
Abstract
Air localized within the spinal canal is called pneumorrhachis. In the case of pneumorrhachis, air can be present in the extradural, the intradural, or the subarachnoid space of the spinal canal. The air within the soft tissue of the posterior mediastinum may dissect along fascial planes, through the intervertebral neural foramina, and into the extradural or the subarachnoid space. Nontraumatic pneumorrhachis is a rare presentation. Most of the time, pneumorrhachis is asymptomatic, remains localized, and resolves spontaneously. There are very few reports of combined presence of pneumomediastinum and extradural pneumorrhachis not associated with thoracic injury in the published literature. We report a rare case of pneumorrhachis, pneumomediastinum, pneumothorax, and surgical emphysema in an adult female patient developed after a bout of violent cough related to bronchial asthma.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
Pneumorrhachis is defined as air localized within the spinal canal: in the extradural space; in the intradural space; or in the subarachnoid space. It is a rare condition and is usually incidentally detected during radiological investigations.Citation1 In the radiology practice, it is often associated with severe spinal trauma or is iatrogenic. Most of the time, pneumorrhachis is asymptomatic and is not clinically significant. Pneumorrhachis tends to remain localized and resolves spontaneously.Citation1
Common causes of pneumorrhachis include: penetrating trauma; an invasive procedure like an epidural analgesia or a lumbar puncture; spontaneous or traumatic pneumomediastinum and pneumothorax; degenerative disc disease; or extradural abscess. Bronchial asthma that causes pneumorrhachis is a very rare condition.Citation1–Citation6 To our knowledge, very few cases of this association are reported in the published literature.Citation1–Citation6 Pneumorrhachis secondary to interstitial lung disease was reported by Sandhya et al in 2011.Citation7 A case of pneumorrhachis related to the common flu was recently reported.Citation8 Pneumorrhachis secondary to peanut aspiration was also reported.Citation9 We present a rare case of pneumorrhachis, pneumomediastinum, pneumothorax, and surgical emphysema secondary to an acute attack of bronchial asthma.
Case report
An 18-year-old female Arab, a known asthmatic, presented to the emergency department of our hospital with complaints of chest pain and a nonproductive cough of 1-hour duration. She was conscious and well-oriented to the surroundings but had mild dyspnea. There was no history of receiving assisted mechanical ventilation. There was no previous history of pulmonary tuberculosis, recent trauma, surgery, or other intervention.
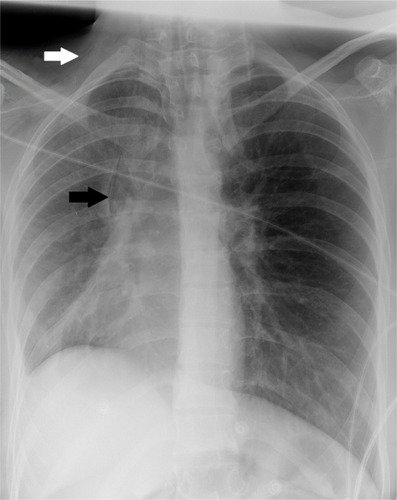
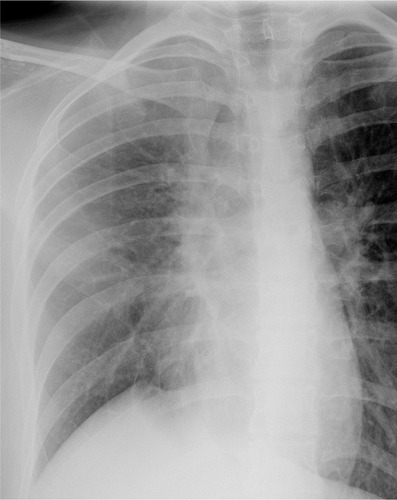
Vital parameters were stable, and body temperature was normal. There was subcutaneous emphysema involving the right side of the neck. Auscultation of the chest did not reveal any significant abnormality. A chest radiograph was obtained, which revealed surgical emphysema along the upper part of the right lateral chest wall and the right side of the neck. Minimal pneumomediastinum was also noted with air within the superior mediastinum on the right. A loss of volume of the right lung was noted with a shift of mediastinum to the right and elevated right diaphragmatic dome (). No lung consolidation, pneumothorax, or pleural collection was noted. The patient collapsed immediately after the chest radiograph was obtained. She was intubated and given intravenous fluids and vasopressors to control the hypotension. Her condition stabilized after 2 hours. The portable bedside chest radiograph revealed increased severity of pneumomediastinum, surgical emphysema, right lung collapse, and mediastinal shift to the right ().
Figure 1 Frontal chest radiograph.
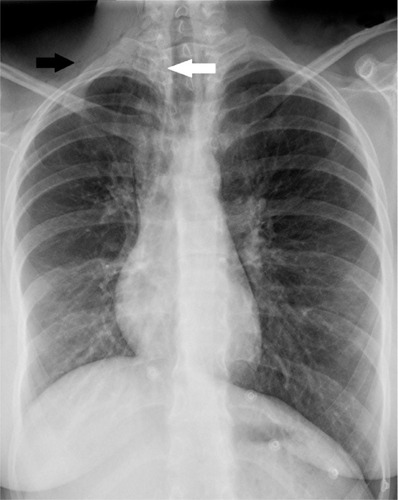
Figure 2 Portable bedside semi-sitting chest radiograph.
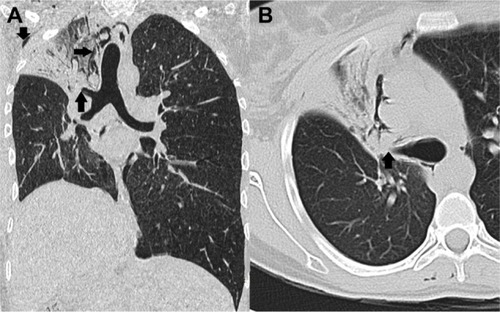
Computed tomography (CT) imaging of the thorax was also performed, which confirmed the dissection of air into the mediastinal and subcutaneous spaces (). A CT scan also revealed air within the posterior spinal extradural space in the thoracic spine ( and ), minimal pneumothorax on the right, and obstruction of the segmental right upper lobe bronchus by mucus plugs ().
Figure 3 Axial nonenhanced chest CT scan.
Abbreviation: CT, computed tomography.
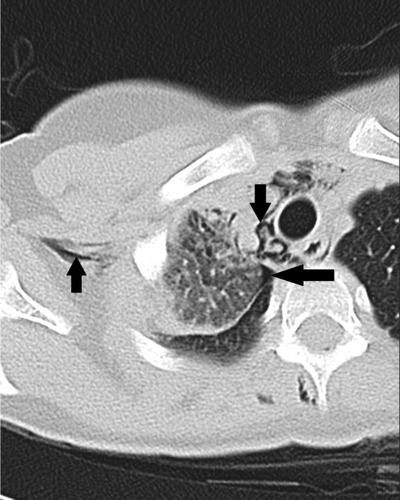
Figure 4 Axial nonenhanced chest CT scan.
Abbreviation: CT, computed tomography.

Figure 5 Sagittal reformatted CT scan images of chest.
Abbreviation: CT, computed tomography.
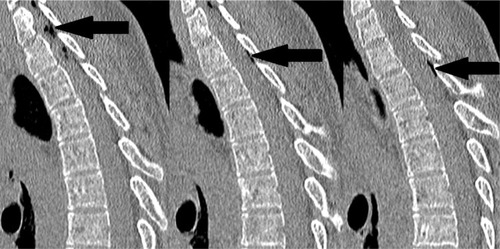
Figure 6 Coronal and axial reformatted CT scan images of the chest.
Abbreviation: CT, computed tomography.
She was hospitalized and treated with antibiotics, bronchodilators, oxygen inhalation, and other conservative measures. A bronchoscopic removal of mucus plugs and thick secretions was also performed. After only 5 days, clinical findings got better. The chest radiograph revealed resolution of the pneumomediastinum and surgical emphysema and a significant improvement of the right lung collapse and mediastinal shift to the right (). She improved rapidly during her stay in the hospital and was discharged after 7 days.
Figure 7 Follow-up frontal chest radiograph.
Discussion
Pneumorrhachis can be classified by etiology into traumatic, nontraumatic, and iatrogenic types.Citation1 Pneumorrhachis usually does not cause any symptoms and is, most of the time, incidentally detected. Pneumorrhachis that is not associated with trauma or intervention is a very rare condition. Pneumorrhachis has been described secondary to spontaneous or nontraumatic pneumomediastinum or pneumothorax.Citation10 There are very few reports of the combined presence of pneumomediastinum and extradural pneumorrhachis that are not associated with thoracic injury in the published literature.
Our patient developed pneumorrhachis, pneumomediastinum, pneumothorax, and surgical emphysema without any trauma. Air within the spinal canal is usually an isolated finding. It may be detected in the cervical, thoracic, or lumbosacral regions – or the entire spinal canal. Pneumorrhachis commonly remains localized.Citation1 In our case, pneumorrhachis was extradural and localized in the lower cervical and upper thoracic spine. Pneumorrhachis is primarily a clinical imaging diagnosis, and clinicians do not play any role in its diagnosis, as pneumorrhachis is almost always asymptomatic. Pneumorrhachis can be diagnosed on a radiograph or a CT scan of the spine. A CT scan is the investigation of choice in its diagnosis.Citation1,Citation8–Citation11
In our case, also, the pneumorrhachis was asymptomatic and incidentally detected on a chest CT scan. A violent cough can sometimes occur in bronchial asthma, may cause sudden elevation of intra-alveolar pressure, and consequently may lead to a rupture of the peripheral pulmonary alveoli.Citation1
The leaked air dissects through the perivascular interstitium of the lung and may traverse through the fascial planes from the retropharyngeal space or the mediastinum. Air traversing through the fascial planes may pass through the intervertebral neural foramina into the spinal canal.Citation1 There are no barriers along the fascia to prevent this spread of air from the chest to the spinal canal.Citation1
The patient collapsed immediately after obtaining the first radiograph likely due to an acute lung collapse, which – in turn – may have been caused by an obstruction by a mucus plug or a blood clot. Increased right lung collapse was detected on the subsequent chest radiograph. The severe collapse of a lung as a result of large mucus plugs occluding major airways has been described in many studies on different lung diseases, including bronchial asthma.Citation12 Occluding large mucus plugs may cause reduced gas exchange, increasing inspiratory pressure, and breathing difficulty.Citation12
In most cases, extradural pneumorrhachis is self-limiting and resolves spontaneously when the etiological entity is taken care of. In our case also, the pneumorrhachis resolved spontaneously. A rare case of symptomatic pneumorrhachis having neurological deficits has been reported.Citation11
Conclusion
In conclusion, we present a very rare case of extradural pneumorrhachis due to pneumomediastinum, which – in turn – was secondary to bronchial asthma. Most cases of pneumorrhachis can be managed conservatively, as spontaneous resolution is common. Pneumorrhachis is, thus, a benign condition. However, it is essential for the treating physician to study carefully the associated disease conditions and neurological status of the patient, as neurological deficits may occur in some cases.Citation11
Disclosure
The authors report no conflicts of interest in this work.
References
- KaraoglanACalMAOrkiAArpaozuBMColakAPneumorrhachis associated with bronchial asthma, subcutaneous emphysema and pneumomediastinumTurk Neurosurg201121466666822194136
- Pérez FrutosMDCerezo AriasMOCórdoba LópezAGranado MartínezD[Pneumorrhachis: a rare complication of an asthma episode]Med Intensiva2011352130131 Spanish20542355
- MandenPKSiddiquiAHPneumorrhachis, pneumomediastinum, pneumopericardium and subcutaneous emphysema as complications of bronchial asthmaAnn Thorac Med20094314314519641647
- EesaMKandpalHSharmaRMisraASpontaneous pneumorrhachis in bronchial asthmaActa Radiol200647767267416950703
- OertelMFKorinthMCReingesMHGilsbachJMPneumorrhachis of the entire spinal canalJ Neurol Neurosurg Psychiatry2005767103615965224
- van der KloosterJMGrootendorstAFOphofPJBrouwersJWPneumomediastinum: an unusual complication of bronchial asthma in a young manNeth J Med19985241501549646625
- SandhyaPKeshavaSNDandaDPadhanPMathewJGibikoteSPneumorrhachis and pneumomediastinum in connective tissue disease-related interstitial lung disease: case series from a tertiary care teaching hospital in South IndiaRheumatol Int20123251415141921442175
- PatelVRavalGGavadiaKPneumothorax, pneumomediastinum, subcutaneous emphysema and pneumorrhachis as complications of common fluAm J Case Rep20121319820123569528
- SankarJJainASureshCPPeanut aspiration leading to pneumorrhachis in a pre-schoolerBMJ Case Rep20132013
- MigeotMKesslerREtxeberria IzalARutgersMPGilleMPneumorrhachis associated with a spontaneous pneumomediastinumRev Neurol (Paris)2013169217317423079853
- KimSWSeoHJSymptomatic epidural pneumorrhachis : a rare entityJ Korean Neurosurg Soc2013541656724044086
- GurjarMSinghalSPoddarBSinghRKCollapse of left lung after endotracheal intubation: Is it always due to misplacement of tube?J Emerg Trauma Shock20103330520930996