
Abstract
Kikuchi disease, also called Kikuchi–Fujimoto disease or Kikuchi’s histiocytic necrotizing lymphadenitis, is a rare, benign condition of unknown cause, usually characterized by cervical lymphadenopathy and fever. The diagnosis is based on histopathology. Our patient was a woman with bilateral cervical lymphadenopathy, fever, chest and abdominal pain, fatigue, maculopapular rash on her face, trunk, and upper and lower extremities. Immunological and rheumatological tests were negative. We took a cervical lymph node biopsy that showed a proliferative and necrotizing process centered in the paracortex characterized by patchy circumscribed or confluent areas of necrosis associated with karyorrhexis, and was remarkable by the absence of granulocytes and the paucity of plasma cells. These findings confirmed the diagnosis of Kikuchi’s disease. The patient’s hemoglobin values decreased, and the peripheral blood smear revealed schistocytes. Blood tests showed raised D-dimer, activated partial thromboplastin time, prothrombin time, and international normalized ratio with decreased fibrinogen. The patient’s condition quickly worsened and disseminated intravascular coagulopathy eventually developed. Her initial management consisted of a corticosteroid and hydroxychloroquine.
Introduction
Kikuchi–Fujimoto disease (KFD), or histiocytic necrotizing lymphadenitis, was originally described in Japan in 1972 by KikuchiCitation1 and Fujimoto et al.Citation2 In the following years, several series of cases involving patients of different ages, races, and geographic origins were reported. This is a self-limiting process of unknown etiology, but in some reports, an immunologic or infectious event was speculated as being involved in the pathogenesis.Citation3 However, it can rarely be fatal.Citation4 KFD is more frequent among Asians, especially among Japanese individuals. It was thought to be much more common among women, with a female to male ratio of about 4:1, but in recent reports, the actual ratio is suggested to be closer to 1:1.Citation5 Most of the patients are under the age of 30 years old.Citation6 Regional tender lymphadenopathy (mostly cervical) and fever are the two most characteristic features of this disorder.Citation7 Night sweats, weight loss, nausea, vomiting, and sore throat are the other findings that can be observed in this disease.Citation7 Diagnosis is based on excisional biopsy of enlarged lymph nodes. The disease may be mistaken for and treated as lymphoma because it frequently mimics high-grade lymphoma.Citation6 We report a case of disseminated intravascular coagulopathy caused by KFD.
Case report
A 32-year-old woman was admitted to hospital complaining of fever, fatigue, as well as chest and abdominal pain of 15 days’ duration, and with no personal and family history for tuberculosis and malignant diseases. Vital signs in the emergency department revealed a temperature of 39°C, a blood pressure level of 140/80 mmHg, a heart rate of 88 bpm, and a respiratory rate of 16 breaths/minute. On physical examination, she was lethargic and maculopapular rashes were patent on her face, trunk, and upper and lower extremities. She had bilateral enlarged cervical, axillary, and inguinal lymph nodes, which were freely mobile, painless on palpation, discrete and sized in the range of 0.5–3.7 cm. In , computed tomography of the neck showed the presence of lymphadenomegalies of various sizes. Cardiovascular and respiratory examinations were unremarkable. Initial laboratory studies revealed hemoglobin levels of 10.2 g/dL, leukocytes of 17,800/mm³ with an abnormal differential count of eosinophils of 9.8%, neutrophils of 54.3%, monocytes of 14%, platelets of 205,000/mm³, lactate dehydrogenase of 578 U/L, C-reactive protein of 28.2 mg/L, and an erythrocyte sedimentation rate (ESR) of 77 mm/hour. Liver and renal tests were normal. Serologic tests for toxoplasma, Epstein–Barr virus, rubella, cytomegalovirus, herpes simplex type 1, hepatitis B, and hepatitis C were all negative. Blood, urine, and sputum cultures were negative. Sputum culture was also negative for acid-fast bacilli. Protein electrophoresis showed polyclonal gammopathy. Also, immunological and rheumatological tests, including antinuclear antibody, deoxyribonucleic acid antibody, perinuclear anti-neutrophil cytoplasmic antibodies, antineutrophil cytoplasmic antibodies, extractable nuclear antigens, and rheumatoid factor were all negative. Electrocardiogram and chest radiographs were normal.
Figure 1 Computed tomography of neck; lymphadenomegalies in various dimensions.

Computed tomography demonstrated generalized lymphadenopathy in the axillae, cervical area, paraaortic areas, inguinal area, and mediastinum.
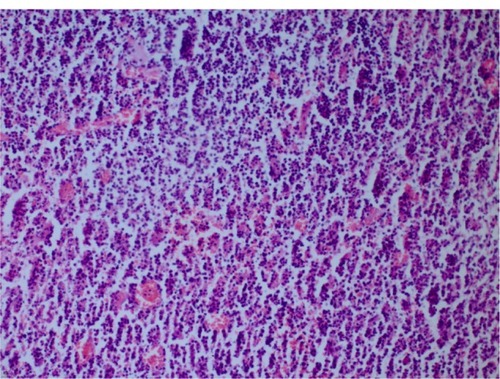
We took a cervical lymph node biopsy that showed karyorrhectic debris and the cellular infiltration of histiocytes and immunoblasts in the absence of polymorphonuclear leukocytes () and activated B-cells with histiocytes (). An immunohistochemical study showed that the lymphoid cells adjacent to the necrotic foci were strongly positive for cluster of differentiation (CD)3, and the histiocytic cells at the periphery of the necrotic foci were strongly positive for CD68, so we thought that this histological pattern was suggestive of KFD.
Figure 2 Karyorrhectic debris and cellular infiltration of histiocytes and immunoblasts in the absence of polymorphonuclear leukocytes (hematoxylin and eosin stain ×200).
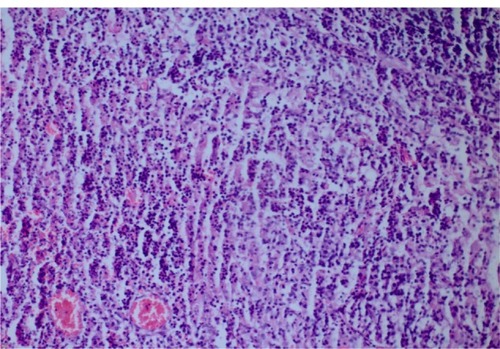
Figure 3 Histiocytes and activated B-cells (hematoxylin and eosin stain ×200).
After diagnosis, the patient received corticosteroid and hydroxychloroquine therapy. During treatment, the patient’s clinical and laboratory parameters worsened. The patient’s diagnosis was revised, but new findings were unremarkable for a particular disease. The patient’s hemoglobin values decreased, and the peripheral blood smear revealed schistocytes. Blood tests showed raised D-dimer, activated partial thromboplastin time, prothrombin time, and international normalized ratio with decreased fibrinogen. The patient’s condition quickly worsened and eventually disseminated intravascular coagulopathy (DIC) developed. She remained completely unresponsive to therapy and she subsequently died.
Discussion
KFD has a worldwide distribution, with higher prevalence noted among Japanese and other Asiatic people.Citation5 Although a viral or autoimmune pathogenesis, notably with systemic lupus erythematosus, has been suggested, the etiology still remains unknown. The patients most often present with cervical lymphadenopathy, which may be painful and can be accompanied by fever and upper respiratory tract symptoms.Citation7 However, the most common complaint is the unilateral involvement of the posterior cervical group. Other less common manifestations include fever, axillary and mesenteric lymphadenopathy, splenomegaly, parotid gland enlargement, cutaneous rash, arthralgias, myalgias, aseptic meningitis, bone marrow hemophagocytosis, and interstitial lung disease.Citation7 Erythematous macules, papules, plaques, and nodules are the forms of cutaneous lesions that can be observed in this disease. Our patient had bilateral cervical lymphadenopathy, fever, fatigue, chest and abdominal pain, as well as a maculopapular rash on her face, trunk, and upper and lower extremities. Laboratory investigations are usually unremarkable, except for an elevated ESR, mild neutropenia, and lymphocytosis in some cases.Citation8 Our patient had a high ESR and lymphocytosis. A pathologist, rather than a clinician, usually diagnoses KFD, and the diagnosis is generally based on an excisional biopsy of affected lymph nodes. Open biopsy seems to be the only reliable way to establish a diagnosis; however, some authors suggest that fine-needle biopsy may also be helpful.Citation9 The characteristic histopathological features of the disease include geographic necrosis in the paracortical areas, karyorrhectic debris, and cellular infiltration of the histiocytes and immunoblasts in an absence of granulocytes. Mitoses are often seen. The accumulation of CD68-positive stained histiocytes in the necrotic areas of lymph nodes is helpful in the diagnosis. The ratio of misdiagnosis is defined as 40%, and it is reported that non-Hodgkin lymphoma is the most common disease that has a risk of interference with KFD.Citation2 The frequent mitotic activity, especially in the areas of intensive immunoblasts and lymphoblasts, may result in a misdiagnosis of non-Hodgkin lymphoma.Citation10 In our patient, we performed a lymph node biopsy for diagnosis. The lymph node biopsy showed karyorrhectic debris, and the cellular infiltration of histiocytes and immunoblasts in an absence of polymorphonuclear leukocytes, and so the diagnosis of KFD was confirmed.
Several non-neoplastic conditions such as systemic lupus erythematosus, toxoplasmic lymphadenitis, infectious mononucleosis and cat-scratch disease can mimic KFD; the main problem for the histopathologist is to distinguish this disease from non-Hodgkin’s lymphoma.Citation8 In our patient, serological, immunological, and rheumatological tests, blood, urine and sputum cultures, and also sputum cultures for acid-fast bacilli were all negative.
Occasionally, the disease may progress to a mortal state, as in our case. Our patient rapidly developed DIC and she died. DIC, also called consumption coagulopathy and defibrination syndrome, is a systemic process characterized by both thrombosis and hemorrhage.Citation11 During this process, endothelial damage, enhanced expression, and the release of granulocyte and macrophage procoagulant substances (such as tissue factor) activate the coagulation. Increased expression and release may be a direct action of endotoxin and other membrane lipopolysaccharides, or it may be an indirect action that results from mediation via the activation of cytokines, such as interleukin-6 and tumor necrosis factor alpha.Citation12 In some studies, it has been reported that the serum concentrations of some inflammation mediators such as interferon-γ and interleukin-6 had increased during the acute phase of KFD, and they returned to normal during the convalescent phase; this suggests that these cytokines could play a role in the pathogenesis of this condition.Citation13 The occurrence of DIC, which could be due to a massive cytokine release (mainly of tumor necrosis factor alpha, interleukin-1, and interleukin-6) by the activated mononuclear cells within the many lymph nodes affected by the disease is a remarkable feature for this case.Citation14 In addition, massive release of interferon-γ probably played an important role as well. This cytokine release could explain the elevated lactate dehydrogenase levels in this patient.
No effective treatment has been established for KFD. It has a benign course and is self-limited. The patients usually require no specific treatment; the signs and symptoms usually resolve within 6 months from the time of diagnosis.Citation8 Symptomatic treatment measures such as analgesics, antipyretics, rest, and so on, may be used to relieve patients’ complaints.Citation7 Corticosteroids may be used for severe cases.Citation8 There is also a report on treatment with chloroquine and hydroxychloroquine,Citation15 and intravenous immunoglobulin was also used to effectively treat a patient with severe KFD.Citation16 In our patient, DIC developed despite treatment with corticosteroids and hydroxychloroquine, and she subsequently died.
A clinician must consider DIC when a patient with KFD shows elevations in D-dimer, activated partial thromboplastin time, prothrombin time, and international normalized ratio, and decreases in fibrinogen and hemoglobin. It must be remembered that the patients with KFD who develop DIC may progress to the point where the disease is fatal.
Disclosure
The authors report no conflicts of interest in this work.
References
- KikuchiMLymphadenitis showing focal reticulum cell hyperplasia with nuclear debris and phagocytes: a clinicopathological study. Nippon Ketsueki Gakkai ZasshiActa Hematol Jpn197235379380
- FujimotoYKojimaYYamaguchiKCervical subacute necrotizing lymphadenitisNaika197230920927
- Duskin-BitanHKivitySOlchovskyDSchibyGEzraDMouallemMKikuchi-Fujimoto diseaseIsr Med Assoc J2010121061762121090519
- NorrisAHKrasinskasAMSalhanyKEGluckmanSJKikuchi-Fujimoto disease: a benign cause of fever and lymphadenopathyAm J Med199610144014058873511
- LinHCSuCYHuangCCHwangCFChienCYKikuchi’s disease: a review and analysis of 61 casesOtolaryngol Head Neck Surg2003128565065312748557
- DorfmanRFBerryGJKikuchi’s histiocytic necrotizing lymphadenitis: an analysis of 108 cases with emphasis on differential diagnosisSemin Diagn Pathol1988543293453217625
- BoschXGuilabertAMiquelRCampoEEnigmatic Kikuchi-Fujimoto disease: a comprehensive reviewAm J Clin Pathol2004122114115215272543
- KucukardaliYSolmazgulEKunterEOnculOYildirimSKaplanMKikuchi-Fujimoto Disease: analysis of 244 casesClin Rheumatol2007261505416538388
- HsuehEJKoWSHwangWSYamLTFine-needle aspiration of histiocytic necrotizing lymphadenitis (Kikuchi’s disease)Diagn Cytopathol1993944484528261853
- TongTRChanOWLeeKCDiagnosing Kikuchi disease on fine needle aspiration biopsy: a retrospective study of 44 cases diagnosed by cytology and 8 by histopathologyActa Cytol200145695395711726124
- VincentJLDe BackerDDoes disseminated intravascular coagulation lead to multiple organ failure?. Crit Care ClinJul2005213469477
- JansenPMPixleyRABrouwerMInhibition of factor XII in septic baboons attenuates the activation of complement and fibrinolytic systems and reduces the release of interleukin-6 and neutrophil elastaseBlood1996876233723448630396
- KubotaMTsukamotoRKurokawaKImaiTFurushoKElevated serum interferon gamma and interleukin-6 in patients with necrotizing lymphadenitis (Kikuchi’s disease)Br J Haematol19969546136158982035
- ChanJKWongKCNgCSA fatal case of multicentric Kikuchi’s histiocytic necrotizing lymphadenitisCancer1989639185618622784712
- RezaiKKuchipudiSChundiVArigaRLoewJShaBEKikuchi-Fujimoto disease: hydroxychloroquine as a treatmentClin Infect Dis20043912e124e12615578393
- NoursadeghiMAgelNGibsonPPasvolGSuccessful treatment of severe Kikuchi’s disease with intravenous immunoglobulinRheumatology (Oxford)200645223523716352644