
Abstract
Purpose
Diaphragmatic hernias (DHs) are divided into congenital and acquired hernias, most of which are congenital. Among acquired DHs, up to 80% are left-sided, only a few iatrogenic DHs have been reported, and bilateral hernias are extremely rare. For diagnostic reasons, many DHs are overlooked by ultrasonography or X-ray and are only recognized at a later stage when complications occur.
Methods
In 2009, we performed three partial diaphragm replacements in our clinic for repairing DHs using a PERMACOL™ implant.
Results
As all patients had uneventful postoperative courses and the clinical outcomes were very good, we present one special case of a 65-year-old male with a giant iatrogenic bilateral DH with an enterothorax.
Conclusion
We see a good indication for diaphragm replacements by using a PERMACOL™ implant for fixing especially DHs with huge hernial gaps and in cases with fragile tissue.
Introduction
Non-traumatic diaphragmatic hernias (DHs) are mainly of congenital origin, whereas DHs in adults are seen in blunt (0.8%–5% incidence) or penetrating (10%–15% incidence) thoracoabdominal trauma.Citation1–Citation3 Among acquired DHs, up to 80% are left-sided, bilateral hernias are extremely rare, and only a few iatrogenic DHs have been reported.Citation4 Most acquired DHs are caused by sternotomies in adult and pediatric cardiac surgery and abdominal surgery.Citation5–Citation10
The majority of traumatic or iatrogenic DHs manifest immediately or shortly after an accident. Despite there being various diagnostic tools, some hernias can still be overlooked and only recognized at a later stage when complications resulting from the herniated organs have manifested.Citation2,Citation11–Citation14 Nevertheless, some develop long after the injury and only turn symptomatic after an interval of months or years.Citation15,Citation16 The main symptoms of DHs are abdominal/chest pain and dyspnea due to pulmonary compression, bowel obstruction and strangulation, which were present in our case.
Thoracotomy and/or laparotomy are often required in a hemodynamic unstable polytraumatic patient. However, thoracoscopy and/or laparoscopy have recently been suggested in the literature to be helpful for both the diagnosis and treatment of these lesions in order to reduce the high morbidity and mortality rates seen with open procedures.Citation2,Citation13,Citation17–Citation20 Although the closure technique for the hernia site is still a matter of discussion, direct closure without plastic seems to be favored by some authors.Citation13,Citation18
Case report
The reported patient is a 65-year-old male. During a vocal cord operation 10 years before, there was an accidental intralaryngeal gas explosion that required several subsequent tracheal reconstructions. Consequently, a huge bilateral diaphragmatic hernia developed over the years.
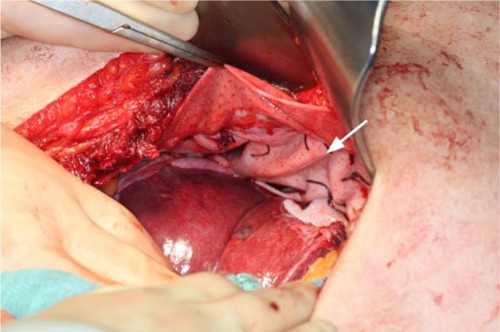
As the patient was suffering from progredient dyspnea, a computed tomography was performed, which showed a complete enterothorax (); therefore, an operative approach was indicated. The upper abdomen was incised by transverse laparotomy revealing a large package of small intestine ventrally disappearing on both sides of the chest (). The adhesions were divided and the parts of the colon and jejunum that were dislocated in the chest were repositioned into the abdomen. Some parts were partially strangulated but still in good shape. The stomach, however, was in the correct anatomical location. After repositioning and resection of the hernial sac, the hernial gap could hardly be adapted (). The diaphragm was very weak, which suggested that a direct closure would be too fragile. For this reason, a large flap of PERMACOL™ (original size: 18 cm ×28 cm ×1.5 cm; Covidien Ltd, Dublin, Ireland) was trimmed to fit so that it covered both sides of the dorsal diaphragm and the ventral part of the flap overlapped with the abdominal wall incision (). The flap was fixed all around with VICRYL™ 0 sutures (Johnson & Johnson, New Brunswick, NJ, USA; ). As a pneumothorax on the right side was provoked by the manipulation, thoracic drainage was applied. The abdominal wall was occluded involving the ventral edge of the PERMACOL™ flap to provide for more stability.
Figure 1 Computed tomography scan of the thorax showing a complete enterothorax (arrows).

Figure 2 A large package of small intestine disappearing on both sides of the chest.
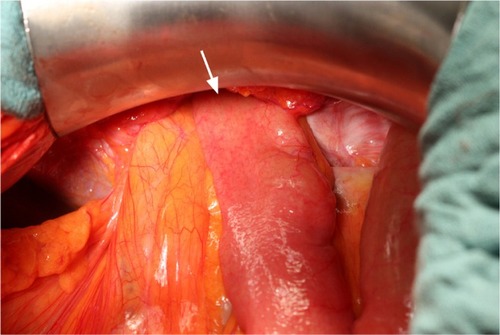
Figure 3 Huge hernial gap in the diaphragm.
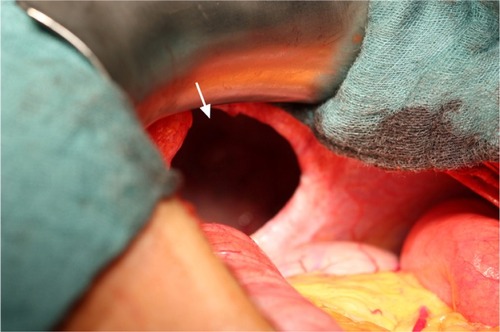
Figure 4 Cutting and fitting of the PERMACOL™ implant.

Figure 5 Final result after fixing the PERMACOL™ implant with VICRYL™ sutures.
The postoperative course was uneventful apart from paroxysmal atrial fibrillation and the patient was released from hospital 16 days after operation.
The postoperative follow-up after 3 and 6 months including a computed tomography scan did not reveal any pathologies.
Discussion
The interesting aspects of this case are the huge bilateral expansion of the DH and the unusual iatrogenic cause preceding the symptoms by 10 years.
The distinct weakness of the entire diaphragm – a hint of the chronic progress of the hernia – required reconstruction by an implant. Usually, synthetic mesh like polytetrafluoroethylene is used to close hernial gaps but also other material is sometimes used. In this case, we decided to use a large porcine dermal collagen flap which serves as a matrix for cell ingrowth and neovascularization, because of its very good biocompatibility. Even though there was a previous report about the rejection of a PERMACOL™ implant used in abdominal wall repair, in our case, we had no postoperative complications or any hernia relapse.Citation21
Conclusion
Based on our experience, PERMACOL™ implants are a good choice for diaphragm replacements especially for fixing DHs with huge hernial gaps and in cases with fragile tissue.
Finally, prospective and randomized trials have to be performed to resolve the pros and cons of this procedure.
Disclosure
The authors report no conflicts of interest in this work.
References
- GhanemANChankunTSBrooksPLTotal gastric gangrene complicating adult Bochdalek herniaBr J Surg19877497793664240
- NauTSeitzHMousaviMVecseiVThe diagnostic dilemma of traumatic rupture of the diaphragmSurg Endosc200115999299611443468
- RossettiGBruscianoLMaffettoneVGiant right post-traumatic diaphragmatic hernia: laparoscopic repair without a meshChir Ital200557224324615916154
- SirbuHBuschTSpillnerJSchachtruppAAutschbachRLate bilateral diaphragmatic rupture: challenging diagnostic and surgical repairHernia200591909215351874
- AshourKJamiesonKLakhooKA sternotomy too farInteract Cardiovasc Thorac Surg20099475375419620173
- BettolliMJacksonCCSweeneyBRubinSIatrogenic anterior diaphragmatic hernia in childhoodEur J Pediatr Surg200818427527618629775
- ChinRYGlewMJBradyPIatrogenic intrapericardial diaphragmatic herniaANZ J Surg200272968168312269926
- DraftsBCChughtaiHLEntrikinDWIatrogenic intrapericardial diaphragmatic hernia diagnosed by cardiovascular magnetic resonanceJ Cardiovasc Magn Reson201012320064206
- DukhnoOPeiserJLevyIOvnatAIatrogenic diaphragmatic hernia due to laparoscopic gastric bandingSurg Obes Relat Dis200621616316925323
- MuysomsFECathenisKKHamerlijnckRPClaeysDALaparoscopic repair of iatrogenic diaphragmatic hernias after sternectomy and pedicled omentoplastyHernia200913661762319710999
- CristofaroMGLazzaroFCafaroDPost-traumatic diaphragmatic hernia with late diagnosis. Report of a clinical caseAnn Ital Chir2000715595598 Italian11217477
- MontresorEProcacciCGuariseAStrangulated traumatic hernia of the diaphragm. A report of two casesChir Ital199951647147610742899
- RufGMappesHJKohlbergerEBaumgartnerUFarthmannEHDiagnosis and therapy of diaphragmatic rupture after blunt thoracic and abdominal traumaZentralbl Chir199612112429 German8852737
- ScaglioneMPintoFGrassiRDiagnostic sensitivity of computerized tomography in closed trauma of the diaphragm. Retrospective study of 35 consecutive casesRadiol Med2000991–24650 Italian10803186
- AlimogluOEryilmazRSahinMOzsoyMSDelayed traumatic diaphragmatic hernias presenting with strangulationHernia20048439339615098101
- CarterBNGiuseffiJFelsonBTraumatic diaphragmatic herniaAm J Roentgenol Radium Ther19516515672
- KoehlerRHSmithRSThoracoscopic repair of missed diaphragmatic injury in penetrating trauma: case reportJ Trauma19943634244278145332
- KurataKKubotaKOosawaHEdaNIshiharaTThoracoscopic repair of traumatic diaphragmatic rupture. A case reportSurg Endosc19961088508518694953
- MeyerGHüttlTPHatzRASchildbergFWLaparoscopic repair of traumatic diaphragmatic herniasSurg Endosc200014111010101411116407
- WadhwaASurendraJBSharmaALaparoscopic repair of diaphragmatic hernias: experience of six casesAsian J Surg200528214515015851372
- WottonFTAkohJARejection of Permacol mesh used in abdominal wall repair: a case reportWorld J Gastroenterol200915344331433319750579