazan University.
Disclosure
The author reports no conflicts of interest in this work.
References
- PrasadKCRanjanRKAgarwalSPrasadSCBhatJCongenital laryngeal saccular cyst: report of a case in an infantEar Nose Throat J2006851495116509245
- CivantosFJHolingerLDLaryngoceles and saccular cysts in infants and childrenArch Otolaryngol Head Neck Surg199211832963001554451
- TosunFSökenHOzkaptanYSaccular cyst in an infant: an unusual cause of life-threatening stridor and its surgical treatmentTurk J Pediatr200648217818016848124
- KinnunenIKlemiPGrenmanRSaccular laryngeal cysts. Three case studies and review of the literatureORL J Otorhinolaryngol Relat Spec200062210911110729802
- SennesLUImamuraRFrizzariniRHachiyaAChaguryAACongenital laryngeal saccular cystBraz J Otorhinolaryngol2012783137
- Zamfir-Chiru-AntonAGheorgheDCSaccular cyst with atypical presentationJ Med Life20169219920427453755
- BenoitCDayTLaryngeal saccular cystDiagn Ther Endosc200062919418493532
- ThurmondMCoteDNStridor in the neonate: laryngomalaciaJ La State Med Soc199614893753789150664
- KristensenSTveteråsKCongenital laryngeal cyst in infancy. A rare cause of life-threatening stridorORL J Otorhinolaryngol Relat Spec19864831501553714197
- HolingerLDEtiology of stridor in the neonate, infant and childAnn Otol Rhinol Laryngol1980895 Pt 13974007436240
- LecoqMDrapeFEpidemiological survey of dysphonia in children at primary school entryRev Laryngol Otol Rhinol19961174323325
- TavaresELBrasolottoASantanaMFPadovanCAMartinsRHEpidemiological study of dysphonia in 4-12 year-old childrenBraz J Otorhinolaryngol201177673674622183280
- CardingPNRoulstoneSNorthstoneKALSPAC Study TeamThe prevalence of childhood dysphonia: a cross-sectional studyJ Voice200620462363016360302
- KallvikELindströmEHolmqvistSLindmanJSimbergSPrevalence of hoarseness in school-aged childrenJ Voice2015292e260
- MartinsRHGHidalgo RibeiroCBFernandes de MelloBMZBrancoATavaresELMDysphonia in childrenJ Voice2012265674.e17674.e20
- ConnellyAClementWAKubbaHManagement of dysphonia in childrenJ Laryngol Otol2009123664264719216835
- ConnorNPCohenSBTheisSMThibeaultSLHeatleyDGBlessDMAttitudes of children with dysphoniaJ Voice200822219720917512168
- MornetECoulombeauBFayouxPAssessment of chronic childhood dysphoniaEur Ann Otorhinolaryngol Head Neck Dis2014131530931224986259
- KirseDJReesCJCelmerAWBrueggerDEEndoscopic extended ventriculotomy for congenital saccular cysts of the larynx in infantsArch Otolaryngol Head Neck Surg2006132772472816847179
- NarcyPBobinSManac’hYLaryngeal cysts in the newborn (9 cases) (author’s transl)Ann Otolaryngol Chir Cervicofac19799612881888533092
- ProwseSKnightLCongenital cysts of the infant larynxInt J Pediatr Otorhinolaryngol201276570871122376997
- MassothLJDigoyGPPaul DigoyGFlexible carbon dioxide laser-assisted endoscopic marsupialization and ablation of a laryngeal saccular cyst in a neonateAnn Otol Rhinol Laryngol2014123854154424646753
- AbramsonALZielinskiBCongenital laryngeal saccular cyst of the newbornLaryngoscope19849412 Pt 1158015826503577
- KumarSGargSSahniJKRadiofrequency ablation of laryngeal saccular cyst in infants: a series of six casesInt J Pediatr Otorhinolaryngol201276566766922398119