
Abstract
Introduction
Abdominal pain is a diagnostic problem that requires immediate care and treatment for surgeons and gynecologists. The causes of abdominal pain in women of childbearing age range from benign and temporary to potentially life threatening. Rare etiologies such as spontaneous ruptured endometrioma are often not included in the radar of diagnosis due to their rarity and non-specific signs and symptoms in the patient. This case report aimed to show a resemblance between the clinical symptoms of acute abdomen in diffuse peritonitis due to hollow viscus perforation and spontaneous ruptured endometrioma.
Case Description
A 42-year-old woman presented to our hospital with abdominal pain. She had a history of fever for two weeks. She came from a tropical rural area where typhoid fever is common. She was advised to undergo emergency laparotomy because of the suspicion of diffuse peritonitis due to a hollow viscus perforation due to typhoid infection. Because of acute abdominal pain, a vertical incision was made to explore her abdominal cavity, and chocolate-like fluid and ovarian cysts were found during surgery. The diagnosis was changed to diffuse peritonitis due to spontaneous rupture of the endometrioma bilaterally.
Conclusion
This case suggests that the exact diagnosis and cause of abdominal pain varies. As the current gold standard for endometrioma is laparoscopy, surgeons must prepare a collaborative approach to the cause of the disease.
Plain Language Summary
Abdominal pain is common and often requires prompt medical care. In women, it can have various causes, including rare ones, such as spontaneous ruptured endometrioma, which can be difficult to diagnose owing to its rarity and vague symptoms. We describe the case of a 42-year-old woman with abdominal pain and fever, initially suspected to have diffuse peritonitis due to typhoid infection. However, surgery revealed a ruptured endometrioma, highlighting the challenge of accurately diagnosing such conditions. This case emphasizes the need to consider the diverse diagnoses of abdominal pain and the importance of collaborative approaches among medical professionals to ensure accurate diagnosis and treatment.
Introduction
Acute abdominal pain is a diagnostic problem that requires immediate care and treatment by both surgeons and gynecologists. Investigations such as blood testing and imaging are frequently necessary, and early surgical intervention is occasionally considered essential to avoid prolonged treatment.Citation1 The causes of abdominal pain in women of childbearing age range from benign and temporary to potentially life-threatening, which may be caused by either gynecological or non-gynecological illnesses such as infection, bleeding, infarction of tissue, or obstruction of a hollow viscus.Citation2 Acute appendicitis, cholecystitis, pancreatitis, and diverticulitis are common causes of an acute abdomen. Obstetric and gynecologic factors that might lead to this condition include, but are not limited to, ruptured ectopic pregnancy, pelvic inflammatory disease, and ovarian torsion.Citation1 It is important to consider these cause due to during reproductive age, sometimes symptoms can also lead to a misdiagnosis.Citation3,Citation4
Endometrioma rupture is rare, occurring in <3% of cases. The rupture of an ovarian endometrioma can result in acute peritonitis similar to other etiologies.Citation5 The exact risk factor for this rupture is still limited, with endometriomas being suggested by other findings of endometriosis.Citation6 Preoperative diagnosis of endometrioma rupture is infrequent due to its resemblance to other abdominal problems that are more common.Citation7 The gold standard of diagnosing endometrioma and its rupture is still by laparoscopy. This case report aimed to show a resemblance between the clinical symptoms of acute abdomen in diffuse peritonitis due to hollow viscus perforation and diffuse peritonitis due to spontaneous ruptured endometrioma found during surgery.Citation8
Case Presentation
A 42-year-old P1A0 woman was admitted to our hospital with a two-week history of chronic fever. Her fever was notable for being present mostly during evenings. She reported that she felt better with paracetamol, but her fever did not abate. During her fever, she complained of watery stools for two days, after which she was constipated. The patient did not complain of dysmenorrhea or dyspareunia. She lived in a rural area where tropical infections, such as typhoid and paratyphoid fever, are common. There was no family history of malignancy. Her last pregnancy occurred 21 years ago and she had undergone hormonal contraceptive injections for 20 years. The patient had an irregular menstrual cycle with a duration of 5–7 days. The patient had no relevant medical history. Laboratory workup results () suggested typhoid fever.
Table 1 Laboratory Test Results of the Patient with Abdominal Pain Before and After Surgery
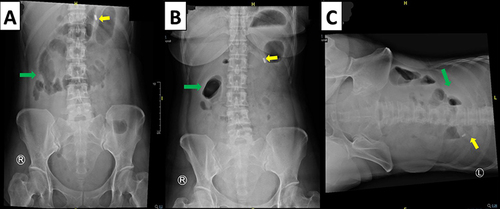
During observation in the ward, the patient suddenly developed severe, acute abdominal pain. The pain was unprovoked and started in the lower abdomen. It soon spread to the entire abdomen, and an acute abdomen was diagnosed. Subsequently, she underwent abdominal radiography (), which showed excessive intestinal air distribution in the right upper abdomen and suspected localized ileus in the right upper abdomen. Diffuse peritonitis due to suspected hollow viscus perforation as a complication of typhoid fever was established, and an emergency laparotomy was performed immediately.
Figure 1 Abdominal X-ray; (A) supine position; (B) half sitting position; (C) left lateral decubitus position. Green arrow showed excessive intestinal air distribution in the right upper abdomen, suspicion of localized ileus at right upper abdomen; yellow arrow showed an NGT position.
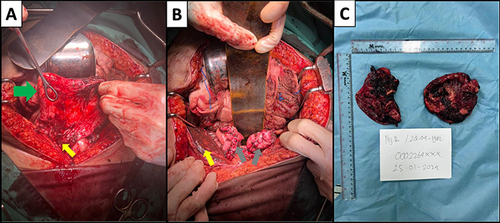
In the theatre, approximately 1000 cc of chocolate-like fluid was discovered after accessing the peritoneal cavity. The fluid was evacuated and ruptured bilateral ovarian cysts were observed ( and ). A gynecological surgeon performed the surgery and found bilateral endometriomas. The right endometrioma measured approximately 10 cm in diameter, whereas the left endometrioma measured approximately 15 cm (). Adhesions with the surrounding organs were observed and successfully lysed. A bilateral cystectomy was performed.
Figure 2 Surgery finding; (A) intra-operative image of ruptured cyst endometriomas, green arrow showed the wall of ruptured cyst, yellow arrow showed fluid-like fluid in intraabdominal; (B) intra-operative image of chocolate cyst after evacuated, grey arrow showed the cyst that had been sutured, yellow arrow showed chocolate-like fluid in intraabdominal; (C) gross specimen of rupture endometriomas.
She was transferred to a high-dependency unit before being transferred to the general gynecology ward. She was hospitalized for four days; fortunately, she recovered uneventfully. The pathological report confirmed the diagnosis of bilateral endometriomas.
Discussion
Acute abdomen is a medical condition that requires immediate care and treatment. The individual typically exhibits an abrupt onset of stomach discomfort accompanied by concurrent symptoms of nausea or vomiting. Globally, it accounts for 10% of all visits to the emergency department.Citation9 Approximately one-third of individuals with abdominal pain experience non-specific abdominal pain, followed by colic renal.Citation9 Other causes which may contribute to this presentation, either due to surgical causes or gyneco-obstetrical causes, are ectopic pregnancy, uterine rupture, ovarian cysts, etc.Citation10 Another gynecological cause is ruptured endometrioma, as in the case presented. The occurrence of an endometrial cyst rupture is infrequent, although not uncommon, retrospective research conducted over seven years, involving 720 women who underwent surgery for endometrioma cysts, found that the incidence of rupture was 2.2%.Citation11 Furthermore, among a substantial collection of cases with acute abdominal pain due to gynecological reasons, 4.6% (70 out of 1509) were identified as resulting from the rupture of an endometrial cyst.Citation12 Endometrioma can be found in up to 44% of woman with endometriosis,Citation8 and only 3% among them suffer the complication with the rupture of endometrioma cysts.Citation5 This condition is usually associated with ovarian adhesion, like the current case.Citation8
Endometriomas, also known as “chocolate cyst” are cystic tumors that arise from endometriosis and are frequently found in the ovaries.Citation13 These tumors are known as chocolate cysts because of their thick dark brown color resulting from fluid with similar characteristics to what we observed in the patient.Citation14 Endometriomas can cause severe abdominal pain followed by peritoneal signs. The exact location of the pain depends on the side of the abnormal growth. In the present case, the mass was found bilaterally in the adnexa. Disease severity may contribute to the patient’s discomfort level. In the event of ovarian endometrioma rupture, viscous endometrial fluid may leak into the abdominal cavity, resulting in substantial pain and inflammation. These individuals frequently exhibit symptoms of sudden and severe surgical conditions affecting the abdomen.Citation13
Traditionally, the patient may previously have dysmenorrhea, dyspareunia, or other endometriosis symptoms.Citation5 Previous history or symptoms of endometriosis could help clinicians to narrow down the cause of the acute abdomen in such a patient but in our patient, she did not experience such, so it is unknown how long she had this condition.Citation5 However the delay of the confirmation is not unusual, Soliman et al found that the interval between the appearance of symptoms and the identification of the condition is frequently prolonged, with an average duration of 4.4 years. As a result, patients may arrive at the Emergency ward without a confirmed diagnosis of endometriosis.Citation15 Aside from that, the spontaneous rupture of endometrioma is also not on the radar due to no clues supporting the diagnosis in the patient, such as a history of pelvic or abdominal trauma, or pregnancy, that would lead the clinician to suspect there is something from a gynecologic aspect.Citation5 In this patient we also did not find a prior history of endometriosis which could be more likely to experience rupture, as the stretching forces between existing adhesions and an expanding ovarian cyst are heightened.Citation16
Based on a physical examination, endometriomas typically has minimal findings; however, if the patient presents with endometrioma rupture, the patient may present with an acute abdomen upon evaluation, including peritoneal signs such as abdominal rigidity, rebound pain, and involuntary guarding; however, these symptoms are not specific to endometrioma.Citation8,Citation16 Gu et al and Huang et al found that ruptured endometrioma tends to occur in patients with lower BMI; however, the exact correlation is still unknown.Citation17,Citation18
Transvaginal ultrasonography (TVU) could be the first choice of imaging study to differentiate between non-gynecological and gynecological causes, such as ruptured endometrioma. Endometriomas can often be visualized on imaging through TVU with a sensitivity and specificity approaching 90%.Citation8 On ultrasound, an endometrioma will typically appear as a cystic structure with low-level internal echoes, but the final pathology still needs an operating table.Citation7 However, TVU has some flaws due to its high false-negative rate and sometimes is not acceptable to some people and may exacerbate pelvic pain symptoms.Citation19 Other imaging modalities that can be considered are magnetic resonance imaging (MRI). MRI has shown a higher sensitivity than ultrasonography for the detection of pelvic masses. However, owing to the cost of MRI, its benefit does not outweigh the financial burden; thus, ultrasound is more commonly used. Similar to ultrasound, MRI is limited in detecting diffuse pelvic endometriosis and may only be beneficial for identifying endometriomas. Other modalities could be used, such as biomarker examinations like CA125, CA19-9, and D-dimer, which are aroused extraordinarily in ruptured endometriomas; however, these biomarkers alone are insufficient for the diagnosis of the disease.Citation20–22 Therefore, it is important to remember that these diagnostic tools only help to differentiate between causes, and the definitive diagnosis of endometriosis is made through surgical visualization of the lesions.Citation7
The gold standard for the diagnosis of endometriosis is via laparoscopy.Citation7 During a laparoscopy, endometriosis lesions typically appear blue or black. However, they can appear as red, white, or nonpigmented lesions. At this time, the severity of the disease can also be evaluated, If there are significant adhesions, peritoneal defects, or endometriomas present, this indicates a more severe disease.Citation13 Based on the size of the cyst they can rupture, a patient who experiences ruptured endometrioma typically has larger diameter cysts than an unruptured patient, however the exact diameter that is prone to rupture is still unknown.Citation17 Dai et al, found the cut-off before the cyst ruptures is 9.5 cm, with specificity of 98.6% and sensitivity of 28.6%.Citation21 Our patient fulfilled this cutoff, as her cysts were at least 10 cm in diameter. Interestingly, some authors have reported that endometriomas are more common in the left ovary than in the right ovary. This might be due to anatomic asymmetry due to the nearby presence of the sigmoid colon and the left broad ligament, causing decreased peritoneal fluid circulation on the left side.Citation23
Conclusion
Acute abdominal pain may be due to various causes, either gynecological and non-gynecological. Endometrioma cyst rupture is a relatively rare cause of acute abdomen. Accurate preoperative diagnosis may not always be possible owing to similarities with other etiologies of acute abdominal pain. An explorative laparotomy is the mainstay of treatment for unstable cases.
Ethical Approval
The authors’ institution does not require ethical approval for publication of single case report.
Consent for Publication
The patient provided written informed consent for publication of the case report and the accompanying images.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
We would like to acknowledge and express our gratitude to our colleagues in the Obstetrics and Gynecology Department of Hasan Sadikin for their help with the case study.
References
- Patterson JW, Kashyap S, Dominique E. Acute Abdomen [Internet]. St. Luke’s Univ. Hosp. Bethlehem: StatPearls Publishing, Treasure Island (FL); 2023. Available from: http://europepmc.org/abstract/MED/29083722. Accessed June 25, 2024.
- Samuelson RN. Acute Abdominal Pain in Women. Decis Mak Med. 1993;590.
- Di Tucci C, Di Mascio D, Schiavi MC, Perniola G, Muzii L, Benedetti Panici P. Pelvic Inflammatory Disease: possible Catches and Correct Management in Young Women. Case Rep Obstetrics Gynecol. 2018;2018:5831029. doi:10.1155/2018/5831029
- Boujida S, M’hamdi O, Mahfoud H, Baydada A, Kharbach A. Ruptured interstitial ectopic pregnancy: a case report and review of the literature. Ann Med Surg. 2012;79:104076.
- Petruškevičiūtė E, Bužinskienė D. Acute Diffuse Peritonitis Due to Spontaneous Rupture of an Infected Endometrioma: a Case Report. Acta Med Lituanica. 2021;28(2):360–366. doi:10.15388/Amed.2021.28.2.20
- Kavoussi SK, Odenwald KC, As-Sanie S, Lebovic DI. Incidence of ovarian endometrioma among women with peritoneal endometriosis with and without a history of hormonal contraceptive use. Eur J Obstet Gynecol Reprod Biol. 2017;215:220–223. doi:10.1016/j.ejogrb.2017.06.028
- Young H, Bui TL, Cramer SE, O’Connell R, Houshyar R. Ruptured endometrioma in a nonpregnant patient: a case report. J Med Case Rep. 2022;16(1):161. doi:10.1186/s13256-022-03361-3
- Cranney R, Condous G, Reid S. An update on the diagnosis, surgical management, and fertility outcomes for women with endometrioma. Acta Obstet Gynecol Scand. 2017;96(6):633–643. doi:10.1111/aogs.13114
- Cervellin G, Mora R, Ticinesi A, et al. Epidemiology and outcomes of acute abdominal pain in a large urban Emergency Department: retrospective analysis of 5340 cases. Ann Transl Med. 2016;4(19):362. doi:10.21037/atm.2016.09.10
- Boukar YME, Mokake D, Elong FA, et al. Prevalence, Aetiology, and Clinical Profile of Acute Abdomen in Pregnancy in Southwest Cameroon: a 5-Year Retrospective Study. Surg Sci. 2023;14(1):1–9. doi:10.4236/ss.2023.141001
- Evangelinakis N, Grammatikakis I, Salamalekis G, et al. Prevalence of acute hemoperitoneum in patients with endometriotic ovarian cysts: a 7-year retrospective study. Clin Exp Obstet Gynecol. 2009;36(4):254–255.
- Coutureau J, Mandoul C, Verheyden C, Millet I, Taourel P. Acute abdominal pain in women of reproductive age: keys to suggest a complication of endometriosis. Insights Imaging. 2023;14(1):94. doi:10.1186/s13244-023-01433-6
- Hoyle AT, Puckett Y Endometrioma. Treasure Isl StatPearls Publ. 2020; Available from: https://www.ncbi.nlm.nih.gov/books/NBK559230/. Accessed June 25, 2024.
- Arafah M, Rashid S, Akhtar M. Endometriosis: a comprehensive review. Adv Anat Pathol. 2021;28(1):30–43. doi:10.1097/PAP.0000000000000288
- Soliman AM, Fuldeore M, Snabes MC. Factors associated with time to endometriosis diagnosis in the United States. J Women’s Heal. 2017;26(7):788–797. doi:10.1089/jwh.2016.6003
- Kohli B, Sharma A, Minhas S. Ruptured endometrioma: a rare event. Int J Clin Obstet Gynaecol. 2022;6(1):111–112. doi:10.33545/gynae.2022.v6.i1b.1125
- Gu Z, Li X, Dai Y, et al. Clinical features of patients with previous spontaneous rupture of ovarian endometrioma operated electively: a case-control study. Reprod Health. 2023;20(1):156. doi:10.1186/s12978-023-01702-z
- Huang YH, Hsieh CL, Shiau CS, Lo LM, Liou JD, Chang MY. Suitable timing of surgical intervention for ruptured ovarian endometrioma. Taiwan J Obstet Gynecol. 2014;53(2):220–223. doi:10.1016/j.tjog.2014.04.018
- Pascoal E, Wessels JM, Aas‐Eng MK, et al. Strengths and limitations of diagnostic tools for endometriosis and relevance in diagnostic test accuracy research. Ultrasound Obstet Gynecol. 2022;60(3):309–327. doi:10.1002/uog.24892
- Gözüküçük M, Taşkın S, Taşcı T, Sönmezer M, Atabekoğlu C. Relation of high CA125 and CA19-9 levels with recent rupture of endometrioma. Gynecol Surg. 2011;8(4):395–398. doi:10.1007/s10397-011-0673-9
- Dai X, Jin C, Hu Y, et al. High CA-125 and CA19-9 levels in spontaneous ruptured ovarian endometriomas. Clin Chim Acta. 2015;450:362–365. doi:10.1016/j.cca.2015.09.019
- Shuang T, Wang Y, Zhao L, et al. Extremely high serum CA19-9 level along with elevated D-dimer in assisting detection of ruptured ovarian endometriosis. Ann Med. 2022;54(1):1444–1451. doi:10.1080/07853890.2022.2074534
- Gałczyński K, Jóźwik M, Lewkowicz D, Semczuk-Sikora A, Semczuk A. Ovarian endometrioma – a possible finding in adolescent girls and young women: a mini-review. J Ovarian Res. 2019;12(1):104. doi:10.1186/s13048-019-0582-5