Abstract
Certain clinical aspects of vivax malaria are no longer defined as benign. We present a case of vivax malaria with three relapses in a pregnant Japanese woman who had returned to Japan from the Comoros Islands in East Africa. Data on the successful delivery, examination of Duffy-blood group antigen, and microscopic findings of growing stages of Plasmodium vivax are thought to be of considerable interest.
Keywords:
Introduction
There is growing evidence that the impact of Plasmodium vivax has been underestimated in developing and poor countries.Citation1,Citation2 The difficulty of differential diagnosis and lack of proper treatment of both blood-stage and latent parasites are two of the reasons for the prevalence of vivax malaria.
Case report
A 28-year-old Japanese woman who had been married to an African man and lived in the Comoros Islands for 1 year was admitted to our hospital in Japan because of chills and severe headache. She was 30 weeks pregnant and had taken medication against malaria 2 months previously when she was in Africa.
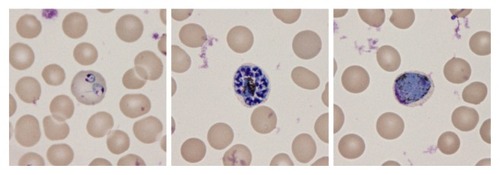
Laboratory findings showed leukocyte (6,600/μL) and platelet (6.6 × 104/μL) counts, as well as hemoglobin (9.7 g/dL), C-reactive protein (CRP; 19.2 mg/dL), fibrin/fibrinogen degradation products (FDP) (35.1 μg/mL), and FDP D-dimer (38.5 μg/mL) levels. Giemsa staining of peripheral blood using pH 7.4 buffer showed that 1.8% of the erythrocytes were infected by Plasmodium. After the ring form, schizont, and gametocyte of this parasite were determined (), the results of the subsequent rapid diagnostic test and DNA assay led to a diagnosis of vivax malaria.
Figure 1 Microscopic findings of the growing stages of Plasmodium species in erythrocytes, which are known to be the merozoite, trophozoite, schizont, and gametocyte stages. Ring forms of two early trophozoites can be observed in an enlarged erythrocyte (left). The presence of more than 16 merozoites in a mature schizont suggests P. vivax infection (center). The presence of a round gametocyte in an enlarged erythrocyte also suggests P. vivax infection (right).
Seven-day medication (quinine 1500 mg/day) against malaria, administered under strict observation and with the patient’s agreement, led to remission. However, vivax malaria relapsed in the 34th week of pregnancy. The presence of latent parasites was suspected to be the cause of the fevers. The next quinine administration resulted in another remission. To exterminate the latent parasites, we assessed mother and child blood glucose-6-phosphate dehydrogenase (G6PD) activities after 39th week spontaneous vaginal delivery, after which she was treated again with primaquine (15 mg/day; 14 days). The new born baby’s weight was 2850 g. There were no abnormalities in either the baby or the placenta. There was no mother-to-child transmission. Mother and child are healthy after 6 months of anti-relapse therapy.
Discussion
Four distinct Plasmodium species are known to regularly infect humans: P. falciparum, P. vivax, P. malariae, and P. ovale. Certain clinical aspects of vivax malaria are not defined as benign anymore because relapse, severe clinical cases, and drug resistance have been reported for P. vivax.Citation1–Citation3 Relapse of P. vivax and P. ovale is known to be triggered by dormant hypnozoites in the liver.Citation2
Plasmodium falciparum malaria is defined as malignant and is a major public health problem in Africa, including the Comoros Islands,Citation4 while vivax malaria is the major cause of malaria outside Africa, mainly afflicting Asia and the Americas.Citation2 Why would vivax malaria be less prevalent in Africa? It is known that Africans with Duffy-blood group antigen negative erythrocytes cannot be infected by P. vivax,Citation5 because it requires the Duffy-blood group antigen as an obligate receptor for invasion,Citation6 and the Duffy-blood group antigen negative phenotype Fy(a− b−) frequently occurs in the native African.Citation7,Citation8
On the other hand, treatment of symptomatic vivax malaria during pregnancy is very difficult. It may lead to preterm delivery and fetal loss, and neonates of non-immune mothers may be at a particular risk of congenital malaria resulting from transplacental passage of parasites.Citation9 Quinine as well as chloroquine are the drugs of choice for the treatment of vivax malaria. Primaquine, the only therapeutic option for these dormant tissue forms, is contraindicated during pregnancy because of the risk of fetal hemolysis.Citation10 Even more noteworthy, low-birth weight associated with vivax malaria has also been reported during second and subsequent pregnancies.Citation11
We reported here repeated recurrences of vivax malaria in a Japanese primigravida from the Comoros Islands. Since the Duffy-blood group antigen of our patient was Fy(a+ b−), our findings support the notion that we should pay careful attention to the occurrence of P. vivax even in Africa,Citation12 in addition to the numerous local Duffy-blood group antigen-negative populations.
Acknowledgments
We thank Dr S Kano, Department of Tropical Medicine and Malaria, Research Institute, National Center for Global Health and Medicine in Japan, for evaluating examinations of using the Binax NOW Malaria Rapid Diagnostic Test (Binax Inc, USA) and RT-PCR using QIAGEN – QIAamp DNA Mini Kit for Plasmodium species. We also thank the Japanese Red Cross Society Saitama Blood Center, for their Duffy-blood group antigen evaluations.
Disclosure
The authors report no conflicts of interest in this work.
References
- PriceRNTjitraEGuerraCAVivax malaria: neglected and not benignAm J Trop Med Hyg200777Suppl 6798718165478
- CarltonJMAdamsJHSilvaJCComparative genomics of the neglected human malaria parasite Plasmodium vivaxNature2008455721475776318843361
- ArgawalRNathAGuptaGNoninvasive ventilation in Plasmodium vivax related ALI/ARDSIntern Med2007462007201118084125
- RebaudetSBogreauHSilaïRGenetic structure of Plasmodium falciparum and elimination of malaria, Comoros archipelagoEmerg Infect Dis201016111686169421029525
- ChaudhuriAPolyakovaJZbrzeznaVCloning of glycoprotein D cDNA, which encodes the major subunit of the Duffy blood group system and the receptor for the Plasmodium vivax malaria parasiteProc Natl Acad Sci U S A1993902210793107978248172
- MichonPFraserTAdamsJHNaturally acquired and vaccine-elicited antibodies block erythrocyte cytoadherence of the Plasmodium vivax Duffy binding proteinInfect Immun200068963164317110816459
- MatsuokaHHasegawaMIshiiAA survey of malaria, glucose- 6-phosphate dehydrogenase deficiency and Duffy blood group in six localities in GuatemalaJ J Trop Med Hyg19881619
- HowesREPatilAPPielFBThe global distribution of the Duffy blood groupNat Commun2011226621468018
- ter KuileFORogersonSJPlasmodium vivax infection during pregnancy: an important problem in need of new solutionsClin Infect Dis2008461382138418419440
- BairdJKNeglect of Plasmodium vivax malariaTrends Parasitol2007231153353917933585
- NostenFMcGreadyRSimpsonJAEffects of Plasmodium vivax malaria in pregnancyLancet1999354917854654910470698
- MizunoYKudoKKanoSDifficulty of proper diagnosis for an imported vivax malaria patient from AfricaKansenshogaku Zasshi2007815597599 Japanese17966644