
Abstract
Introduction
Proptosis in children with acute-onset accompanied by signs of inflammation is commonly caused by orbital cellulitis, however, the possibility of rhabdomyosarcoma should always be considered by the clinician. This is a case report of a five-year-old boy presenting with an acute-onset of proptosis without a history of trauma and systemic infection. Our clinical differential diagnosis included orbital cellulitis and orbital rhabdomyosarcoma.
Purpose
To report a case of orbital cellulitis that clinically and radiologically mimics rhabdomyosarcoma.
Case presentation
A five-year-old boy presented with rapid-onset proptosis, periorbital edema, pain and visual loss in the left eye for two weeks without a history of trauma, upper respiratory tract infection, sinusitis or immunosuppression. Our clinical differential diagnosis includes rhabdomyosarcoma and orbital cellulitis. Complete blood count reveals a leukocytosis. Multislice computed tomography (MSCT) scan shows lesions involving the lateral orbit and the retro bulbar space. Antibiotics combination and adjunct anti-inflammatory intravenously shows excellent clinical resolution.
Conclusions
The study demonstrates difficulty in differentiating acute orbital cellulitis from rhabdomyosarcoma based on clinical findings. In addition, the case highlights that antibiotic combination of cephalosporin and aminoglycosides together with an adjuvant corticosteroid as an anti-inflammatory was effective in the case of acute orbital cellulitis.
Introduction
Orbital cellulitis is the most common serious eye infection in children.Citation1 Classic clinical findings include fever, leukocytosis, erythema, proptosis, chemosis, ptosis, restriction of and pain with ocular movement, loss of visual acuity and an afferent pupillary defect.Citation2–Citation5 Orbital cellulitis usually appears as acute-onset proptosis with signs of inflammation. However, in thosecircumstances, rhabdomyosarcoma should also be considered because it is also well known for its rapid unilateral proptosis.Citation6,Citation7 Orbital rhabdomyosarcoma is an orbital malignancy that is also common in children and has been reported to be responsible for 4% of all orbital masses in children.Citation6–Citation9 We report a case of orbital cellulitis that mimics rhabdomyosarcoma in a five-year-old boy with rapid-onset unilateral proptosis.
Case presentation
A five-year-old boy presented with rapid-onset proptosis and inferior displacement of the left globe for two weeks with associated with pain and discharge. There is history of the same condition in contralateral eyes that spontaneously heal without any treatment. It was previously treated with intravenous antibiotic for three days without any improvement. There was no history of trauma, upper respiratory tract infection, sinusitis or immunosuppression. The vital signs were within normal limit. The left eye showed proptosis, periorbital edema, chemosis in all quadrants of the conjunctiva and severe exposure keratopathy (). The swelling was tender and soft in consistency. Proptosis and displacement of the left globe to inferior were present. There was limitation of all movement of the globe. Examination of right eye was within normal limit. Based on history and clinical examination, clinical diagnosis of rhabdomyosarcoma was made with orbital cellulitis as differential diagnosis.
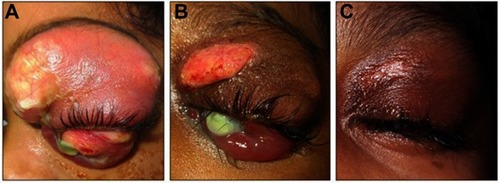
Figure 1 Baseline clinical presentation of left eye shows uniaxial proptosis with marked palpebral edema and conjunctival chemosis. Note the corneal ulcers.

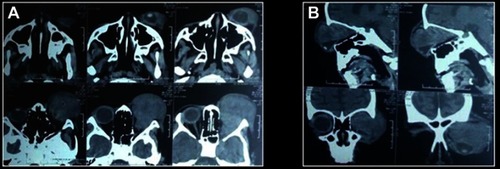
A multislice computed tomography (MSCT) scan showed lesions involving the lateral orbit () and the retro bulbar space (). Complete blood count showed leukocytosis with signs of infection. Systemic screening results for metastasis were negative. Consultation with ear, nose and throat (ENT) specialist confirm no clinical and radiological signs of sinusitis. A dental consultation also showed no odontogenic infection. Community acquired pneumonia (CAP) was confirmed by a pediatrician from clinical and thorax radiologic findings. A biopsy was not performed due to suboptimal condition for anesthetic procedure.
Figure 2 (A) Multi slice computed tomography (MSCT) scan of the orbit clearly shows right eye proptosis with lesion involving superior orbit, lateral orbit and retro bulbar space; (B) The lesion had variegated appearances and was indenting the globe.
On three days' administration of broad-spectrum cephalosporin antibiotic 750 mg twice a day, there is slight improvement of the patient's condition (). Patient shows resolution of clinical presentation after an additional intravenous administration of anti-inflammatory dexamethasone 5 mg twice a day for three days (). The patient made a good response after additional intravenous administration of broad-spectrum aminoglycoside antibiotic 40 mg twice a day for one week (). Simultaneously with intravenous therapy, an alpha receptor antagonist sympathomimetic and antibiotic were given topically to prevent further damage to the anterior segment of eyeball. After three weeks' therapy, the globe recovered, proptosis and displacement disappeared and ocular motility became normal. The visual prognosis was poor but with topical treatment, the ocular surface began to show better results. The patient’s legal guardian signed the written informed consent for publication of the case details and accompanying images. Institutional approval was not necessary.
Figure 3 (A) Clinical improvement after three days. (B) Resolution of proptosis, chemosis and edema after adjuvant intravenous corticosteroid. (C) The palpebral could close after three weeks’ therapy with antibiotics combination and corticosteroid.
Discussion and conclusion
Proptosis is an anterior displacement of the globes due to a space-occupying lesion in the orbit.Citation10 The causes in children were different from adults. Orbital cellulitis is known to be the most common cause of proptosis among children.Citation11 Other causes of proptosis in children include: developmental, vascular malformations, inflammations, and neoplasms.Citation12 Even though orbital cellulitis is the most common cause, childhood proptosis needs special attention as it is commonly caused by malignant lesion and at least threatens vision. In children presenting with acute rapid-onset unilateral proptosis with signs of inflammation, the possibility of rhabdomyosarcoma should always beconsider.
Rhabdomyosarcoma is the most common primary orbital malignancies in children. The onset is five to seven years. The classic clinical picture is sudden onset and rapid progression of unilateral proptosis with inferior or inferior temporal displacement of the globe.Citation13 Moreover, early signs and symptoms of orbital cellulitis include fever, lethargy, headache, rhinorrhea, eyelid edema, orbital pain and tenderness on palpation. Proptosis, chemosis and limited ocular movement suggest orbital involvement.Citation14
Acute, rapidly progressive proptosis that presents in this case, raises a high suspicion of orbital rhabdomyosarcoma; notwithstanding, associated pain does not eliminate orbital cellulitis as a differential diagnosis. Based on complete blood count, leukocytosis with signs of infection occured. It is known that sinusitis is the most common cause of bacterial cellulitis, consequently once it is suspected, orbital imaging is indicated to confirm orbital involvement, to document the presence and extent of sinusitis and subperiosteal abscess and also to rule out a foreign body in the patient with a history of trauma.Citation14 Some examinations should be done to rule out causes of infection, such as nasopharyngeal, conjunctival and blood culture. These procedures were not performed in this case considering the history of intravenous antibiotic. Accordingly, the result must be masked. The typical pathogens associated with acute sinusitis, including Streptococcus pneumoniae, Streptococcus pyogenes, Staphylococcus aureus, Haemophilus influenza, Moraxella catarrhalis, and nonhemolytic streptococci (including the Streptococcus milleri group) were common causes of orbital cellulitis.Citation5 Etiology varies with age, in children younger than nine years old it is generally caused by single aerobic pathogen. In older children and adults, S. pneumoniae, S. pyogenes, S. aureus, and various anaerobic species are common. Gram-negative organisms are found primarily in immunosuppressed patients.Citation14
A study by Ferguson and McNabb shows that in 56% of their patients that had blood cultures none had positive results. Based on their study, positive results more likely come from cultures taken from abscesses. They also noted that there was no correlation between etiology of orbital abscesses and cultures from conjunctiva.Citation15
MSCT scan imaging shows a well-defined, irregular, homogenous lesion in the left supero-temporal orbit and the retro bulbar space. Consultation with an ENT specialist confirmed no clinical and imaging signs of sinusitis. These findings lead to high possibilities of rhabdomyosarcoma. In CT scan, orbital RMS appears as a well-defined, homogenous, soft tissue mass that is isodense to muscles without bone destruction in earlier stages, but in advanced cases with bone destruction, there is invasion of surrounding structures and calcification. Focal hemorrhage or necrosis could give a heterogeneous appearance and moderate to marked general enhancement with contrast.Citation16
A consultation with a pediatrician was made before planning a biopsy. Pediatrician revealed an inadequate condition for anesthetic procedure due to CAP. Intravenous antibiotic of cephalosporin was administered. There is slight improvement after three days. The possibilities of orbital cellulitis reappeared. The most common cause of orbital cellulitis is bacterial infection. Bacterial infections of the orbit, originate from three primary sources: direct spread from adjacent sinusitis, dacryocystitis or dacryoadenitis, direct inoculation after trauma or skin infection, and hematologic spread from distant focus (eg, otitis media and pneumonia).Citation17
Garcia and Harris, in their prospective study, established that patients younger than nine years of age with small, medial subperiosteal abscesses of nondental origin who did not have evidence of optic nerve compression, gas within the abscess space, frontal sinusitis, or chronic sinusitis were successfully managed with medical therapy alone.Citation18
Adjuvant corticosteroid intravenously showed good response in one week for this case. The use of corticosteroid is still controversial in the treatment of orbital cellulitis. However, the use of systemic steroids under the coverage of appropriate antibiotics could decrease inflammatory response and does not have adverse effects. A prospective, randomized, comparative clinical study by Pushkar et al supports the beneficial effect of corticosteroids as an adjunct to antibiotics in acute bacterial orbital cellulitis. Addition of steroids helped in early resolution of inflammation and improved the overall outcome.Citation19
In addition to routine antibiotic, gentamycin was used. Intravenous combination antibiotics showed good clinical resolution. Surgical intervention was not performed; not only because of patient's suboptimal condition for anesthetic procedures, but also because of antibiotic clinical response.
A study by Chang et al showed that the most therapeutic antibiotic regimens for orbital cellulitis were a combination of aminoglycosides and penicillin and/or cephalosporin.Citation20 Bactericidal of these two antibiotic groups are different. Bacterial action of aminoglycosides is inhibition of protein biosynthesis, alternatively, penicillin and cephalosporin inhibit bacterial cell wall synthesis. Smith et al found that in patients older than nine years, proptosis, extra ocular movement (EOM) restriction, or elevated IOP at the time of presentation are significantly more likely to require surgical intervention during their hospitalization.Citation21
Complications of orbital cellulitis were varied. Cavernous sinus thrombosis and intracranial extension may result in death. Other complications include corneal exposure with secondary ulcerative keratitis as shown in this case, as well as panopthalmitis. Secondary glaucoma, neurotrophic keratitis, septic uveitis or retinitis, infectious neuritis, inflammatory neuritis, optic nerve edema, exudative retinal detachment and central retinal artery occlusion could also happen.Citation14
This case shows that an acute rapid-onset progressive proptosis may have special attention for diagnosis and management. Orbital cellulitis may mimic rhabdomyosarcoma in baseline clinical presentation. Antibiotic combinations of cephalosporin with aminoglycosides along with corticosteroid, show very good clinical resolution.
Disclosure
The authors report no conflicts of interest in this work.
References
- Jain A, Rubin PA. Orbital cellulitis in children. Int J Ophthalmol Clin. 2001;41(4):71–86. doi:10.1097/00004397-200110000-00009
- Foster JA, Carter KD, Durairaj VD, et al. Section 07: orbit, eyelids and lacrimal system In: Cantor LB, Rapuano CJ, Cioffi GA, editors. 2016–2017 Basic and Clinical Science Course. San fransisco: American Academy of Opthalmology; 2016:70–72.
- Bergin DJ, Wright JE. Orbital cellulitis. Br J Ophthalmol. 1986;70(3):174–178. doi:10.1136/bjo.70.3.1743954974
- Chandler JR, Langenbrunner DJ, Stevens ER. The pathogenesis of orbital complications in acute sinusitis. Laryngoscope. 1970;80(9):1414–1428. doi:10.1288/00005537-197009000-000075470225
- Nageswaran S, Woods CR, Benjamin DK Jr., Givner LB, Shetty AK. Orbital cellulitis in children. Pediatr Infect Dis J. 2006;25(8):695–699. doi:10.1097/01.inf.0000227820.36036.f116874168
- Bajaj MS, Pushker N, Chaturvedi A, et al Orbital space occupying lesion in Indian children. J Pediatr Ophthalmol Strabismus. 2007;44:106–111.17410962
- Boparai MS, Dash RG. Clinical, ultrasonographic and CT evaluation of orbital rhabdomyosarcoma with management. Indian J Ophthalmol. 1991;39:129–131.1841888
- Volpe NJ, Jacobeic FA. Paediatric orbital tumours.. Int Ophthalmol Clin. 1992;32:201–221.1537659
- McDonough RL, Leib ML. Atypical presentation of orbital rhabdomyosarcoma: a report of two cases. J Pediatric Ophthalmol Strabismus. 1995;32:262–265.
- Ganessan K, Bakhshi S. Proptosis in children: approach. Indian J Med Pediatr Onc. 2004;25(Suppl 2):S33–S34.
- Char DH. Tumors of the Eye and Ocular Adnexia. Hamilton: BC. Decker, Inc; 2001.
- Rao AA, Naheedy JH, Chen JYY, Robbins SL, Ramkumar HL. A clinical update and radiologic review of pediatric orbital and ocular tumors. J Oncol. 2013;2013:1–22. doi:10.1155/2013/975908
- Lueder GT, Archer SM, Hered RW, et al. Section 06: pediatric ophthalmology and strabismus In: Cantor LB, Rapuano CJ, Cioffi GA, editors. 2016–2017 Basic and Clinical Science Course. San fransisco: American Academy of Ophthalmology; 2016:313–314.
- Lueder GT, Archer SM, Hered RW, et al. Section 06: pediatric ophthalmology and strabismus In: Cantor LB, Rapuano CJ, Cioffi GA, editors. 2016–2017 Basic and Clinical Science Course. San fransisco: American Academy of Ophthalmology; 2016:306–308.
- Ferguson MP, McNabb AA. Current treatment and outcome in orbital cellulitis. Aust N Z J Ophthalmol. 1999;27(6):375–379.10641894
- Jurdy L, Merks JHM, Pieters BR, et al. Orbital rhabdomyosarcomas: a review. Saudi J Ophthalmol. 2013;27:167–175. doi:10.1016/j.sjopt.2013.06.00424227982
- Pelton RW, Klapper SR. Preseptal and Orbital Cellulitis. Focal Points: Clinical Modules for Ophthalmologists. San fransisco: American Academy of Opthalmoloy; 2008, module 11.
- Garcia GH, Harris GJ. Criteria for nonsurgical management of subperiosteal abscess of the orbit: analysis of outcomes 1988–1998. Ophthalmology. 2000;107(8):1454–1456; discussion 1457–1458.10919887
- Pushkar N, Tejwani LK, Bajaj MS, Khurana S, Velpandian T, Chandra M. Role of oral corticosteroids in orbital cellulitis. Am J Ophthalmol. 2013;156:178–183. doi:10.1016/j.ajo.2013.01.03123622565
- Chang CH, Lai YH, Wang HZ, Su MY, Chang CW, Peng CF. Antibiotic treatment of orbital cellulitis: an analysis of pathogenic bacteria and bacterial susceptibility. J Ocul Pharmacol Ther. 2000;16(1):75–79. doi:10.1089/jop.2000.16.7510673134
- Smith JM, Bratton EM, DeWitt P, Davies BW, Hink EM, Durairaj VD. Predicting the need for surgical intervention in pediatric orbital cellulitis. Am J Ophthalmol. 2014;58(2):387–394. doi:10.1016/j.ajo.2014.04.022