
Abstract
We report the case of a patient with anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) who exhibited sudden progression of lung infiltration while maintaining stable kidney function. The 69-year-old man was diagnosed with AAV and renal insufficiency 4 years ago. Pulmonic affectation was detected in the right lower lobe of lung by a computed tomography (CT) scan. After beginning cyclophosphamide pulse therapy and sequential therapy with low-dose prednisone, he underwent a 4-year follow-up to detect changes in hemoglobin levels and serum creatinine levels, and had chest CT examinations. The CT scan and creatinine assay showed stable pulmonic fibrosis and kidney function. Although there was no increase of creatinine and detectable perinuclear ANCA, the patient suffered a pulmonary hemorrhage and levels of hemoglobin became progressive lower; the lung infiltration was found to be enlarged compared to the last examination the previous year. After immunosuppressive therapy for one week, the lung fibrosis was progressive, increased pulmonary hemorrhage occurred, and the patient died due to respiratory failure but not end-stage renal failure.
Introduction
The anti-neutrophil cytoplasmic autoantibodies (ANCA)-associated vasculitides (AAVs) comprise a group of diseases characterized by necrotizing vasculitis of small vessels, frequently with involvement of the kidneys and lung.Citation1 Genetic and environmental factors are involved in their etiopathogenesis, with a possible role for silica exposure in AAVs and Staphylococcus aureus infection in granulomatosis with polyangiitis.Citation2 In the clinic, alveolar hemorrhage (AH) is a major cause of early death in AAV; severe AH is strongly correlated with renal vasculitis. AAV patients with renal involvement who need renal replacement therapy have the worst survival prognosis.Citation3,Citation4 We report a case of AAV that remained stable over 4 years and then showed sudden activity as lung infiltration instead of end-stage renal failure (ESRF).
Case report
A 69-year-old male patient presented as an outpatient with increased creatinine levels (281 μmol/L) associated with proteinuria (2.5 g/24 h) and hematuria (110 g/L). His history was not unusual and he denied any abuse of alcohol, drugs, or over-the-counter stimulants. Review of his history was negative for any recent fever, rash, contact with sick persons, or acute illness involving the respiratory or gastrointestinal tract. The examination of ANCA and a chest radiograph were unusual. He was diagnosed with ANCA-associated vasculitis after findings of a perinuclear ANCA (p-ANCA) positive reaction (495 U/mL), urine examination, renal insufficiency by creatinine assay, and lung infiltration by CT scan. After starting treatment with cyclophosphamide pulse therapy, sequential therapy with low-dose prednisone (10 mg qid [every other day]), he underwent a 4-year follow-up. During this time, the level of serum creatinine was stable (), and both proteinuria and hematuria improved (). A chest CT scan was performed, which showed that the lung fibrosis remained unchanged ().
Figure 1 The patient’s serum creatinine (Cr) level over a 4-year period.
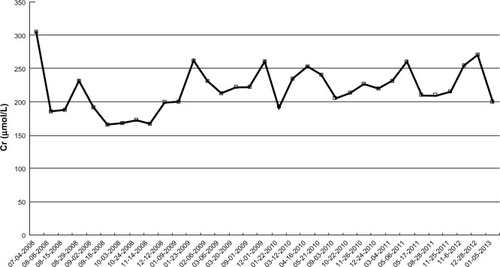
Figure 2 The patient’s hemoglobin level over a 4-year period.
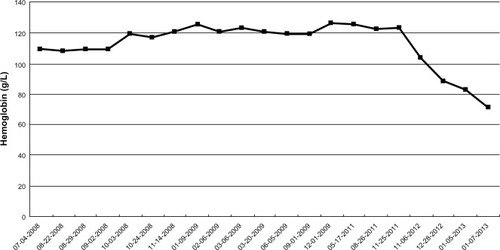
Figure 3 The patient’s chest CTs over a 4-year period. The CT scan shows a progressive pulmonary affectation during the last 2 months.
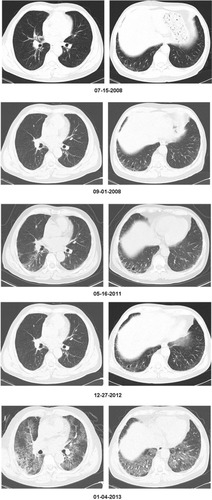
However, after the 4-year follow-up, the patient experienced a sudden and rapid deterioration in lung infiltration and exhibited pulmonary hemorrhage (PH) along with a progressively lower hemoglobin (). Interestingly, there was not only no increase in creatinine levels (), but also a negative conversion of p-ANCA. The galactomannan assay and Mycobacterium tuberculosis antigen-specific interferon (IFN)-gamma release assays (T-SPOT®-TB test; Oxford Immunotec Ltd, Oxford, UK) were both negative. After immunosuppressive therapy (methylprednisolone and cyclophosphamide pulse therapy for 1 week), and empirical widened coverage of anti-infective therapy, progressive lung fibrosis occurred, the PH worsened, and he died from respiratory failure.
Discussion
Vasculitides that cause granulomatous disease are characterized by the presence of ANCA-type antibodies. In most cases, the antibodies are directed against the proteinase 3-antineutrophil cytoplasmic antibody (PR3-ANCA). Such effects may well contribute to a proinflammatory environment in ANCA-associated small-vessel vasculitis and generalized vascular disease.Citation5,Citation6
Renal involvement is frequently present in AAV and is an important cause of ESRF. It has been reported that when patients with AAV progress to ESRF, they are less likely to experience relapse of their vasculitis.Citation7 Furthermore, AAV is both a common cause of diffuse AH and a life-threatening disease.Citation8,Citation9 Although severe PH can occur in ESRD patients with AAV, disease activity and relapses of AAV should be monitored even before the patient’s disease progresses to PH.
In this case, we encountered a patient with AAV suffering from a fatal pulmonary affectation but presenting stable kidney function. Based on the patient’s progressively lower hemoglobin and CT results, AH might be involved in pulmonary affectation. It is suggested that hemorrhage may be a useful biomarker for evaluating the clinical status of AAV.
Induction therapy with oral cyclophosphamide has been a mainstay of treatment in patients with severe renal failure secondary to AAV. The role of plasmapheresis in the treatment of these diseases has also been studied retrospectively.Citation10 Recently obtained insights into the pathogenesis of AAVs have led to a more targeted treatment of these life-threatening diseases. Furthermore, invasive pulmonary aspergillosis has been reported to be a severe opportunistic infection in immunocompromised patients.Citation11,Citation12 Patients with AAV undergoing immunosuppressive treatment are more prone to invasive pulmonary aspergillosis, but only a few cases have been reported in the literature. In this case, the serum galactomannan assay for invasive fungal infections was negative, and empirical antifungal therapy did not reverse his prognosis. Therefore, opportunistic infection was either not found or was not involved in acute exacerbations of the AAV in this patient.
ANCA-associated vasculitis and interstitial lung disease are uncommon conditions. The occurrence of both diseases in the same patient is increasingly recognized. As Arulkumaran et alCitation13 have reported, interstitial lung disease was observed in 2.7% of patients with AAV. It is now recognized that a significant portion of patients with idiopathic pulmonary fibrosis can experience sudden and rapid deterioration in disease course that cannot be explained by infection, heart failure, or thromboembolic disease.Citation14,Citation15 These events are often fatal and have been termed acute exacerbations of underlying disease. Whereas they are most often described in patients with idiopathic pulmonary fibrosis, they have also been reported to be seen in patients with other forms of interstitial lung disease.Citation16 Further investigation into similarities and common pathways in acute exacerbations of various fibrotic lung diseases (including pulmonary vasculitides) may yield additional insight into this recently recognized syndrome.
Diagnosis of AAV can be made according to clinical symptoms, laboratory test results, and image data; however, the gold standard remains the histological proof of a necrotizing, pauci-immune small vessel vasculitis. We report the case of a patient with AAV suffering fatal pulmonary affectation but presenting with almost normal kidney function, indicating that the lungs are possibly the only target organs in acute exacerbations of AAV. It is important to consider the progression of lung fibrosis as a possible complication in AAV patients who have an underlying abnormality of the lung. Even though the optimal strategies for AAV remain unclear, in the future, it might be possible to tailor the treatment modalities according to the risk factors. It is therefore necessary to establish an early diagnosis based on the symptoms. And thanks to new treatments, and despite AAVs being potentially serious diseases, their prognosis has considerably improved in recent years.Citation17,Citation18
Acknowledgments
This work was supported by Jiangsu Provincial Special Program of Medical Science (BL2012023) and Project of Department of Public Health of Jiangsu Province (H201208) and Natural Science Foundation of Jiangsu Province University (13KJB320021). We thank Dr S Puneeth Kumar (The First Affiliated Hospital of Soochow University) for reviewing this article.
Disclosure
The authors report no conflict of interest in this study.
References
- LeeRWD’CruzDPPulmonary renal vasculitis syndromesAutoimmun Rev201091065766020472100
- KallenbergCGStegemanCAAbdulahadWHHeeringaPPathogenesis of ANCA-associated vasculitis: new possibilities for interventionAm J Kidney Dis EpubJune272013
- FatmaLBEl AtiZLamiaRAlveolar hemorrhage and kidney disease: characteristics and therapySaudi J Kidney Dis Transpl201324474375023816724
- HruskovaZCasianALKonopasekPLong-term outcome of severe alveolar haemorrhage in ANCA-associated vasculitis: a retrospective cohort studyScand J Rheumatol201342321121423374071
- SandersJSHuitemaMGHanemaaijerRvan GoorHKallenbergCGStegemanCAUrinary matrix metalloproteinases reflect renal damage in anti-neutrophil cytoplasm autoantibody-associated vasculitisAm J Physiol20072936F1927F1934
- HeeringaPHuugenDTervaertJWAnti-neutrophil cytoplasmic autoantibodies and leukocyte-endothelial interactions: a sticky connection?Trends Immunol2005261156156416139567
- SeckSMDussolBBrunetPBurteySClinical features and outcomes of ANCA-associated renal vasculitisSaudi J Kidney Dis Transpl201223230130522382223
- ChenMZhaoMHSevere pulmonary hemorrhage in patients with end-stage renal disease in antineutrophil cytoplasmic autoantibody-associated vasculitisAm J Med Sci2009337641141419359982
- CordireJFCottinVAlveolar hemorrhage in vasculitis: primary and secondarySemin Respir Crit Care Med201132331032121674416
- AydinZGursuMKaradagSRole of plasmapheresis performed in hemodialysis units for the treatment of anti-neutrophilic cytoplasmic antibody-associated systemic vasculitidesTher Apher Dial201115549349821974704
- WeidanzFDayCJHewinsPSavageCOHarperLRecurrences and infections during continuous immunosuppressive therapy after beginning dialysis in ANCA-associated vasculitisAm J Kidney Dis2007501364617591523
- PraprotnikSSneznaS-STomsicMShoenfeldYThe curiously suspicious: infectious disease may ameliorate an ongoing autoimmune destruction in systemic lupus erythematosus patientsJ Autoimmun2008301–2374118158235
- ArulkumaranNPeriselnerisNGaskinGInterstitial lung disease and ANCA-associated vasculitis: a retrospective observational cohort studyRheumatology (Oxford)201150112035204321873269
- JudgeEPFabreAAdamaliHIEganJJAcute exacerbations and pulmonary hypertension in advanced idiopathic pulmonary fibrosisEur Respir J20124019310022135282
- Simon-BlancalVFreynetONunesHAcute exacerbation of idiopathic pulmonary fibrosis: outcome and prognostic factorsRespiration2012831283521860222
- WilcoxBERyuJHKalraSExacerbation of pre-existing interstitial lung disease after oxaliplatin therapy: A report of three casesRespir Med2008102227327917945475
- BirckRSchmittWHKaelschIAvan der WoudeFJSerial ANCA determinations for monitoring disease activity in patients with ANCA-associated vasculitis: systematic reviewAm J Kidney Dis2006471152316377381
- SandersJSHuitemaMGKallenbergCGStegemanCAPrediction of relapses in PR3-ANCA-associated vasculitis by assessing responses of ANCA titres to treatmentRheumatology (Oxford)200645672472916399845