
Abstract
An autoamputated wandering calcified ovary (AWCO) is an extremely rare cause of abdominal calcification in the pediatric population. We present the magnetic resonance imaging (MRI) features of AWCO in a child. To our knowledge, the MRI features of AWCO have not been previously described in the published literature. Our case report indicates that the MRI findings are characteristic in the diagnosis of an AWCO and can completely obviate the need for invasive procedures in this mostly benign disease. An AWCO should be considered in all cases of mobile calcific opacities on radiographs in female patients. We advise that MRI be conducted in all suspected cases of AWCO for accurate and noninvasive diagnosis, and regular follow-up should be performed with ultrasound. The findings in our case report have the potential to change the course of investigations and management in suspected cases.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
Autoamputation of an ovary is an extremely rare condition.Citation1–Citation8 Torsion of an ovary or an ovarian lesion and the adnexa can lead to infarction and necrosis and subsequent amputation of the ovary.Citation1–Citation3 An amputated ovary gets calcified (dystrophic calcification) and may freely float in the peritoneal cavity.Citation3 In most cases, a blunt ending fallopian tube is noted on the involved side with the free-floating calcified ovary during surgery or laparoscopy.Citation3 Confirmation of the diagnosis of an autoamputated wandering calcified ovary (AWCO) in most of the previously reported cases was made during surgery or laparoscopy, and all of these cases were evaluated by X-rays, ultrasound, and computed tomography (CT) scan alone or in combination.Citation1–Citation8 A magnetic resonance imaging (MRI) study has not been conducted in any of these previously reported cases of AWCO.Citation1–Citation8 This is the first MRI report of its kind in the literature of an AWCO in a pediatric patient.Citation1–Citation8 We describe the characteristic MRI features of AWCO in this report, and review the literature about the autoamputation of ovaries or the adnexa.
Case material
A 9-year-old Asian Indian girl presented to the emergency department with a complaint of right lower abdominal pain. The pain was of 2 hours’ duration and colicky in nature. She was afebrile and in good general condition. No abdominal guarding, rigidity, or rebound tenderness was noted on examination. Her past medical history was not significant. She was born by normal vaginal delivery in a hospital, and the antenatal and perinatal period was uneventful. Prenatal ultrasound was not done and no radiological investigations were done since birth. Urine and blood examinations were normal. A plain erect abdominal X-ray and an abdominal ultrasound were performed. A 1.2 cm oval calcific opacity was noted in the left side of the pelvis on the abdominal plain X-ray (), and an ultrasound of the abdomen was unremarkable. She was managed conservatively with analgesics. She was sent home after the pain subsided and called again for evaluation of the left pelvic opacity. Another abdominal plain X-ray obtained after a week showed the same opacity in the pelvis in the midline (). A CT scan was performed, suspecting the opacity to be a vesical calculus, which showed an oval calcified lesion in the right adnexa (). The CT scan findings raised suspicion of an ovarian dermoid. No fat density was noted in relation to the wandering calcified pelvic lesion. MRI was performed for further evaluation. It showed an absent right ovary and a calcified lesion in the left adnexa adjacent to the left ovary (–), suggesting that it was an autoamputated wandering calcified right ovary. An absent right adnexa and a blunt-ending right fallopian tube were very well visualized on MRI, and they were best visualized on short TI inversion recovery images. A normal left ovary was very well demonstrated on T2-weighted MRI images. On fat suppressed T1-weighted images, the AWCO appeared as an oval hyperintense lesion with a central hypointense area. Peripheral hyperintensity on T1-weighted images in AWCO can be due to methemoglobin or soft calcifications, and the central hypointense area can be due to thick or dense calcifications. The AWCO did not enhance on postcontrast images. Only regular follow-up with ultrasound was advised; no treatment was given, as it is a benign condition and generally does not require surgical intervention unless complicated. Pain in the abdomen did not recur after the first episode and was considered as unrelated to the AWCO. The patient was followed up for 1 year until the writing of this report with an ultrasound study every 6 months, and no significant changes in the existing findings (or no new findings) were noted. The diagnosis by MRI completely obviated the need for laparoscopy, saving the patient from an unnecessary surgical procedure.
Figure 1 Abdominal plain X-rays showing an oval calcific opacity.
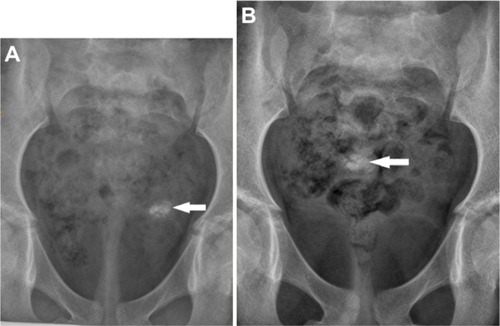
Figure 2 Axial computed tomography scan (bone window) image showing oval calcification (arrow) in the right adnexa.
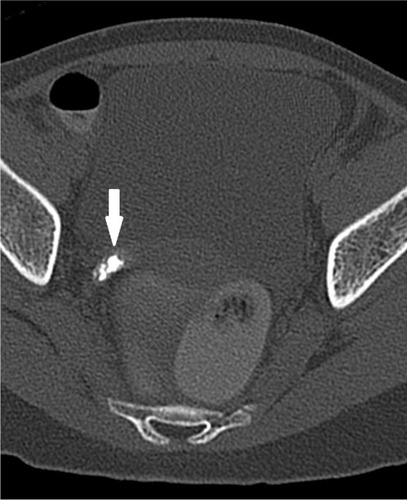
Figure 3 Axial short TI inversion recovery magnetic resonance image showing absent right adnexa and blunt ending right fallopian tube.
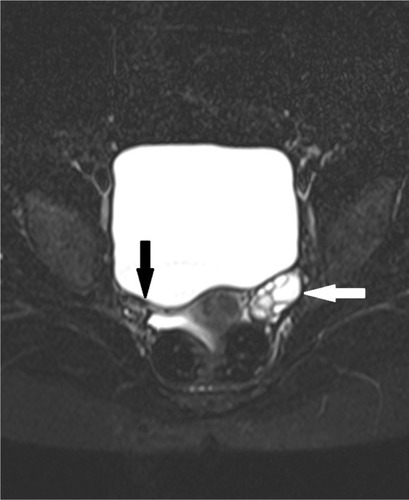
Figure 4 Axial fat suppressed T1-weighted image showing oval hyperintense lesion with thick central calcification in the left adnexa (arrow).
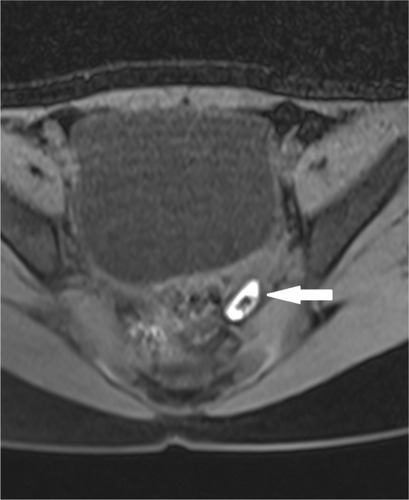
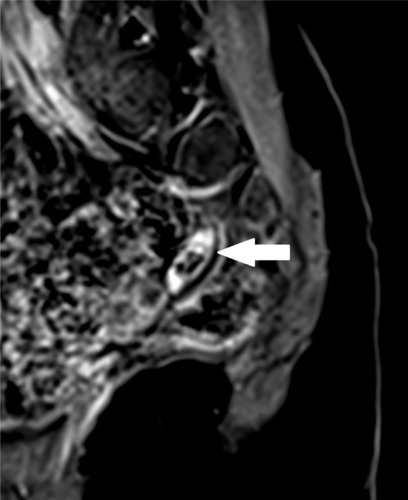
Figure 5 Sagittal post-gadolinium contrast T1-weighted fat suppressed image shows nonenhancing calcified oval lesion (arrow) in the left adnexa.
Discussion
The autoamputation of an ovary is an extremely rare cause of calcification on an abdominal plain X-ray in the pediatric population.Citation3 Common causes of the pelvic calcification in young females include teratoma, ovarian neoplasm, chronic ovarian inflammation, appendicolith, urinary bladder calculus, lymph nodal calcification, calcification in a Meckel’s diverticulum, gallstone, or neoplasms of the pelvic bones.Citation9
Autoamputation of an ovary can be unilateral or bilateral, and it can occur during the prenatal or neonatal period.Citation3 It is more common on the right side.Citation1–Citation3 The autoamputated ovary is mostly found incidentally while investigating symptoms not related to it, on prenatal ultrasound, or during surgery for different or related causes.Citation1–Citation8
In addition to our case, 96 cases of autoamputated ovaries were noted in the published literature, for a total of 97 cases.Citation1–Citation3 Half (49/97) of these cases involved pediatric patients (<18 years).Citation1–Citation3 Most of these cases were diagnosed via antenatal ultrasonography, likely because it is a very commonly performed examination.Citation3 A wandering cystic abdominal mass was demonstrated on antenatal ultrasound in almost all of these cases.Citation1–Citation3 In all cases, in older children, the diagnosis was made after laparoscopy or during surgery.Citation1–Citation3 Only 14 cases of radiologically demonstrated wandering calcified ovary were identified in the literature, and MRI findings have not yet been described in this group.Citation3 In our case, MRI clearly demonstrated the lack of an ovary/adnexa and a freely mobile oval calcified lesion (autoamputated ovary) in the pelvis, suggesting that it was an autoamputated wandering calcified right ovary. The MRI findings are characteristic in the diagnosis of an AWCO. Ultrasonography can show the absence of the adnexa, but MRI is superior in delineating soft tissue morphology. Also, ultrasonography may not demonstrate the displaced calcified ovary.Citation10 CT scans can show calcifications very well, but they are limited in terms of resolving soft tissue abnormalities.Citation9 Radiation risk from CT scans can be a concern in young females.Citation11 X-rays can only demonstrate mobile calcifications. Therefore, MRI is far better in conclusively demonstrating the absent adnexa and also in localizing the wandering calcified ovary, thus making it the investigation of choice in suspected cases of AWCO.
Conclusion
The MRI findings are characteristic in the diagnosis of an AWCO, and they can completely obviate the need for laparoscopy in this benign condition. An AWCO should be suspected in all cases of mobile calcific opacities on radiographs in females. We advise that MRI be performed in all suspected cases of AWCO for accurate and noninvasive diagnosis, and that regular follow-up with ultrasound be performed. The findings in our case report have the potential to change the management of AWCO in suspected cases.
Disclosure
The authors report no conflicts of interest in this work.
References
- TrotmanGEZamoraMGomez-LoboVNon-surgical management of the auto-amputated adnexa in the neonate: a report on two casesJ Pediatr Adolesc Gynecol Epub2013926
- FocseneanuMAOmurtagKRattsVSMerrittDFThe auto-amputated adnexa: a review of findings in a pediatric populationJ Pediatr Adolesc Gynecol201326630531323287601
- UygunIAydogduBOkurMHOtcuSThe first report of an intraperitoneal free-floating mass (an autoamputated ovary) causing an acute abdomen in a childCase Rep Surg2012201261573423119216
- KogaKHiroiHOsugaYNagaiMYanoTTaketaniYAutoamputated adnexa presents as a peritoneal loose bodyFertil Steril201093396796819394607
- MatsushitaHKurabayashiTYanaseTHashidateHAutoamputation of an ovarian cyst: a case reportJ Reprod Med20095411–1270971120120906
- PeitsidouAPeitsidisPGoumalatsosNPapaspyrouRMitropoulouGGeorgouliasNDiagnosis of an autoamputated ovary with dermoid cyst during a Cesarean sectionFertil Steril20099141294.e9e1219176224
- VisnjicSDomljanMZupancicBTwo-port laparoscopic management of an autoamputated ovarian cyst in a newbornJ Minim Invasive Gynecol200815336636918439514
- KusakaMMikuniMEctopic ovary: a case of autoamputated ovary with mature cystic teratoma into the cul-de-sacJ Obstet Gynaecol Res200733336837017578369
- KaeserMAMcDonaldJKKettnerNWA calcific pelvic mass in a woman with chronic spinal pain: a case of mature cystic teratomaJ Chiropr Med201110432733222654694
- McCarthySMagnetic resonance imaging in obstetrics and gynecologyMagn Reson Imaging19864159663512947
- Berrington de GonzálezAMaheshMKimKPBhargavanMLewisRMettlerFLandCProjected cancer risks from computed tomographic scans performed in the United States in 2007Arch Intern Med2009169222071207720008689