
Abstract
Background
Recurrent oral erythema multiforme (ROEM) is an uncommon subtype of erythema multiforme. Immunoglobulin E (IgE) is essential in acute allergy reactions and chronic allergic inflammatory disorders.
Purpose
This report aims to describe the advantages of total IgE screening for detecting mouthwash allergic reactions associated with ROEM.
Case Presentation
A 29-year-old woman came to the Oral Medicine clinic complaining of canker sores all over her mouth and swollen lips accompanied by crusts that had been bleeding easily two months prior. Complaints worsened after the patient used alcohol-containing mouthwash without a history of fever or other symptoms. Extra-oral examination showed upper and lower lip edema with hemorrhagic crusts that bleed easily. No lesions were found in other parts of the body. Intra-oral examination showed ulcers, multiple, irregular in almost the entire oral mucosa. Laboratory examination revealed non-reactive anti-HSV-1 IgG and a total IgE serum level of 612.00 IU/mL. The diagnosis based on the examination results is recurrent oral erythema multiforme.
Case Management
The patient was instructed to stop using alcohol-containing mouthwash, maintain oral hygiene, a healthy lifestyle, adequate hydration, and a balanced diet. Prednisone, benzydamine HCL mouthwash, 0.025% hyaluronic acid mouthwash, multivitamins, and hydrocortisone cream were given as pharmacological therapy. The oral lesions improved in 12 days and the total IgE serum level examination showed a decrease (385 IU/mL).
Conclusion
The total IgE examination can be a screening tool for mouthwash allergy-related reactions to disease and represents the response of ROEM therapy as evidenced by clinical improvement.
Introduction
Erythema multiforme (EM) is a hypersensitivity reaction of the skin and mucosa with marked lesions produced by antigenic stimuli.Citation1,Citation2 A target component or ocular lesion is typical in EM but seems uncommonly present. Oral involvement is reported in 70% of cases, with the vermilion border of the lips, buccal, labial, and lingual mucosa being the most commonly affected areas.Citation3,Citation4 Mucosal lesions are typically erythematous, with shallow erosions and pseudomembranes. Mucosal erosions can be excruciatingly painful, so the medical condition of the patient must be evaluated to preserve oral intake.Citation5
Thirty percent of EM cases may progress to chronic status, characterized by a recurring or persistent course, limiting food intake, necessitating hospitalization, and impairing quality of life.Citation6 Recurrent erythema multiforme and rare persistent erythema multiforme are two entities identified within the clinical spectrum of EM. Patients with recurrent EM experience an average of six episodes per year and a mean disease duration of six to ten years. Recurrent EM is a high morbidity disorder, meaning it often occurs over several years. Recurrent EM is commonly associated with HSV infection, but numerous heterogeneous stimuli such as recurrent M. pneumonia infection, hepatitis C, vulvovaginal candidiasis, menstruation, and high intake of food preservatives have also been reported.Citation7
The human oral mucosa is exposed to many pathogens that can potentially lead to contact allergy. Three types of contact allergy to the oral mucosa are labeled: dental materials, food, and oral hygiene products.Citation8 Hygiene products such as mouthwash can contain many flavorings agents and preservatives capable of causing oral allergic reactions.Citation9 Several brands of mouthwash contain alcohol, which can cause or worsen oral lesions. According to one study, prolonged contact with mouthwash chemicals, including essential oils, antiseptics, and astringents, in addition to low pH on the surface of the oral mucosa, may directly damage the surface epithelium and cause epithelial sloughing.Citation10
Allergy is known as a state of hypersensitivity caused by exposure to specific allergens, and it is characterized by the development of particular antibodies known as Immunoglobulin E (IgE).Citation11 IgE is essential in both acute allergy reactions and chronic allergic inflammatory disorders.Citation12 Men and women, children and adults, and populations with various genetic backgrounds and amounts of exposure to environmental factors all have distinct mean IgE levels.Citation13 Serum tests for total IgE are convenient, economical, and effective when employed as primary screening instruments for atopic status.Citation13,Citation14 Under normal conditions, serum IgE levels are generally low, and increased levels tend to coincide with allergic reactions.Citation15 The purpose of this report is to describe the advantages of total IgE screening for detecting mouthwash allergic reactions associated with recurrent erythema oral multiforme (ROEM).
Case Report
A 29-year-old woman came to the Oral Medicine Clinic at Padjadjaran University Dental Hospital with canker sores throughout her mouth, swollen lips, and hemorrhagic crusts that bleed easily two months prior. The complaint started with a small canker sore on the lateral of the tongue, which the patient attempted to treat with “Natural Green Tea” alcohol-containing mouthwash, but the canker sore was felt to have worsened. The patient admitted to recurrent mouth ulcers but had never experienced such a severe condition before. Previous history of allergy or fever was refused by the patient.
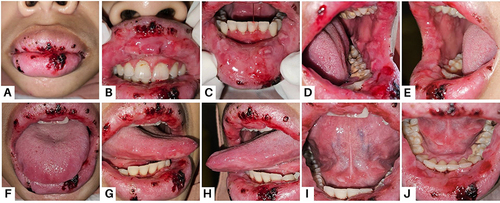
Extra-oral examination revealed upper and lower lip edema with hemorrhagic crusts that bled easily. No lesions were found in other parts of the body. Intra-oral examination showed a macerated appearance on the upper and lower labial mucosa accompanied by multiple ulcers with erythema edges. Several ulcer lesions with irregular margins were also identified on the right and left buccal mucosa, ventral tongue, and floor of the mouth. The gingiva region of teeth 21–24 showed painless erythema with diffuse borders ().
Figure 1 Oedema of the upper and lower lip with hemorrhagic crusts and bleeding easily (A); Multiple irregular ulcer lesions surrounded by erythema areas: Upper labial mucosa (B); Lower labial mucosa (C); Left buccal mucosa (D); Right buccal mucosa (E); Tongue dorsum (F); Right lateral tongue (G); Left lateral tongue (H); Tongue ventral (I); and Floor of the mouth (J).
Based on the history and clinical findings, the suspected diagnosis on the first visit was herpes-associated erythema multiforme, with the differential diagnosis being contact stomatitis and stomatitis medicamentosa. Investigations were carried out to determine the etiology and rule out the possibility of a differential diagnosis. shows the results of a complete blood count, IgE, and anti-HSV-1 IgG titer. Based on the examination, a diagnosis of recurrent oral erythema multiforme was made.
Table 1 Hematology Examination Result
Following the initial visit, the patient was advised to discontinue using alcohol-containing mouthwash. Prednisone was used at a dose of 20 mg per day, divided equally during morning and night. In addition, the patient was instructed to take multivitamins in the morning, rinse her mouth with benzydamine HCl mouthwash before meals, and 0.025% hyaluronic acid mouthwash after meals, 10 mL each three times a day. Furthermore, apply hydrocortisone cream to the lips three times per day. Improvement of lesions in the lips and oral cavity were shown in .
Figure 2 Improvement of the oral lesion on the twelfth day: Lips (A); Upper labial mucosa (B); Lower labial mucosa (C); Left buccal mucosa (D); Right buccal mucosa (E); Tongue dorsum (F); Right lateral tongue (G); Left lateral tongue (H); Tongue ventral (I); and Floor of the mouth (J).
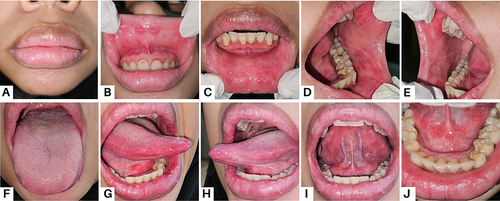
The complaint of swollen lips that bleed easily disappeared on the second visit (twelfth day), but there was a little stinging in her mouth. The patient still felt redness and pain in the upper labial and buccal mucosa. Multivitamins, hydrocortisone cream, and benzydamine HCl mouthwash were discontinued at this visit. The patient was instructed to continue to use 0.025% hyaluronic acid mouthwash, take prednisone at a dose of 15 mg per day, and do scaling. Total serum IgE levels were re-evaluated to screen for allergic conditions and the results are shown in .
Table 2 Total IgE Serum Level Examination
On the third visit, the pain in the mouth was no longer felt and the patient had done scaling. The patient used the medication according to the instructions given. Instructions to continue taking prednisone at a dose of 5mg per day, education to maintain oral hygiene, and a well-balanced lifestyle were given to the patient.
Discussion
Erythema multiforme is an acute immune-mediated disease with mucocutaneous involvement that can be mild (EM minor and EM major), fulminant, or severe (Steven-Johnson syndrome/SJS and toxic epidermal necrolysis/TEN) according to the number of mucosal sites involved and the severity of the lesions.Citation16,Citation17 Intraoral lesions mostly affect the anterior part of the oral cavity and are observed on non-keratinized mucosa. In addition to the palate and alveolar mucosa, the lips are usually always involved, the lips are superficially ulcerated, swollen, and cracked, along with diagnostically distinct blood crusts.Citation7 Based on the history and clinical findings in this article, the suspected diagnosis on the first visit was herpes-associated erythema multiforme, with the differential diagnosis being contact stomatitis and stomatitis medicamentosa.
The term “recurrent erythema oral multiforme” (ROEM) is used when EM lesions are recurrent and confined to the oral mucosa without causing skin lesions. Many investigators have proposed that ROEM is a new subset of EM that has not been widely recognized. Although some recent findings suggest that the diagnosis of ROEM can be made in the absence of positive laboratory data or even when laboratory results of HSV infection are negative, using laboratory techniques to detect HSV infection is sometimes necessary.Citation18 In this case report, an anti-HSV-1 IgG serology test was performed and showed negative results.
The majority of patients with ROEM would present with a chief complaint and a history of recurring ulcerations, which could indicate recurrent aphthous ulcers. ROEM lesions, however, are typically irregular, in contrast to recurrent aphthous ulcer lesions, which are consistently round or oval.Citation18 Based on the clinical examination results showing multiple ulcer lesions with irregular shapes and a history of recurrent complaints, the diagnosis of ROEM was made in the present case report. The diagnosis of ROEM typically can be made based on history and clinical findings. Skin biopsy is indeed performed in only 10% of reported cases of pediatric EM.Citation18,Citation19
Allergy is described as a hypersensitive state caused by exposure to specific allergens. Allergens may get into the body through the skin, oral mucosa, eyes, lungs (inhaled), digestive tract (swallowed), or injection.Citation20 Human oral mucosa is a target for numerous microorganisms and can induce contact allergies. Three types of contact allergies are caused in the oral mucosa, namely dental materials, food, and oral hygiene products. Food and oral hygiene products are involved factors because they contain flavoring agents and preservatives.Citation8 Allergies can cause a wide range of clinical signs and symptoms of oral and perioral disease, including perioral dermatitis, lichenoid reactions, stomatitis, cheilitis, gingivitis, burning sensation, and swelling of the lips and face.Citation21 These clinical presentation varies, making diagnosis difficult and posing a treatment challenge.Citation9
Mouthwashes are agents that can be used for antiseptic, analgesic, anti-inflammatory, or antifungal effects. Mouthwashes with antiseptic solutions are commonly used to reduce the number of microbial colonies in the oral cavity. There are several reasons given for using alcohol-containing mouthwash, but only in particular circumstances and for short periods.Citation22 The ingredients in toothpaste and mouthwash can differ depending on the country of manufacture. According to a study, alcohol-containing mouthwash has 0.092% eucalyptol, 0.042% menthol, 0.060% methyl salicylate, 0.064% thymol, and 26.9% alcohol.Citation10 Some of these components may induce allergies or irritant contact stomatitis. Detergents, preservatives, antiseptics, and flavors typically cause contact stomatitis.Citation23 A study of xerostomia patients discovered that 10.5% of individuals experienced mucosal sloughing after seven days of using alcohol-containing mouthwash.Citation10
“Natural Green Tea” alcohol-containing mouthwash, as used by the patient in this case report, is a mouthwash with many essential oils and green tea leaf extracts. Otera et al described a case of hypersensitivity pneumonitis caused by inhalation of green tea dust after exposure to epigallocatechin (a major component of tea polyphenols). In 2003, Toshihiro et al investigated 11 workers from a green tea processing company who were diagnosed with asthma due to epigallocatechin gallate. Another study described a young woman who developed oropharyngeal and respiratory symptoms after drinking green tea, which was previously shown not to cause allergic reactions.Citation24
Identification of the causative allergens that cause allergic disease is the primary goal of allergy diagnostic evaluation. “Natural green tea” mouthwash is suspected to be the cause of the patient’s allergic reaction that triggered the occurrence of ROEM. The skin test to confirm the suspicion could not be done because the patient moved out of town due to work. In vitro, diagnosis of IgE-mediated allergic disease is useful in identifying the causative allergen and usually involves different laboratory procedures.Citation25 Total serum IgE levels have been important in assessing patients with suspected allergic diseases for many years. Although there are still shortcomings in the sensitivity reported to date, Chang et al study describes the role of serum total IgE examination as a first-line tool for allergy screening and diagnosis.Citation14
Treatment of EM with mucosal involvement depends largely on its severity. Acute conditions generally resolve on their own, but some patients experience recurrent conditions. Identifying the etiology of EM is critical in developing successful therapeutic modalities because treatment modalities differ for acute and recurrent disease. In acute disease, treatment is rarely necessary because lesions generally regress over several weeks, and supportive therapy focuses on improving symptoms. In recurrent EM, therapy focuses on treating the etiology through systemic antiviral prophylaxis therapy.Citation1 Corticosteroids are commonly used to treat ROEM, but once ROEM is a chronic condition with prolonged treatment, corticosteroids are typically not enough to induce remission. When corticosteroid medication is tapered off or stopped, flares are often observed.Citation26
High-potency topical corticosteroid gel can be used together with antiseptic mouthwashes and oral anesthetic solutions in mild to moderate disease.Citation1 As in this report, 0.025% hyaluronic acid mouthwash was administered as an anti-inflammatory agent and aided the healing process. Benzydamine HCL mouthwash is given with the aim of topical anesthesia to reduce patient complaints of pain and to help increase oral intake. In addition, systemic glucocorticoid therapy can be used with a regimen that is mostly given, namely prednisone 40–60 mg/day, and gradually reduced over 2–4 weeks.Citation1 The patient in this case was given prednisone therapy 20 mg/day considering the severity of the lesion. Multivitamins are given as supportive therapy to improve the general condition of the patient.
IgE is mostly known as anaphylactic immunoglobulin and is studied in allergic diseases such as allergic rhinitis and asthma as well as food allergy where specific IgE allergen complexes play a significant role in physiopathology in both acute and chronic phases of allergic inflammation.Citation27 IgE examination in this case was carried out to screen the possibility of an allergic condition and a high IgE value (612 IU/mL) was obtained. Prolonged exposure to allergens can result in widespread erythema of the gingiva or mucosa, as well as ulceration.Citation20 Evaluation of the total IgE value was carried out after discontinuing the use of mouthwash, which was suspected to be an allergen, and therapy for three weeks. The total IgE value at the second examination showed a decrease (385 IU/mL) although it was still above the normal value.
Both IgE and eosinophils play important roles in allergy, but there is controversy in some literature regarding the relationship between serum IgE and eosinophil count. Gwalabe et al reported that there was no significant association between serum IgE and eosinophil count. A possible explanation for this is that the majority of participants in this study had normal eosinophil counts, whereas serum IgE level was raised in all of the participants.Citation28
Total IgE is one of the cost-effective, efficient, and convenient tests that can be used as a first-line screening tool for atopic status. Higher levels of serum total IgE (>100 IU/mL for adults and >77 IU/mL for children) are defined as positive. However, Tu et al have shown that the use of total serum IgE levels alone does not provide sufficient diagnostic accuracy in detecting allergic diseases in a pediatric population in Taiwan.Citation14 Evaluation of total serum IgE levels in this report aims to assess the patient’s allergic condition by considering the reduction in signs and symptoms of inflammation as well as clinical improvement.
Conclusion
Recurrent oral erythema multiforme is a rare type of EM that is difficult to diagnose because there are no specific diagnostic criteria. The diagnosis of ROEM can be made through subjective examination by investigating the history of the disease and objective examination as recurrent multiple ulcers limited to the oral mucosa without causing skin lesions. Aid examinations can provide information about the etiology of the disease, rule out other possible diagnoses such as contact stomatitis and stomatitis medicamentosa, and reveal the response of the disease to therapy. The total IgE examination can be a screening tool for detecting mouthwash allergic reactions to disease and represents the response of ROEM therapy, as evidenced by clinical improvement.
Consent Statements
The patient has approved and written informed consent for the publication of this case report, including the images. The institution has also approved the publication of this article.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
The authors would like to thank the patient who generously participated in this study and also thank Padjadjaran University; Department of Oral Medicine, Faculty of Dentistry, Padjadjaran University; and the staff of Dental Hospital Padjadjaran University.
Additional information
Funding
References
- Soares A, Sokumbi O. Recent updates in the treatment of erythema multiforme. Med. 2021;57(9):1.
- de Risi-Pugliese T, Sbidian E, Ingen-Housz-Oro S, Le Cleach L. Interventions for erythema multiforme: a systematic review. J Eur Acad Dermatol Venereol. 2019;33(5):842–849. doi:10.1111/jdv.15447
- Gosavi AP, Jogi MG, Chavan RB, Tolat SN, Ramawanshi SM. Drug induced mucosal erythema multiforme. Int J Res Dermatology. 2018;4(4):614. doi:10.18203/issn.2455-4529.IntJResDermatol20184472
- Patel R, Mohan A, Omar N, Pardi M. Drug-induced erythema multiforme major in an elderly female. J Community Hosp Intern Med Perspect. 2022;12(3):71–74. doi:10.55729/2000-9666.1057
- Trayes KP, Love G, Studdiford JS. Erythema multiforme: recognition and management. Am Fam Physician. 2019;100(2):82–88.
- Roux C, Sbidian E, Bouaziz J-D, et al. Evaluation of thalidomide treatment of patients with chronic erythema multiforme: a multicenter retrospective cohort study. JAMA dermatol. 2021;157(12):1472–1476. doi:10.1001/jamadermatol.2021.4083
- Krishnankutty K, Chaudhuri K, Ashok L. Erythema multiforme: a case series and review of literature. Open Access J Trans Med Res. 2018;2(4):124–130.
- Minciullo PL, Paolino G, Vacca M, Gangemi S, Nettis E. Unmet diagnostic needs in contact oral mucosal allergies. Clin Mol Allergy. 2016;14(1):1–8. doi:10.1186/s12948-016-0047-y
- Reinhart JP, Stoopler ET, Crawford GH. Oral Hypersensitivity Reactions. Dermatol Clin. 2020;38(4):467–476. doi:10.1016/j.det.2020.05.007
- Wang D, Woo S. Histopathologic Spectrum of Intraoral Irritant and Contact Hypersensitivity Reactions: a Series of 12 cases. Head Neck Pathol. 2021;15(4):1172–1184. doi:10.1007/s12105-021-01330-8
- Sharma M, Khaitan T, Raman S, Jain R, Kabiraj A. Determination of Serum IgE and eosinophils as a diagnostic indicator in allergic rhinitis. Indian J Otolaryngol Head Neck Surg. 2019;71(s3):1.
- Navinés-Ferrer A, Serrano-Candelas E, Molina-Molina G-J, Martín M. IgE-related chronic diseases and Anti-IgE-based treatments. J Immunol Res. 2016;2016:8163803. doi:10.1155/2016/8163803
- Altrichter S, Fok JS, Jiao Q, et al. Total IgE as a Marker for Chronic Spontaneous Urticaria. Allergy Asthma Immunol Res. 2021;13(2):206–218. doi:10.4168/aair.2021.13.2.206
- Chang Y-C, Lee T-J, Huang -C-C, Chang P-H, Chen Y-W, C-H F. The role of phadiatop tests and total immunoglobulin E levels in screening aeroallergens: a hospital-based cohort study. J Asthma Allergy. 2021;14:135–140. doi:10.2147/JAA.S292710
- Li H, Wang L, Li X, Chen W, Zhang Y, Chen J. Serum IgE levels are associated with the prognosis of minimal change disease. Front Immunol. 2022;13:1–10.
- Dalipi ZS, Dragidella F, Dragidella DK. Oral manifestations of exudative erythema multiforme in a patient with COVID-19. Case Rep Dent. 2021;2021:1148945. doi:10.1155/2021/1148945
- Miwa Y, Kawamoto N, Hirata K, Matsunami K, Imamura A. Erythema multiforme minor during sublingual immunotherapy. Pediatr Int. 2021;63(3):348–349. doi:10.1111/ped.14424
- Du Y, Wang F, Liu T, et al. Recurrent oral erythema multiforme: a case series report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol. 2020;129(4):e224–9. doi:10.1016/j.oooo.2019.11.013
- Zoghaib S, Kechichian E, Souaid K, Soutou B, Helou J, Tomb R. Triggers, clinical manifestations, and management of pediatric erythema multiforme: a systematic review. J Am Acad Dermatol. 2019;81(3):813–822. doi:10.1016/j.jaad.2019.02.057
- Dayanarayana U, Shastry SP, Shankar C, Kumar NN, Rama Murthy T, Mahesh B. Allergic manifestations in the oral cavity. J Calif Dent Assoc. 2022;50(5):245–255.
- Lugović-Mihić L, Ilić I, Budimir J, Pondeljak N, Mravak Stipetić M. Common allergies and allergens in oral and perioral diseases. Acta Clin Croat. 2020;59(2):318–328. doi:10.20471/acc.2020.59.02.16
- Kumar PS, Raj AJ. Effects of alcohol containing mouthwash on oral tissue: a review. Int J Sci Res. 2017;6(6):1584–1587.
- Cifuentes M, Davari P, Rogers RS. Contact stomatitis. Clin Dermatol. 2017;35(5):435–440. doi:10.1016/j.clindermatol.2017.06.007
- Mourelle R, Pineda F, Ojeda I, et al. Anaphylaxis caused by green tea: a case report. J Investig Allergol Clin Immunol. 2018;28(5):343–344. doi:10.18176/jiaci.0279
- Ansotegui IJ, Melioli G, Canonica GW, et al. IgE allergy diagnostics and other relevant tests in allergy, a World Allergy Organization position paper. World Allergy Organ J. 2020;13(2):100080. doi:10.1016/j.waojou.2019.100080
- Dias de Oliveira NF, Miyamoto D, Maruta CW, Aoki V, Santi CG. Recurrent erythema multiforme: a therapeutic proposal for a chronic disease. J Dermatol. 2021;48(10):1569–1573. doi:10.1111/1346-8138.16046
- Colas L, Magnan A, Brouard S. Immunoglobulin E response in health and disease beyond allergic disorders. Allergy Eur J Allergy Clin Immunol. 2022;77(6):1700–1718. doi:10.1111/all.15230
- Gwalabe S, Adamu A, Kirfi A, Dunga J, Maigari I. Serum immunoglobulin E level and its relationship with eosinophil count among patients with allergic rhinitis in tertiary hospital in Bauchi, northeastern Nigeria: a cross‑sectional study. Niger J Clin. 2024;27(3):389–393. doi:10.4103/njcp.njcp_605_23