
Abstract
Pressure injury (PI) corresponds to a skin damage of ischemic aetiology that affects the integrity of the skin and is produced by prolonged pressure or friction between a hard internal and external surface. Treatment can be challenging when there is no resolution with usual care. The use of autologous platelet-rich plasma (APRP) gel arises as a therapeutic possibility in the presence of chronic pressure injuries. The case of a patient with chronic PI who has been treated with APRP is presented, achieving resolution of the lesion.
Introduction
Immobility syndrome is defined as a limitation in the ability to perform activities of daily living due to decreased motor functions; it occurs at any age,Citation1 but the population over 65 years of age are especially susceptible.Citation2 This syndrome increases mortality and morbidity among those who suffer from it. Thus, older adult patients with acute immobility (rapid loss of motor function in less than three days) have a 50% higher probability of dying in the next six month relative to older adult patients without it.Citation3 Similarly, immobility produces physiological alterations in various systems, including the cardiovascular, musculoskeletal and skin system.Citation4 Thus, cardiovascular system undergoes several changes such as the appearance of orthostatic hypotension following the decrease in intravascular volume, or an increased risk of thromboembolic disease due to venous stasis. In the musculoskeletal system, immobility produces a progressive decrease in muscle strength, retractions and ankylosis at joint level.Citation3 Meanwhile, on the skin system, it is common to find pressure injuries (PI), also known as bedsores or decubitus ulcers,Citation4 defined as cutaneous lesions of ischemic aetiology that affect the integrity of the skin and the underlying tissues that are produced by prolonged pressure or friction between an internal and external hard surface.Citation5 A tissue such as skin or muscle requires a capillary pressure of 20 mmHg to allow adequate tissue perfusion; a continuous pressure (longer than two hours) greater than 30 mmHgCitation3 triggers an ischemic process that can end in necrosis.Citation6
It has been found that current prevention techniques may not adequately prevent serious pressure injuries.Citation7 Although the best way to avoid the complications of PI is prevention through skin care, proper moisture management, minimizing pressure and attention to the patient’s needs,Citation7 difficulties in controlling the PI risk factors make pressure ulcers a prevalent problem.Citation8 Therefore, it is necessary to look for complementary alternatives to conventional PI management to avoid the development of deep or chronic injuries. In the management of similar injuries, innovative strategies related to the field of regenerative medicine have been used, such as the use of platelet rich plasma (PRP). There are a diverse number of studies in the use of PRP for the management of ulcers that have evaluated its efficacy and safety in the management of ulcers in the lower limbs,Citation9–Citation14 especially in patients with diabetes.Citation15–Citation18 In these patients, PRP promotes and accelerates the healing of chronic diabetic foot ulcers. Thus, PRP helps healing in patients who have had a skin graft rejection or who have comorbidities that contraindicate anaesthetic or surgical procedures.Citation16 Similarly, a systematic review and meta-analysis of the management chronic diabetic foot ulcers shows scientific evidence of the use of PRP for the treatment of diabetic ulcers. Their authors claim PRP could be the treatment of choice for the topical care of chronic wounds in diabetic patients. In fact, it is proposed that health services that care for patients with chronic wounds should ensure that any patient who requires it can benefit from the use of PRP.Citation19
Based on the biological plausibility of the use of PRP and the favorable evidence of its use in skin lesions, after signing an informed consent, PRP was added to conventional management in a patient who had a chronic ulcer and a high risk to develop a new PI. The treatment was developed in a highly complex hospital in Bogotá that had not yet implemented this management; a recent standardized protocol was used.Citation20
Case Report
A 92-year-old man received hospital care after suffering a left hip fracture. This led to prolonged bed rest of more than a month which led him to develop PI in the left heel. Even though he was treated weekly on an outpatient basis for five months, the PI did not heal. The patient was assessed by the wound clinic of a specialist hospital Bogotá-Colombia for the management of his PI. Norton scale was used to obtain the risk to developing a new PI and the result was 14/20 which corresponded to high risk. The patient had a history of blindness, and he had to use a wheelchair. For this reason, he is limited in his mobility and made him dependent for basic activities. He was considered a candidate for the use of PRP alongside conventional therapy (cleaning, application of zinc oxide, maintenance of dry skin and removal of pressure on the lesion).
Ethics Approval
This intervention complied with the Declaration of Helsinki, including approval by the institution’s Ethics Committee (approval number: FM-CIE-0448-18).
Researchers prepared an informed consent that was approved by the ethics committee of the Pontificia Universidad Javeriana. The patient was blind, we obtained a verbal informed consent from the patient and patient’s legal guardian sign the informed consent, for the case details and accompanying images to be published.
Clinical Findings and Therapeutic Intervention
At the first evaluation, the patient had no coagulation abnormalities, no history of cancer, or the presence of signs of local or systemic infection. Within his paraclinical tests, he presented a hemogram with leukocytes 8,800/mm3, hemoglobin 14.8 g/dL, hematocrit 43.5% platelets 336,000/mm3, creatinine 0.57 mg/dL, albumin 39 g/dL, all within normal values. Upon admission to the study, a NUAPCitation5 classification Phase II pressure ulcer with thick edges measuring 1.8×3.2 cm was observed (). After the evaluation of the PI, the preparation of autologous platelet-rich plasma (APRP) was carried out as follows: 50 mL of whole blood was extracted in tubes with sodium citrate, it was centrifuged at room temperature for 10 minutes at a speed of 1,500 rpm, according to the previously standardized protocol.Citation20 8 cm3 of PRP were obtained, which were placed in a Petri dish and 400 mg of calcium gluconate (50 micrograms for each cubic centimeter obtained from PRP), after 25 minutes it was polymerized and applied to the previously cleaned wound. It was covered with a transparent sterile paraffin dressing (Cuticell ®Classic) and the patient’s family member was instructed to remove it after 72 hours. The wound was evaluated at 7 days (); the same treatment was repeated once a week for a total of four sessions. During treatment researchers observed that after the first week there was a slow decrease in the percentage of closure of the PI, but that after 15 days a closure greater than 50% was achieved and after the third application and evaluation after 24 days, the closing was greater than 90% (). Finally, at the fifth week, the PI was evaluated, showing changes in the diameter of the wound of 0.5×1.2 cm, without signs of infection or discharge (). The wound continued to receive normal healing during the following weeks and after another month of treatment the wound closed completely.
Figure 1 Injury at the beginning of the study day 0.

Figure 2 Visit 8 days after the first application of APRP.

Figure 3 Evolution of the patient’s PI, percentage of closure versus time (days).
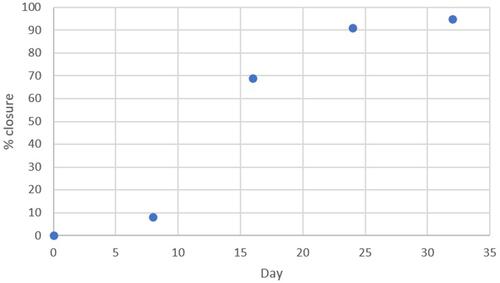
Figure 4 Assessment 32 days after starting the protocol.

Discussion
PI have an increasing prevalence and incidenceCitation21 due to the increase in life expectancyCitation22 and disability in the general population.Citation23 Furthermore, PI tend to be wounds that are difficult to heal, which makes them the focus of infectiousCitation24 or chronic inflammatory processes, a source of morbidity and even mortality in populations that remain immobile for various reasons. This leads to poor quality of life, social isolation, emotional stress and depression in patients who suffer from them,Citation25 as well as significant economic repercussions.Citation26 The prevention of these injuries is the best alternative to avoid these complications and costs.Citation27 However, even with the use of devices with specialized static surfacesCitation28 and rigorous protocols for their prevention, it is not possible to avoid them in 100% of patients who are at risk of suffering them.Citation29,Citation30 Thus, once they arise, it is necessary to use effective alternatives to speed up healing. Debridement, position changes, nutritional optimization, treatment of underlying infections and control of spasms have been postulated as essential in its management.Citation31 However, it is also important to seek complementary, innovative and effective alternatives that reduce healing time, hospital stayCitation32 and associated costs.
The healing of ulcers, especially chronic ones, is dependent on growth factors. The therapeutic administration of growth factors topically, associated with conventional preventive measures, has the potential to accelerate the healing of these wounds.Citation33 Thus, APRP, a treatment that contains fibrin and high concentrations of growth factors, is an option that has shown potential in preliminary studies to help the healing of these wounds.Citation34,Citation35
PRP has been widely used in clinical practice in various tissue disorders. However, there is a little evidenced to suggest the routine use of the PRP in pressure ulcers.Citation36 This fact is consistent with the proposals of some government bodies, such as the Spanish Agency for Medicines and Health Products, which encourage researchers to carry out properly designed clinical trials to establish adequate levels of evidence in each of the pathologies that merit the use of PRPCitation37 or with the conclusions of some systematic reviews regarding the need for randomized clinical trials to evaluate the use of PRP in wound management.Citation38
Currently, there are not a significant number of publications related to the use of PRP in PI or studies in the management of other types of ulcers and in the general management of both acute and chronic wounds. In animals, the efficacy of this intervention in wound healing has been evaluated with favourable results.Citation39–Citation42 Histological techniques have revealed that through the application of PRP products, neovascularization is significantly increased.Citation39–Citation43 Similarly, compared to the controls, PRP significantly improves the formation of granulation tissue, a key element in wound healing.Citation40,Citation42,Citation43 In vitro studies have shown that PRP induces endothelial cell proliferation and capillary formation, as well as increasing fibroblast proliferation compared to the controls in different therapeutic concentrations.Citation40,Citation43,Citation44
Analyses have been carried out on various species. For example, the potential of platelet-derived growth factors to improve surgical wound healing has been evaluated in horses, showing that wounds treated with a PRP gel present rapid epithelial differentiation and greater organization of dermal collagen in comparison with controls.Citation45 Other studies have included stem cells in addition to PRP, this is the case of an investigation where the treatment of severe decubitus ulcers was performed with mesenchymal cells from amniotic fluid and PRP gel in a new born septic foal.Citation46 Plasma rich in growth factors has been evaluated in the healing of skin wounds in albino rabbits, which showed an acceleration in epithelialization and a reduction in skin inflammation at 7 days.Citation47 Similar studies have been carried out in epidermal wounds in rabbit ears with intralesional injection of PRP with convenient results regarding healing.Citation48
In humans, the efficacy and safety of the use of PRP in PI is limited. It is suggested that treatment with growth factors derived from platelets (obtained from PRP) benefit the healing of these lesions and has a potential antibacterial effect. However, the same authors state the need for more studies to support these findings.Citation49 Many of the studies have arisen thanks to the growing trend of applying APRP for the treatment of acute and chronic inflammatory processes,Citation9–Citation11,Citation50 as in the treatment of soft tissue lesions of the musculoskeletal system.Citation51,Citation52 In 1982, a pioneering investigation was published on the use of a fibrin gum, using Platelet Poor Plasma in the repair of a peripheral nerve.Citation53
Since then, especially in the last two decades, these therapies have been used as the main or complementary treatment in different pathologies. APRP is applied topically to the wound or as a local or intra-articular injection. It has been used with appropriate evidence in orthopedics; in the treatment of chronic tendinopathies,Citation54 in dentistry; in post-dental extraction healing and ossification,Citation55,Citation56 in plastic surgery; to improve the healing of lower limb ulcers, ulcers in patients with diabetes and bone grafts.Citation12,Citation38,Citation50,Citation57 Recently, a study using negative pressure wound therapy plus PRP gel found an acceleration in ulcer closure times related to patients with refractory treatment.Citation36 These findings indicate the use of PRP as the treatment of choice for the topical care of chronic wounds. In fact, it is proposed that health services that care for patients with chronic wounds should ensure that any patient who requires it can benefit from the use of PRP.Citation19
The studies cited above motivated the team of the ulcer clinic of a university hospital in Bogotá to implement the use of APRP to close a PI that had not developed satisfactorily with conventional management. The experience of using APRP in this patient was very satisfactory. Even though the PI had received a usual treatment for 5 months never close and after a month of management with APRP, a closure of 95% was obtained. During the intervention and follow-up time, no signs of an allergic reaction or infection were observed. The patient and his caregivers reported having adequately tolerated the handling. Likewise, the members of the Wound Clinic care team stated that the technique of preparation and application of the gel was easy and fast.
Easy application, minimal pain and low cost were evidenced as advantages of using APRP. The preparation and application of the APRP is simple because it consists of few steps and can be learned easily. It is a low-cost technique, once you have the infrastructure that involves a biological safety cabinet and a centrifuge, the rest of the materials such as needles, blood collection system, Petri dish and calcium gluconate, plus the materials used in a regular dressing (gauze, zinc oxide, sterile water or saline solution) are inexpensive. On the other hand, pain is associated with a puncture to obtain plasma but there is no pain when applying the gel. Finally, by accelerating the healing process, patient satisfaction is obtained by achieving the closure of a lesion that affects their quality of life.
APRP is an innovative strategy as an alternative to difficult-to-manage lesions; however, success in this patient may be associated with factors other than APRP, such as the PI phase, the production of growth factors itself, or their nutritional condition. The PI in phase II and III with granulation tissue are in the proliferative phase of healing, in this phase there are numerous growth factors and processes such as angiogenesis and fibroblast migration, which accelerates the process of healing compared to PI in more advanced stages.Citation58 Additionally, biological differences between individuals are a facet that is related to the amount of growth factors and the activation of these factors, which can contribute to the speed of closure of the lesion. Likewise, the patient’s nutrition could be indirectly correlated with their albumin levels. Therefore, since it is a single case, it is difficult to predict whether the improvement of the lesion is only secondary to the use of APRP or the various factors mentioned here.
Conclusions
PI are a problem of increasing prevalence and incidence, a situation that affects the quality of life of patients and incurs excessive costs on the health system. Sometimes these lesions do not respond to conventional management and become chronic. Thus, it is necessary to offer effective and safe alternatives that promote lesion closure. Among these alternatives is the use of APRP, which has shown benefits in tissue regeneration, both in animal models and in humans. However, although it has been used clinically for various types of injuries, the experience of the use of PRP is limited in PI. This report shows a positive experience of the use of PRP in a patient with an PI who had not had a satisfactory evolution with conventional management. Given the efficacy in wound closure and the absence of adverse effects, the use of PRP is considered a promising therapy for the management of chronic PI in the outpatient or hospital setting.
Given that it is the experience of a single patient, studies with a greater number of individuals and different types of PI are required, and allow to evaluate the efficacy and safety of the treatment and, thus, reach enough evidence to consider the use of PRP as part of the usual handling of PI.
Abbreviation
APRP, autologous platelet-rich plasma
Acknowledgments
The authors thank the Universidad Javeriana and the Hospital San Ignacio for the financial support (Investigation project ID: 6223 – Conv. HUSI-PUJ). We also appreciate the financial support to the Universidad de la Sabana (Project ID: MED-247-2018).
Disclosure
Dr Armando Sánchez report grants from Hospital Universitario San Ignacio, during the conduct of the study. Dr Rodrigo Alberto Heredia Ramirez report grants from Hospital Universitario San Ignacio, during the conduct of the study. Dr María José Fernandez Sánchez report grants from Hospital Universitario San Ignacio, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
- Urso ML, Clarkson PM, Price TB. Immobilization effects in young and older adults. Eur J Appl Physiol. 2006;96(5):564–571. doi:10.1007/s00421-005-0109-1
- Fierro A, Solari PS, Pérez A. Síndrome de Inmovilidad. Rev Tendencias Médicas. 2015;2(47):73–76.
- González Madrigal LN. Síndrome de inmovilización en el adulto mayor. Rev Medica Costa Rica Y Centroam. 2015;LXXI(616):551–555.
- Rousseau P. Immobility in the aged. Arch Fam Med. 1993;2(2):169–177. doi:10.1001/archfami.2.2.169
- Black J, Baharestani M, Cuddigan J, et al. National pressure ulcer advisory Panel’s updated pressure ulcer staging system. Dermatol Nurs. 2007;19(4):343–350.
- Salazar CA, Duque OF, Moreno B. Ulceras por presión. In: Gerontología SEdGy, ed. Tratado de Geriatía Para Residentes. Coordinación editorial: International Marketing & Communication, S.A. (IM&C) Vol. 1. 2017:217–226.
- Kayser SA, VanGilder CA, Lachenbruch C. Predictors of superficial and severe hospital-acquired pressure injuries: a cross-sectional study using the international pressure ulcer prevalenceTM survey. Int J Nurs Stud. 2019;89(September2018):46–52. doi:10.1016/j.ijnurstu.2018.09.003
- Delmore B, Ayello EA, Smith D, Rolnitzky L, Chu AS. Refining heel pressure injury risk factors in the hospitalized patient. Adv Ski Wound Care. 2019;32(11):512–519. doi:10.1097/01.ASW.0000579704.28027.d2
- Kim DH, Kim JY, Seo SH, Ahn HH, Kye YC, Choi JE. Recalcitrant cutaneous ulcer of comorbid patient treated with platelet rich plasma: a case report. J Korean Med Sci. 2012;27(12):1604–1606. doi:10.3346/jkms.2012.27.12.1604
- Cervelli V, Gentile P, De Angelis B, et al. Application of enhanced stromal vascular fraction and fat grafting mixed with PRP in post-traumatic lower extremity ulcers. Stem Cell Res. 2011;6(2):103–111. doi:10.1016/j.scr.2010.11.003
- Salemi S, Rinaldi C, Manna F, Guarneri GF, Parodi PC. Reconstruction of lower leg skin ulcer with autologous adipose tissue and platelet-rich plasma. J Plast Reconstr Aesthet Surg. 2008;61(12):1565–1567. doi:10.1016/j.bjps.2008.04.048
- Rozman P, Bolta Z. Use of platelet growth factors in treating wounds and soft-tissue injuries. Acta Dermatovenerol Alp Panonica Adriat. 2007;16(4):156–165.
- Bernuzzi G, Tardito S, Bussolati O, et al. Platelet gel in the treatment of cutaneous ulcers: the experience of the Immunohaematology and Transfusion Centre of Parma. Blood Transfus. 2010;8(4):237–247. doi:10.2450/2009.0118-09
- Ramos-Torrecillas J, De Luna-bertos E, García-Martínez O, Díaz-Rodríguez L, Ruiz C. Use of platelet-rich plasma to treat pressure ulcers: a case study. J Wound Ostomy Continence Nurs. 2013;40(2):198–202. doi:10.1097/WON.0b013e318280018c
- Scimeca CL, Bharara M, Fisher TK, Kimbriel H, Armstrong DG. Novel use of platelet-rich plasma to augment curative diabetic foot surgery. J Diabetes Sci Technol. 2010;4(5):1121–1126.
- Saad Setta H, Elshahat A, Elsherbiny K, Massoud K, Safe I. Platelet-rich plasma versus platelet-poor plasma in the management of chronic diabetic foot ulcers: a comparative study. Int Wound J. 2011;8(3):307–312. doi:10.1111/j.1742-481X.2011.00797.x
- Shan G-Q, Zhang Y-N, Ma J, et al. Evaluation of the effects of homologous platelet gel on healing lower extremity wounds in patients with diabetes. Int J Low Extrem Wounds. 2013;12(1):22–29. doi:10.1177/1534734613477113
- Tzeng Y-S, Deng S-C, Wang C-H, Tsai J-C, Chen T-M, Burnouf T. Treatment of nonhealing diabetic lower extremity ulcers with skin graft and autologous platelet gel: a case series. Biomed Res Int. 2013;2013:837620. doi:10.1155/2013/837620
- Villela DL, Santos VLCG. Evidence on the use of platelet-rich plasma for diabetic ulcer: a systematic review. Growth Factors. 2010;28(2):111–116. doi:10.3109/08977190903468185
- Gómez LA, Escobar M, Peñuela O. Standardization of a protocol for obtaining platelet rich plasma from blood donors; a tool for tissue regeneration procedures. Clin Lab. 2015;61(8):973–980.
- VanGilder C, Amlung S, Harrison P, Meyer S. Results of the 2008-2009 International Pressure Ulcer Prevalence Survey and a 3-year, acute care, unit-specific analysis. Ostomy Wound Manage. 2009;55(11):39–45.
- Neziraj M, Hellman P, Kumlien C, Andersson M, Axelsson M. Prevalence of risk for pressure ulcers, malnutrition, poor oral health and falls – a register study among older persons receiving municipal health care in southern Sweden. BMC Geriatr. 2021;21(1):1–10. doi:10.1186/s12877-021-02205-x
- Jaul E. Who determines the treatment for pressure ulcers in the elderly? Isr Med Assoc J. 2013;15(9):512–515.
- Eilers R, Veldman-Ariesen MJ, Haenen A, van Benthem BH. Prevalence and determinants associated with healthcare-associated infections in long-term care facilities (HALT) in the Netherlands, May to June 2010. Euro Surveill. 2012;17(34):1–8.
- Jones D. Pressure ulcer prevention in the community setting. Nurs Stand. 2013;28(3):47–55. doi:10.7748/ns2013.09.28.3.47.e7660
- Schuurman J, Schoonhoven L, Defloor T, van Engelshoven I, van Ramshorst B, Buskens E. Economic evaluation of pressure ulcer care: a cost minimization analysis of preventive strategies. Nurs Econ. 2009;27(6):390–400.
- Pham B, Teague L, Mahoney J, et al. Early prevention of pressure ulcers among elderly patients admitted through emergency departments: a cost-effectiveness analysis. Ann Emerg Med. 2011;58(5):468–78.e3. doi:10.1016/j.annemergmed.2011.04.033
- McInnes E, Jammali-Blasi A, Bell-Syer SE, Dumville JC, Cullum N. Support surfaces for pressure ulcer prevention. Cochrane Database Syst Rev. 2011;4:CD001735. doi:10.1002/14651858.CD001735.pub4
- Chou R. Pressure ulcer risk assessment and prevention. Ann Intern Med. 2013;159(10):718–719. doi:10.7326/0003-4819-159-10-201311190-00017
- van Rijswijk L, Beitz JM. Creating a pressure ulcer prevention algorithm: systematic review and face validation. Ostomy Wound Manage. 2013;59(11):28–40.
- Cushing CA, Phillips LG. Evidence-based medicine: pressure sores. Plast Reconstr Surg. 2013;132(6):1720–1732. doi:10.1097/PRS.0b013e3182a808ba
- Graves N, Birrell F, Whitby M. Effect of pressure ulcers on length of hospital stay. Infect Control Hosp Epidemiol. 2005;26(3):293–297. doi:10.1086/502542
- Cervelli V, De Angelis B, Lucarini L, et al. Tissue regeneration in loss of substance on the lower limbs through use of platelet-rich plasma, stem cells from adipose tissue, and hyaluronic acid. Adv Skin Wound Care. 2010;23(6):262–272. doi:10.1097/01.ASW.0000363551.82058.36
- de Leon JM, Driver VR, Fylling CP, et al. The clinical relevance of treating chronic wounds with an enhanced near-physiological concentration of platelet-rich plasma gel. Adv Skin Wound Care. 2011;24(8):357–368. doi:10.1097/01.ASW.0000403249.85131.6f
- Sell SA, Ericksen JJ, Reis TW, Droste LR, Bhuiyan MBA, Gater DR. A case report on the use of sustained release platelet-rich plasma for the treatment of chronic pressure ulcers. J Spinal Cord Med. 2011;34(1):122–127. doi:10.1179/107902610X12923394765616
- Liu Q, Zhang N, Li Z, He H. Efficacy of autologous platelet-rich plasma gel in the treatment of refractory pressure injuries and its effect on wound healing time and patient quality of life. Clinics. 2021;76:1–7. doi:10.6061/clinics/2021/e2355
- Ministerio de Sanidad-servicios sociales e igualdad de España. Informe de La Agencia Española de Medicamentos y Productos Sanitarios Sobre El Uso de Plasma Rico En Plaquetas. 2013:1–5
- Martinez-Zapata MJ, Martí-Carvajal AJ, Solà I, et al. Autologous platelet-rich plasma for treating chronic wounds. Cochrane Database Syst Rev. 2012;10(10):CD006899. doi:10.1002/14651858.CD006899.pub2
- Lee H-W, Reddy MS, Geurs N, et al. Efficacy of platelet-rich plasma on wound healing in rabbits. J Periodontol. 2008;79(4):691–696. doi:10.1902/jop.2008.070449
- Pietramaggiori G, Kaipainen A, Czeczuga JM, Wagner CT, Orgill DP. Freeze-dried platelet-rich plasma shows beneficial healing properties in chronic wounds. Wound Repair Regen. 2006;14(5):573–580. doi:10.1111/j.1743-6109.2006.00164.x
- Pietramaggiori G, Scherer SS, Mathews JC, et al. Healing modulation induced by freeze-dried platelet-rich plasma and micronized allogenic dermis in a diabetic wound model. Wound Repair Regen. 2007;16(2):218–225. doi:10.1111/j.1524-475X.2008.00362.x
- Pietramaggiori G, Scherer SS, Mathews JC, et al. Quiescent platelets stimulate angiogenesis and diabetic wound repair. J Surg Res. 2010;160(1):169–177. doi:10.1016/j.jss.2008.09.010
- Takikawa M, Nakamura S-I, Nakamura S, et al. Enhancement of vascularization and granulation tissue formation by growth factors in human platelet-rich plasma-containing fragmin/protamine microparticles. J Biomed Mater Res B Appl Biomater. 2011;97(2):373–380. doi:10.1002/jbm.b.31824
- Bir SC, Esaki J, Marui A, et al. Angiogenic properties of sustained release platelet-rich plasma: characterization in-vitro and in the ischemic hind limb of the mouse. J Vasc Surg. 2009;50(4):870–879.e2. doi:10.1016/j.jvs.2009.06.016
- DeRossi R, de O Coelho ACA, de Mello GS, et al. Effects of platelet-rich plasma gel on skin healing in surgical wound in horses. Acta Cir Bras. 2009;24(4):276–281.
- Iacono E, Merlo B, Pirrone A, et al. Effects of mesenchymal stem cells isolated from amniotic fluid and platelet-rich plasma gel on severe decubitus ulcers in a septic neonatal foal. Res Vet Sci. 2012;93(3):1439–1440. doi:10.1016/j.rvsc.2012.04.008
- Molina-Miñano F, López-Jornet P, Camacho-Alonso F, Vicente-Ortega V. The use of plasma rich in growth factors on wound healing in the skin: experimental study in rabbits. Int Wound J. 2009;6(2):145–148. doi:10.1111/j.1742-481X.2009.00592.x
- Dionyssiou D, Demiri E, Foroglou P, et al. The effectiveness of intralesional injection of platelet-rich plasma in accelerating the healing of chronic ulcers: an experimental and clinical study. Int Wound J. 2013;10(4):397–406. doi:10.1111/j.1742-481X.2012.00996.x
- Ramos-Torrecillas J, García-Martínez O, De Luna-bertos E, Ocaña-Peinado FM, Ruiz C. Effectiveness of platelet-rich plasma and hyaluronic acid for the treatment and care of pressure ulcers. Biol Res Nurs. 2014. doi:10.1177/1099800414535840
- Salcido RS. Autologous platelet-rich plasma in chronic wounds. Adv Skin Wound Care. 2013;26(6):248. doi:10.1097/01.ASW.0000430666.20897.c0
- Moraes VY, Lenza M, Tamaoki MJ, Faloppa F, Belloti JC. Platelet-rich therapies for musculoskeletal soft tissue injuries. Cochrane Database Syst Rev. 2014;4(4):CD010071. doi:10.1002/14651858.CD010071.pub3
- Carter MJ, Fylling CP, Parnell LKS. Use of platelet rich plasma gel on wound healing: a systematic review and meta-analysis. Eplasty. 2011;11:e38.
- Matras H. The use of fibrin sealant in oral and maxillofacial surgery. J Oral Maxillofac Surg. 1982;40(10):617–622.
- Mishra A. Platelet-rich plasma. Orthopedics. 2010;33(7):486–487. doi:10.3928/01477447-20100526-13
- Del Fabbro M, Bortolin M, Taschieri S. Is autologous platelet concentrate beneficial for post-extraction socket healing? A systematic review. Int J Oral Maxillofac Surg. 2011;40(9):891–900. doi:10.1016/j.ijom.2011.04.009
- Antonello GDM, Torres Do Couto R, Giongo CC, Corrêa MB, Chagas OL Júnior, Lemes CHJ. Evaluation of the effects of the use of platelet-rich plasma (PRP) on alveolar bone repair following extraction of impacted third molars: prospective study. J Craniomaxillofac Surg. 2013;41(4):e70–5. doi:10.1016/j.jcms.2012.11.003
- Sommeling CE, Heyneman A, Hoeksema H, Verbelen J, Stillaert FB, Monstrey S. The use of platelet-rich plasma in plastic surgery: a systematic review. J Plast Reconstr Aesthet Surg. 2013;66(3):301–311. doi:10.1016/j.bjps.2012.11.009
- Guarín-Corredor C, Quiroga-Santamaría P, Landinez-Parra NS. Proceso de cicatrización de heridas de piel, campos endógenos y su relación con las heridas crónicas. Rev Fac Med. 2013;61(4 SE):441–448.