
Abstract
Percutaneous transvenous mitral commissurotomy is an established treatment for rheumatic mitral stenosis. Dextrocardic heart can be affected by rheumatic pathology just like the normal heart. However, it is technically demanding to percutaneous interventions especially the septal puncture which should be done in a mirror image of the normal. Here we are reporting a 45 year old woman with severe rheumatic mitral stenosis with dextrocardia with situs inversus totalis. She has undergone a successful percutaneous transvenous mitral commissurotomy.
Keywords:
Introduction
Dextrocardia with situs inversus totalis is a rare congenital anomaly characterized by general transposition of viscera due to reverse rotation including heart that rotates to the right side.Citation1 The reported incidence is around 1 in 12000 pregnancies.Citation2 This anomaly has been reported in our country, Ethiopia.Citation3 It may be associated with other congenital heart disease.Citation2 It can be affected by acquired heart disease just like the normal heart. The reported prevalence of rheumatic heart disease in Ethiopia is 19 per 1000 school aged children, which is one of the highest in the world.Citation4 The first line treatment for a favorable isolated rheumatic mitral stenosis is percutaneous transvenous mitral commissurotomy (PTMC) which has excellent short term and long term outcomes if it is done in experienced centers.Citation5 We are reporting one of the first case in our region in a 45 year old female patient with dextrocardia with situs inversus totalis and severe rheumatic mitral stenosis who underwent successful PTMC.
Case Summary
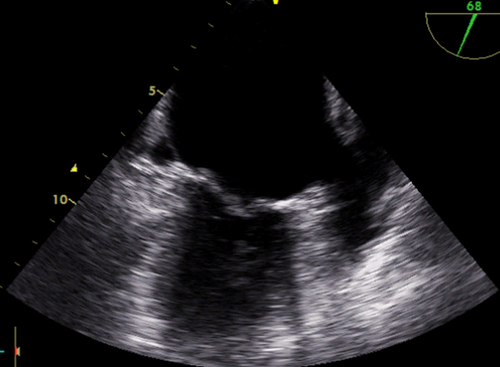
A 45 year old woman presented with progressive shortness of breath and intermittent palpitation for 5 years. She had visited several internists for 3 years before presenting to cardiac center. She had six successful pregnancies, the last one being 11 years back. She had an intermittent dry cough and lower extremity swelling. She was diagnosed with rheumatic heart disease just before her referral to our center. The case was discussed by our heart team including interventional cardiologists and cardiac surgeons before the procedure and the hospital officials before the procedure. On pre-procedure physical examination, she had an irregularly low volume pulse with grade III murmur of mitral stenosis and aortic regurgitation with all heart sounds heard on the right side. Her electrocardiogram shows right axis deviation, absent R-wave progression in the chest leads and course atrial fibrillation (). Postero-anterior chest x ray showed cardiac apex pointing to the right, right-sided aortic arc and lower level right hemidiaphragm presents compared to the left (). Transthoracic and trans-esophageal echocardiography showed mirror image dextrocardia and morphologic changes of rheumatic heart disease involving the mitral and aortic valves, severe mitral stenosis with mitral valve area of 0.7 cm2 and transmitral mean gradient of 13 mmHg, Mild Mitral Regurgitation, Mild Aortic Regurgitation and Moderate Pulmonary hypertension with no left atrial thrombus (). The calculated Wilkin’s score of our patient was 6/16 which is favorable for valvotomy.
Figure 1 12 Lead electrocardiogram.
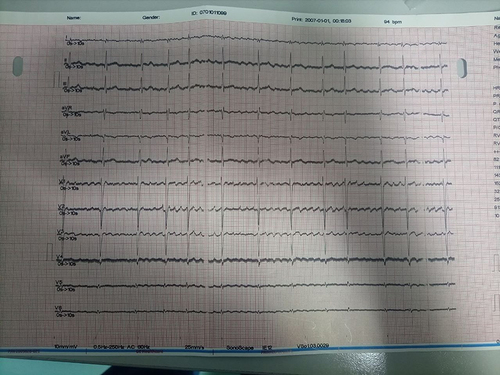
Figure 2 Posteroanterior Chest X ray.
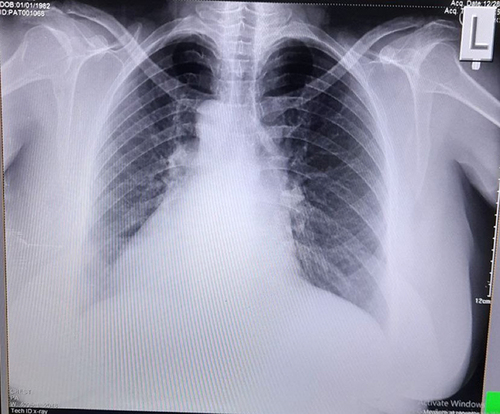
Figure 3 Pre-procedure transesophageal echocardiography.
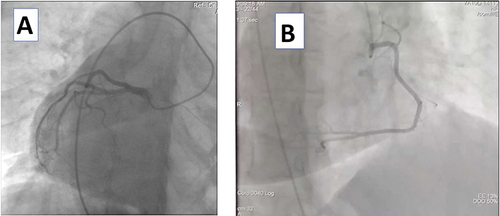
With local anesthesia for both right side femoral arterial access for pigtail catheter at aortic root demarcation to keep the anatomic alignment for the interatrial septum puncture and left femoral vein. Coronary angiography shows normal coronary arteries ( and ).
Figure 4 Coronary angiogram of the left (A) and right (B) coronary arteries.
One of the difficulties in dextrocardia with mitral stenosis is interatrial septal puncture. One of the options to overcome this challenge is to use pseudo normalization (reverse) of the anatomy with the use of application of the newer Cath lab machine. Unfortunately, the software could not do this so we used septal puncture with straight anteroposterior (AP) mode and left ventricle entrance with left anterior oblique (LAO) 30°. We used reverse loop technique which makes the axis better ().
Figure 5 Fluoroscopic image of balloon dilatation of the mitral valve.
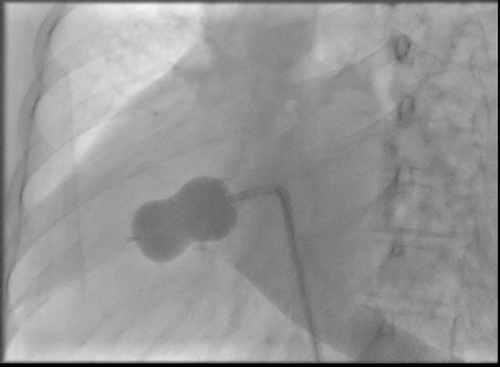
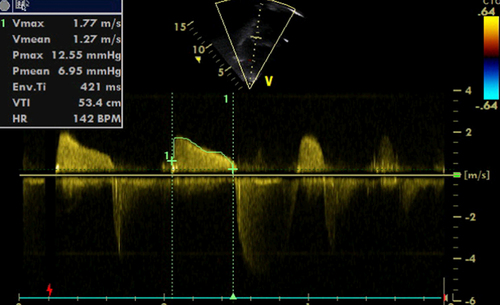
PTMC was done with trans-septal puncture in mirror fashion of normal, which was successful with pre and post procedure variables attached (). The post procedure echocardiogram is attached (). The patient was successfully discharged in the next day with significant improvement of her symptoms. We have seen the patient in 2 weeks and 3 months with significant clinical improvement.
Table 1 Pre and Post Procedure Valve Area and Hemodynamic Parameters
Figure 6 Post-procedure transthoracic echocardiography CW Doppler across the mitral valve.
Discussion
Dextrocardia with Situs Inversus is a rare heart condition characterized by abnormal positioning of the heart and other visceral organs.Citation6 The apex of the heart is positioned on the right side of the chest. Most affected individuals have a normal life expectancy without associated symptoms or disability. Our patient has been asymptomatic for more than 4 decades. Ethiopia is one of the high burden countries for rheumatic heart disease with the prevalence of 19 per 1000 school aged children based on the most recent study. Dextrocardic heart is not immune from rheumatic heart disease.Citation4 Cases of rheumatic heart disease with dextrocardia has been reported from many parts of the world with reported successful surgical and percutaneous interventions.Citation7–9 The anatomical approach of PTMC will be mirror image of the normal heart in patients with mirror image dextrocardia.Citation10 Our patient has normal coronaries on angiography and she had no congenital heart disease other than mirror image dextrocardia. We have summarized the pre and post procedure echocardiography and hemodynamic parameters of our patient. Even though PTMC is an established treatment for rheumatic mitral stenosis most may favor surgical intervention due to the technical difficulties. However, our center decided to do this technically demanding procedure with experienced interventional cardiologist. The procedure was successful with optimal outcome and with no complications. Our take-home message from our case for our readers is that a strong discussion with available heart team and doing such unique cases with the most experienced hands will help patients a lot.
Conclusion
Dextrocardia with situs inversus totalis is rarely seen in clinical practice. Rheumatic heart disease affects these patients just like a normal heart. Understanding the anatomy is very important for optimal outcome of percutaneous or surgical interventions. We have reported the first case of successful valvotomy in a mirror image dextrocrdia in this region.
Consent Statement
The patient gave an informed written consent for publication of her case details, including the history, physical findings, laboratory reports, and images. Our institution has also approved the publication of case details.
Disclosure
The authors report no conflicts of interest in this work.
References
- Saleh A. Dextrocardia with situs inversus totalis in a boy: a case report. Int J Contemp Pediatrics. 2016;1096–1098. doi:10.18203/2349-3291.ijcp20162398
- Bohun CM, Potts JE, Casey BM, Sandor GGS. A population-based study of cardiac malformations and outcomes associated with dextrocardia. Am J Cardiol. 2007;100(2):305–309. doi:10.1016/j.amjcard.2007.02.095
- Tadesse A, Alemu H, Silamsaw M, Gebrewold Y. Kartagener’s syndrome: a case report. J Med Case Rep. 2018;12(1). doi:10.1186/s13256-017-1538-2
- Yadeta D, Hailu A, Haileamlak A, et al. Prevalence of rheumatic heart disease among school children in Ethiopia: a multisite echocardiography-based screening. Int J Cardiol. 2016;221:260–263. doi:10.1016/j.ijcard.2016.06.232
- Abu Rmilah AA, Tahboub MA, Alkurashi AK, et al. Efficacy and safety of percutaneous mitral balloon valvotomy in patients with mitral stenosis: a systematic review and meta-analysis. IJC Heart Vasculature. 2021;2021:33. doi:10.1016/j.ijcha.2021.100765
- Evans WN, Acherman RJ, Collazos JC, et al. Dextrocardia: practical clinical points and comments on terminology. Pediatr Cardiol. 2010;31(1):1–6. doi:10.1007/s00246-009-9516-0
- Bopp P, Bussat P, Lemonnier J, Duchosal PW. Rheumatic heart disease and dextrocardia report of a case from the centre de cardiologie director: prof. Available from: http://archinte.jamanetwork.com/. Accessed July 9, 2024.
- Kulkarni P, Halkati P, Patted S, Ambar S, Yavagal S. Percutaneous mitral balloon valvotomy in a case of situs inversus dextrocardia with severe rheumatic mitral stenosis. Cardiovasc Revascularization Med. 2012;13(4):246–248. doi:10.1016/j.carrev.2012.03.003
- Raju R, Singh S, Kumar P, Kapoor S, Raju BS, Rao S. Case reports percutaneous balloon valvuloplasty in dextrocardia and rheumatic mitral mirror-image stenosis. Catheterization Cardiovasc Diagn. 1993;30(2):138–140. doi:10.1002/ccd.1810300210
- Nallet O, Cormier B, Porte JM, Garbarz E, Michel PL, Vahanian A. Specifics of technique in percutaneous mitral commissurotomy in a case of dextrocardia and situs inversus with mitral stenosis. Catheterization Cardiovasc Diagn. 1996;39(1):85–88. doi:10.1002/(SICI)1097-0304(199609)39:1<85::AID-CCD19>3.0.CO;2-N