
Abstract
Background
Bladder paraganglioma (BPG) is one of the rare neuroendocrine neoplasms that develops from neural crest cells. It categorizes into functional and non-functional types based on the catecholamines secretion. Currently, functional BPG is predicted in advance based on signs and symptoms of catecholamine excess, such as hypertension and “micturition attacks”. However, it is often overlooked because of its rareness. Misdiagnosis of a functional tumor may increase the risk of surgical intervention.
Case Presentation
We reported 3 cases of BPG that they were admitted to the hospital due to abdominal pain or gross hematuria. Computed tomography (CT) scans showed space-occupying lesions in the bladders with diameters less than 3cm. There were no typical catecholamine excess symptoms before surgical intervention. Postoperative pathology confirmed BPG after removal of the tumor. We also analyze 69 cases of BPG that has been reported and found that 78.0% cases were functional among the tumors larger than 3cm.
Conclusion
Bladder tumors larger than 3cm in diameter can serve as an additional predictor of functional BPG. Patients who are suspected should undergo magnetic resonance imaging (MRI) scans, 123/131 metaiodobenzylguanidine (MIBG) scan, and have their catecholamine levels tested. Once the diagnosis is confirmed, patients should be started on fluid replacement therapy and adrenergic blockade to abate the disorders associated with catecholamine excess.
Keywords:
Background
Paraganglioma is one of the rare neuroendocrine neoplasms that derives from neural crest cells. BPG is extremely rare. It constitutes less than 6% of all paragangliomas and 0.06% of all primary bladder tumors.Citation1,Citation2 Since Zimmerman reported the first known case of BPG in 1953,Citation3 the number of reported cases has accumulated only about 185.Citation2
BPG can be categorized into functional and non-functional types. 61.3% of BPG cases were reported to be functional.Citation4 Functional tumors often manifest in catecholamine release induced by micturition. Symptoms may include paroxysmal hypertension, palpitation, headache, dizziness, sweating and even syncope.Citation5,Citation6 The non-functional type is usually presented with painless gross hematuria and is indistinguishable from other types of bladder tumors. Because of its rareness, clinicians often do not consider BPG when diagnosing bladder-occupying lesions. This can lead to misdiagnosis and increase the perioperative risks and complications, especially the functional types. There has been reported that BPG without typical signs and symptoms developed malignant hypertension during surgical resection.Citation7–Citation12 Therefore, preoperative identification of BPG is of great importance.
To increase awareness and understanding of BPG, we report on three patients who were diagnosed and treated for BPG in our hospital. In addition, we analyzed all the reported cases in order to identify other factors that might improve the diagnosis of functional BPG before surgery.
Case Presentation
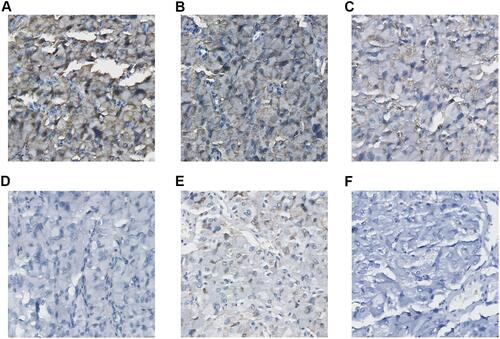
Three patients with BPG in our hospital were between the ages of 45 and 60. They were admitted for abdominal pain or gross hematuria without family history (). CT scans showed space-occupying lesions in the bladders with diameters less than three centimeters (). There were not any typical catecholamine excess symptoms before surgical intervention. Intraoperative blood pressure was stable. Surgical pathology based on the immunohistochemical staining (), which included chromogranin, synaptophysin, Vim, Ki67, S100 and cytokeratin, confirmed the diagnosis of benign BPG.Citation13 Bladder cancer was considered before the operation. Fortunately, it was the benign tumor and the vital signs were stable during the operation. Follow-up cystoscopy performed at three, six, and twelve months showed no recurrence.
Table 1 The Data of the Three Cases
Figure 1 The CT scans of the three cases. (A) Case 1, CT scans of the tumor on the left wall of bladder. (B) Case 2, CT scans of the tumor on the bladder anterior wall. (C) Case 3, CT scans of the tumor on the posterior wall of bladder.

Figure 2 Immunohistochemical staining of the three cases. Immunohistochemistry. Brown staining indicates the positive result (X400). (A) Positive for synaptophysin. (B) Positive for chromogranin. (C) Positive for Vim. (D) Negative for Ki67. (E) The sustentacular cells are stained positive for S100 protein. (F) Negative for cytokeratin.
Discussion and Conclusions
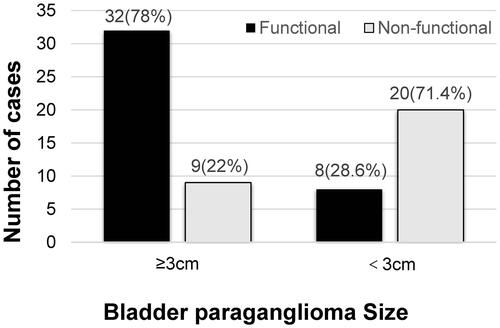
BPG is a rare tumor that currently has no single specific predictor for the preoperative diagnosis, which is easily misdiagnosed as bladder carcinomas. Preoperative misdiagnosis would pose a potential risk for the treatment. We reviewed the case reports of BPG published from 2010 to 2021 in order to find the specific predictor.Citation7–Citation12,Citation14–Citation62 There was a total of 69 cases, including the three cases of ours. Tumors with diameters larger than 3cm were recorded in 41 cases, and less than 3cm in 28 cases. Among the tumors larger than 3cm, 78% were functional, and the smaller than 3cm only 28.6% (). We believe that the functional BPG should be considered when the tumor is larger than 3cm.
Figure 3 The Bladder paraganglioma size. Proportion of functional and non-functional BPG larger than 3 cm or smaller than 3 cm in diameter.
In addition, there have been suggesting that preoperative diagnosis can be inferred from imaging and blood indicators. Wang et al found that an intensely enhanced round or oval-shaped bladder lesion on T1 weighted images are a key MRI feature for paraganglioma.Citation63 On the T2 weighted images, the paraganglioma may exhibit a hyper-intense “salt and pepper” appearance that can differentiate it from other bladder tumors.Citation64 Liang et al reported that bladder masses that display strong hyperintensity on diffusion-weighted MRI images may also be a characteristic of BPG.Citation65 However, MRI cannot distinguish whether the tumor is functional. 123/131MIBG scan, an isotope-imaging technique, has been applied to detect the catecholamine-secreting tumor. The sensitivity for the paraganglioma is 77~99% and the specificity is 95~100%. But the sensitivity decreases in cases of extra adrenal paragangliomas, metastatic paragangliomas, and recurrences.Citation66
Paraganglioma is a neuroendocrine neoplasm that secretes catecholamines. Functional BPG may present with elevated levels of catecholamines, especially during micturition. This phenomenon is referred to as “micturition attacks”Citation67,Citation68 and is usually manifested by headache, palpitations, and syncope. However, 10% of functional tumors may exhibit only minimal or nonspecific symptoms,Citation69 which is so dangerous. Seven cases of above did not present typical clinical symptoms, but the blood pressure both rose higher than 200mmHg during operation.
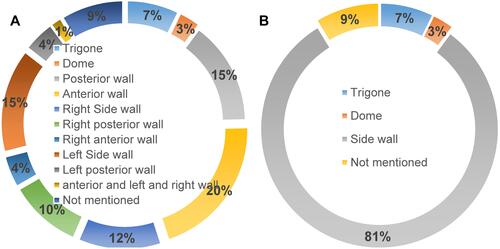
Priyadarshi et al reported that the BPG is most commonly situated at the dome or the trigone of the bladder. Nevertheless, our study found that it is mostly located in the sidewalls (). Musa Male et al compared the characteristics of BPG and urothelial carcinomas using cystoscopy, and found that NPB is more likely to manifest as vascular proliferation, but less likely to have bleeding, necrosis, calcification, pedicles, and multiple lesions.
Figure 4 The distribution of the BPG. (A) Distribution proportion of different parts. (B) Side wall proportion.
Surgical resection remains the mainstay treatment for BPG. Some reports suggest that partial cystectomy is the better treatment option.Citation70 Others recommended transurethral resection of bladder tumor (TURBT).Citation71 We suggest the tumor less than 3cm can be removed through TURBT, depending on the pathology to decide whether further surgical treatment is required. For those larger than 3cm or invaded the full bladder wall, partial or radical cystectomy should be considered. Regardless of the surgical method, preoperative adrenergic blockade to stabilize blood pressure and fluid replacement therapy are recommended for functional tumors.
BPG is a rare bladder tumor that is often missed by clinicians. It can be predicted based on micturition attacks and/or signs and symptoms of catecholamine excess. We suggest that bladder tumors larger than 3cm in diameter can be used as an additional predictor of functional BPG. Patients who are suspected to have functional BPG should undergo MRI scan, 123/131 MIBG scan, and have their catecholamine levels tested. Once a functional tumor is confirmed, patients should be initiated on fluid replacement therapy and adrenergic blockade to abate the disorders associated with catecholamine excess.
Data Sharing Statement
The datasets analysis during the current study are available from the corresponding author on reasonable request.
Consent for Publication
Written informed consent to publish was obtained from all three patients reported.
Disclosure
The authors declare that they have no competing interests.
Additional information
Funding
References
- Katiyar R, Dwivedi S, Trivedi S, Patne SC, Dwivedi US. Non-functional paraganglioma of the urinary bladder treated by transurethral resection: report of two cases. J Clin Diagn Res. 2016;10(2):XD01–XD03.
- Lazareth H, Cohen D, Vasiliu V, et al. Paraganglioma of the bladder in a kidney transplant recipient: a case report. Mol Clin Oncol. 2017;6(4):553–555.
- Zimmerman IJ, Biron RE, Macmahon HE. Pheochromocytoma of the urinary bladder. N Engl J Med. 1953;249(1):25–26. doi:10.1056/NEJM195307022490106
- Beilan JA, Lawton A, Hajdenberg J, Rosser CJ. Pheochromocytoma of the urinary bladder: a systematic review of the contemporary literature. BMC Urol. 2013;13(1471–2490):22. doi:10.1186/1471-2490-13-22
- Deng JH, Li HZ, Zhang YS, Liu GH. Functional paragangliomas of the urinary bladder: a report of 9 cases. Chin J Cancer. 2010;29(8):729–734. doi:10.5732/cjc.009.10703
- Lu H, Male M, Jiang K, Ye Z, Song D, Xia D. Clinical significance of functional and anatomical classifications in paraganglioma of the urinary bladder. Urol Oncol. 2019;37(6):354e359–354 e317. doi:10.1016/j.urolonc.2019.01.027
- Kurose H, Ueda K, Uegaki M, et al. Paraganglioma of the urinary bladder: case report and literature review. IJU Case Rep. 2020;3(5):192–195. doi:10.1002/iju5.12185
- Alkhatatbeh H, Alzaghari D, Alharahsheh S, Ayyad M. Urinary bladder pheochromocytoma managed with TURBT. Case report and review of literature. Urol Case Rep. 2020;33:101291. doi:10.1016/j.eucr.2020.101291
- Sugimura R, Kawahara T, Noguchi G, et al. Functional paraganglioma of the bladder: both radiographic-negative and laboratory-negative case. IJU Case Rep. 2019;2:174–177. doi:10.1002/iju5.12071
- Kido K, Hatakeyama S, Hamano I, et al. Partial cystectomy of paraganglioma of the urinary bladder before living kidney transplantation: case report. Transplant Proc. 2018;50(3):898–901.
- Liang JP, Li HG, Gao LK, Yin L, Yin L, Zhang JW. Bladder paraganglioma: clinicopathology and magnetic resonance imaging study of five patients. Urol J. 2016;13(2):2605–2611.
- Quist EE, Javadzadeh BM, Johannesen E, Johansson SL, Lele SM, Kozel JA. Malignant paraganglioma of the bladder: a case report and review of the literature. Pathol Res Pract. 2015;211(2):183–188.
- Grignon DJ, Ro JY, Mackay B, et al. Paraganglioma of the urinary bladder: immunohistochemical, ultrastructural, and DNA flow cytometric studies. Hum Pathol. 1991;22(11):1162–1169.
- Yin D, Jiao W, Li X, Zhao J. Paraganglioma of the bladder: a case report. Asian J Surg. 2021;11(1):1–4.
- Muhammad S, Yousaf A, Qayyum A, Nazim R, Taqi M. Paraganglioma of urinary bladder in a pediatric patient. Cureus. 2021;13(3):e13964.
- Wang S, Zhang A, Huang S, et al. Non functioning paraganglioma in the urinary bladder: a case report. Urol J. 2020;17(4):426–428.
- Teragaki M, Yamamoto T, Hosomi K, et al. Miction-induced hypertension disclosed by home blood pressure measurement in a patient with small paraganglioma. Intern Med. 2020;59(6):793–797.
- Sonmez G, Tombul ST, Golbasi A, Demirtas T, Akgun H, Demirtas A. Symptomatic paraganglioma of the urinary bladder: a rare case treated with a combined surgical approach. Urol Case Rep. 2020;33:101290.
- Johnson JT, Cherian KE, Kapoor N, Paul TV. Micturition syncope secondary to urinary bladder paraganglioma. BMJ Case Rep. 2020;13(3):e233556.
- Jayarajah U, Herath KB, Fernando MH, Goonewardena S. Phaeochromocytoma of the urinary bladder presenting with malignant hypertension and hypertensive retinopathy. Asian J Urol. 2020;7(1):70–72.
- Urabe F, Miki J, Kimura T, et al. Combination of en bloc transurethral resection with laparoscopic partial cystectomy for paraganglioma of the bladder. IJU Case Rep. 2019;2(5):283–286.
- Sharma AP, Bora GS, Mavuduru RS, Panwar VK, Mittal BR, Singh SK. Management of bladder pheochromocytoma by transurethral resection. Asian J Urol. 2019;6(3):298–301.
- Hermi A, Ichaoui H, Kacem A, et al. Functional bladder paraganglioma treated by partial cystectomy. Case Rep Urol. 2019;2019:4549790.
- Bosserman AJ, Dai D, Lu Y. Imaging characteristics of a bladder wall paraganglioma. Clin Nucl Med. 2019;44(1):66–67.
- Bialek W, Kawecki P, Dyndor K, Wronecki L, Rudzki S. Intraoperative decision to change the course of management based on an ultrasonographic image of urinary bladder paraganglioma - a case study. J Ultrason. 2019;19(77):165–170.
- Alanee S, Williamson SR, Gupta NS. A rare case of non-functioning bladder paraganglioma treated with robotic assisted partial cystectomy. Urol Case Rep. 2019;26:100950.
- Stigliano A, Lardo P, Cerquetti L, et al. Treatment responses to antiangiogenetic therapy and chemotherapy in nonsecreting paraganglioma (PGL4) of urinary bladder with SDHB mutation: a case report. Medicine (Baltimore). 2018;97(30):e10904.
- Mahjoubi Z, Ben Rhouma S, Bibi M, et al. Atypical calcified paraganglioma of the urinary bladder: a new case report. Urol Case Rep. 2018;20:108–110. doi:10.1016/j.eucr.2018.07.024
- El-Tholoth HS, Al Rasheedi S, Alharbi F, Alshammari W, Alzahrani T, Al Zahrani A. Paraganglioma of urinary bladder managed by laparoscopic partial cystectomy in conjunction with flexible cystoscopy: a case report. J Endourol Case Rep. 2018;4(1):15–17. doi:10.1089/cren.2017.0132
- Chaaya G, Morales J, Castiglioni A, Subhani N, Asmar A. Paraganglioma of the urinary bladder: a rare cause of hypertension and urinary tract infections. Am J Med Sci. 2018;355(2):191–194. doi:10.1016/j.amjms.2017.03.037
- Williams P, Siref L, Feloney M. Pheochromocytoma of the bladder. JAAPA. 2017;30(10):23–25. doi:10.1097/01.JAA.0000522134.68445.50
- Srirangalingam U, Banerjee A, Patki P, et al. Succinate dehydrogenase B (SDHB)-associated bladder paragangliomas. Clin Genitourin Cancer. 2017;15(1):e131–e136. doi:10.1016/j.clgc.2016.06.006
- Yadav S, Banerjee I, Tomar V, Yadav SS. Pelvic paraganglioma: a rare and unusual clinical presentation of paraganglioma. BMJ Case Rep. 2016;2016:bcr2015212851.
- Bishnoi K, Bora GS, Mavuduru RS, Devana SK, Singh SK, Mandal AK. Bladder paraganglioma: safe and feasible management with robot assisted surgery. J Robot Surg. 2016;10(3):275–278. doi:10.1007/s11701-016-0573-0
- Sangwatanaroj S, Khovinthasate D, Pathomyok L, Santingamkun A, Snabboon T, Suwanwalaikorn S. Bladder paraganglioma. Am J Med Sci. 2015;350(1):63. doi:10.1097/MAJ.0000000000000254
- Salvatori R, Dackiw AP, Bishop J, Fishman EK. Bladder pheochromocytoma. Endocrine. 2015;48(1):349–350. doi:10.1007/s12020-014-0248-4
- Loveys FW, Pushpanathan C, Jackman S. Urinary bladder paraganglioma: AIRP best cases in radiologic-pathologic correlation. Radiographics. 2015;35(5):1433–1438. doi:10.1148/rg.2015140303
- Han YJ, Ock SY, Kim EJ, Shin HS, Jung YS, Rim H. Thunderclap-like headache triggered by micturition and angina as an initial manifestation of bladder pheochromocytoma. A case report. Sao Paulo Med J. 2015;133(2):154–159. doi:10.1590/1516-3180.2013.6890002
- Dragovic T, Marinkovic D, Kuzmic-Jankovic S, et al. Unrecognised adrenergic symptoms and the delayed diagnosis of urinary bladder paraganglioma. Vojnosanit Pregl. 2015;72(9):831–836. doi:10.2298/VSP140409060D
- Cai Y, Li HZ, Zhang YS. Successful treatment of coexisting paraganglioma of the retroperitoneum and urinary bladder by intermediate-dose 131I-MIBG therapy: a case report. Medicine (Baltimore). 2015;94(41):e1686. doi:10.1097/MD.0000000000001686
- Bagchi A, Dushaj K, Shrestha A, et al. Urinary bladder paraganglioma presenting as micturition-induced palpitations, dyspnea, and angina. Am J Case Rep. 2015;16:283–286. doi:10.12659/AJCR.891388
- Pichler R, Heidegger I, Klinglmair G, et al. Unrecognized paraganglioma of the urinary bladder as a cause for basilar-type migraine. Urol Int. 2014;92(4):482–487. doi:10.1159/000348829
- Kakoi N, Katayama H, Kawamura S, Ito S, Sato I, Tochigi T. [Paraganglioma of the bladder: two case reports]. Hinyokika Kiyo. 2014;60(11):561–566. Japanese.
- Dhull VS, Karunanithi S, Arora S, Jain TK, Kumar R. Diuretic 68Ga DOTANOC PET/CT in imaging of bladder paraganglioma. Clin Nucl Med. 2014;39(10):915–916. doi:10.1097/RLU.0000000000000389
- Song Y, Liu J, Li H, Zeng Z, Bian X, Wang S. Outcomes of concurrent Caesarean delivery and pheochromocytoma resection in late pregnancy. Intern Med J. 2013;43(5):588–591. doi:10.1111/imj.12118
- Malik AA, Afandi B, Jamil G, Akhter SM. Paraganglioma of urinary bladder. BMJ Case Rep. 2013;2013:bcr2013010063. doi:10.1136/bcr-2013-010063
- Feng N, Li X, Gao HD, Liu ZL, Shi LJ, Liu WZ. Urinary bladder malignant paraganglioma with vertebral metastasis: a case report with literature review. Chin J Cancer. 2013;32(11):624–628. doi:10.5732/cjc.012.10317
- Christodoulidou M, Lucky M, Mansour P, Gammal M. Incidental paraganglioma of the urinary bladder in a 66-year-old woman. BMJ Case Rep. 2013;2013:bcr2013008771. doi:10.1136/bcr-2013-008771
- Beilan J, Lawton A, Hajdenberg J, Rosser CJ. Locally advanced paraganglioma of the urinary bladder: a case report. BMC Res Notes. 2013;6:156. doi:10.1186/1756-0500-6-156
- She HL, Chan PH, Cheung SC. Urinary bladder paraganglioma in a post-heart transplant patient. Ann Acad Med Singap. 2012;41(8):362–363.
- Persec Z, Bukovic D, Persec J, et al. Paraganglioma of the urinary bladder–clinicopathological, immunohistochemical and electron microscopy analysis–a case report. Coll Antropol. 2012;36(3):1041–1043.
- Pahwa HS, Kumar A, Srivastava R, Rai A. Unsuspected pheochromocytoma of the urinary bladder: reminder of an important clinical lesson. BMJ Case Rep. 2012;2012:bcr2012006377. doi:10.1136/bcr-2012-006377
- Hanji AM, Rohan VS, Patel JJ, Tankshali RA. Pheochromocytoma of the urinary bladder: a rare cause of severe hypertension. Saudi J Kidney Dis Transpl. 2012;23(4):813–816. doi:10.4103/1319-2442.98167
- Zeitlin I, Dessau H, Lorberboym M, Beigel Y. Malignant pheochromocytoma of the urinary bladder: challenges in diagnosis and management. ISR Med Assoc J. 2011;13(5):311–313.
- Tsai CC, Wu WJ, Chueh KS, et al. Paraganglioma of the urinary bladder first presented by bladder bloody tamponade: two case reports and review of the literatures. Kaohsiung J Med Sci. 2011;27(3):108–113. doi:10.1016/j.kjms.2010.05.005
- Kang SG, Kang SH, Choi H, Ko YH, Park HS, Cheon J. Robot-assisted partial cystectomy of a bladder pheochromocytoma. Urol Int. 2011;87(2):241–244. doi:10.1159/000324269
- De Pasquale V, Magistrelli A, Diomedi Camassei F, Caione P. Unusual bladder mass in a 14-year-old boy: bladder paraganglioma. Urol Int. 2011;86(1):117–120. doi:10.1159/000320840
- Bohn OL, Pardo-Castillo E, Fuertes-Camilo M, Rios-Luna NP, Martinez A, Sanchez-Sosa S. Urinary bladder paraganglioma in childhood: a case report and review of the literature. Pediatr Dev Pathol. 2011;14(4):327–332. doi:10.2350/10-10-0926-CR.1
- Bhalani SM, Casalino DD, Manvar AM. Paraganglioma of the bladder. J Urol. 2011;186(1):279–280. doi:10.1016/j.juro.2011.04.032
- Schaefer IM, Gunawan B, Fuzesi L, Blech M, Frasunek J, Loertzer H. Chromosomal imbalances in urinary bladder paraganglioma. Cancer Genet Cytogenet. 2010;203(2):341–344. doi:10.1016/j.cancergencyto.2010.07.131
- Nayyar R, Singh P, Gupta NP. Robotic management of pheochromocytoma of the vesicoureteric junction. JSLS. 2010;14(2):309–312. doi:10.4293/108680810X12785289145042
- Miwa S, Sugata T. [Asymptomatic pheochromocytoma of the urinary bladder: a case for which preoperative diagnosis was possible]. Hinyokika Kiyo. 2010;56(2):119–121. Japanese
- Wang H, Ye H, Guo A, et al. Bladder paraganglioma in adults: MR appearance in four patients. Eur J Radiol. 2011;80(3):e217–220. doi:10.1016/j.ejrad.2010.09.020
- Athyal RP, Al-Khawari H, Arun N, Abul F, Patrick J. Urinary bladder paraganglioma in a case of von Hippel-Lindau disease. Australas Radiol. 2007;51:B67–B70. doi:10.1111/j.1440-1673.2007.01758.x
- Liang J, Li H, Gao L, Yin L, Yin L, Zhang J. Bladder paraganglioma: clinicopathology and magnetic resonance imaging study of five patients. Urol J. 2016;13(2):2605–2611.
- Taieb D, Neumann H, Rubello D, Al-Nahhas A, Guillet B, Hindie E. Modern nuclear imaging for paragangliomas: beyond SPECT. J Nucl Med. 2012;53(2):264–274. doi:10.2967/jnumed.111.098152
- Kumar S, Choudhary GR, Singh S, et al. Spectrum of retroperitoneal and genitourinary paraganglioma: experience at a North Indian tertiary care center. Cent Eur J Urol. 2015;68(4):421.
- Zhai H, Ma X, Nie W, et al. Paraganglioma of the urinary bladder: a series of 22 cases in a single center. Clin Genitourin Cancer. 2017;15(5):e765–e771. doi:10.1016/j.clgc.2017.03.010
- Messerli FH, Finn M, MacPhee AA. Pheochromocytoma of the urinary bladder. Systemic hemodynamics and circulating catecholamine levels. JAMA. 1982;247(13):1863–1864. doi:10.1001/jama.1982.03320380055031
- Xu DF, Chen M, Liu YS, Gao Y, Cui XG. Non-functional paraganglioma of the urinary bladder: a case report. J Med Case Rep. 2010;4(1752–1947):216. doi:10.1186/1752-1947-4-216
- Baima C, Casetta G, Vella R, Tizzani A. Bladder pheochromocytoma: a 3-year follow-up after transurethral resection (TURB). Urol Int. 2000;65(3):176–178. doi:10.1159/000064868