
Abstract
Introduction
Sacral insufficiency fractures are an important cause of lower back pain in the elderly. Clinically and radiologically, they must be distinguished from osseous metastases, which frequently coexist. To date, no case report has comprehensively explored the full range of diagnostic hurdles and potential pitfalls.
Case presentation
We report the case of a 70-year-old Caucasian female who presented to our services with a short history of progressive back pain without any history of trauma. A prior history of breast cancer was noted. Bone scintigraphy was initially reported as consistent with metastatic sacral deposits. Further characterization with magnetic resonance imaging and computed tomography revealed bilateral insufficiency fractures of the sacral alar. The patient responded well to conservative management.
Conclusion
To avoid misdiagnosis, particularly in those who are also at risk of osseous metastases, sacral insufficiency fractures must always be considered as a cause of lower back pain.
Introduction
Stress fractures can be classified as either fatigue or insufficiency fractures.Citation1 Intuitively, the first describes fractures occurring within normal bone architecture that has been exposed to abnormal or repetitive stresses.Citation2 Conversely, insufficiency fractures occur in abnormal bone under normal stress. Insufficiency fractures of the sacrum (SIFs) were first described by Lourie in 1982.Citation3 Patients undergoing radiotherapy to treat malignant tumors may be at particular risk of SIFs,Citation4 with a prevalence of 89% for patients undergoing radiotherapy for cervical cancer.Citation5 Elderly women with osteoporosis are also at high risk,Citation6 with almost all patients with SIFs demonstrating severe osteopenia on dual X-ray absorptiometry.Citation7 Additionally, rheumatoid arthritis, Paget’s disease, renal osteodystrophy, and hyperparathyroidism have been reported as risk factors.Citation8,Citation9 Sacral stress fractures have occasionally been reported during the last trimester of pregnancy and the early postpartum period.Citation10,Citation11 While preceding trauma may be reported, it is usually minorCitation12 or often completely absent.Citation13
Patients suffering from SIFs often present with limited mobility caused by acute and intractable lumbar or pelvic pain without clear evidence of trauma. Neurological symptoms are usually absent, but radiculopathy has a reported incidence of 5%–6%Citation7 and sphincter disturbance has also been described.Citation14 Pain typically improves on lying supine and increases on weight-bearing. Patients may also complain of parasymphyseal discomfort due to the high incidence of concomitant pubic rami fractures.Citation15
The lack of specific clinical findings makes diagnosis challenging and SIFs remain an under-recognized cause of lower back pain. In fact, there is often a delay of up to 2 months before dedicated sacral imaging is performed.Citation16 In this report, we describe the diagnostic challenge of detecting SIFs and aim to increase awareness of the potential pitfalls.
Case presentation
A 70-year-old Caucasian patient was admitted through the emergency department with severe back pain. She had first experienced discomfort 14 days previously, which had progressively worsened. No history of trauma, however minor, could be recalled. The pain was localized to her lower back with no radicular symptoms. One week after the initial discomfort, the patient was unable to mobilize and had become bedridden. No neurology was demonstrable on examination. Palpation of the lumbar vertebrae was unremarkable but direct pressure over both sacroiliac joints resulted in a marked exacerbation of her pain.
A history of primary breast cancer was reported. The disease was detected during mammographic screening with no radiographic or histological evidence of distant metastasis. As such, the patient had undergone a wide local excision and local radiotherapy 4 years prior. Additionally, she described a longstanding history of rheumatoid arthritis which was controlled with disease-modifying antirheumatic drugs.
Upon admission, our patient was apyrexial and had a normal white blood cell count. Interestingly, raised alkaline phosphatase (ALP) was found at 278 IU/L (reference range: 30–130 IU/L) with normal adjusted calcium. The remaining liver function tests were normal. Marginally raised C-reactive protein was seen at 15 mg/L (reference range: <10 mg/L).
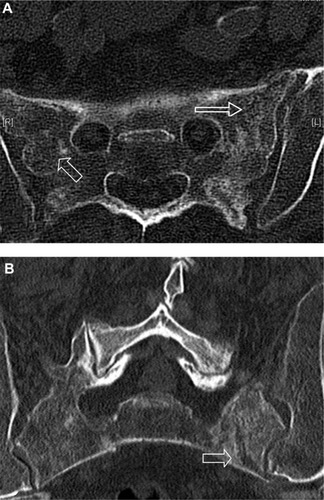
Plain film radiographs of her lumbar spine demonstrated scoliosis but no fractures or suspicious lesions. Similarly, radiographs of her pelvis did not detect any abnormalities. In view of her medical history, bone scintigraphy was performed. This demonstrated a bilateral increase in uptake of technetium-99m in the sacrum and pubic rami (). Initially, this was thought to be consistent with metastatic disease. Subsequently, spinal magnetic resonance imaging (MRI) was performed to characterize the extent of the lesions. T1-weighted images of the sacrum demonstrated symmetrical hypointense areas within both sacral alar (). Whilst symmetry was not in keeping with a neoplastic process, no fracture line was evident. A computed tomography (CT) scan of the sacral region highlighted bilateral fracture lines through the sacral alar in keeping with insufficiency fractures (). CT also demonstrated a right-sided anterior pubic rami fracture.
Figure 1 Bone scintigraphy showing increased sacral uptake bilaterally (hollow arrows) and pubic bone (solid arrow).
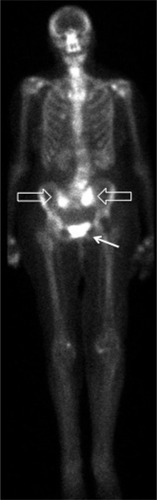
Figure 2 Axial T1-weighted MRI image of sacrum.
Abbreviation: MRI, magnetic resonance imaging.
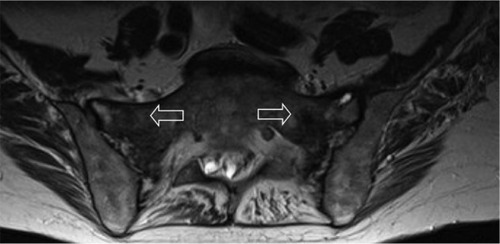
Figure 3 CT images of sacrum.
Abbreviation: CT, computed tomography.
Her pain was successfully managed with a combination of simple and transcutaneous opioid analgesia. The patient was able to mobilize with the aid of a walking frame and was discharged home on day 12 of admission. Subsequent follow-up at 1 month found her pain, mobility, and independence to be gradually improving.
Discussion
Several reports have previously highlighted the variable and nonspecific presentation of SIFs that makes diagnosis challenging.Citation6,Citation9 Whilst not specific for SIFs, Denis et al have classified traumatic sacral fractures into zones,Citation17 which can help predict the clinical features. Zone 1 fractures lie laterally, involving the sacral alar, with zones 2 and 3 fractures progressing medially to involve the neural foramina and sacral bodies, respectively. Consequently, unilateral radicular symptoms are often reported with zone 2 fractures and bilateral neurological symptoms with sphincter dysfunction can occur with involvement of zone 3.
Laboratory investigations are of limited value. Often, no abnormality is found, although a mildly raised ALP, a marker of bone formation, is sometimes seen.Citation18 Of note, ALP is also raised in metastatic disease.Citation19 Radiographs of the pelvis, sacrum, and lumbar spine may initially be used to identify fractures. However, the presence of fecal material, vascular calcifications, and bowel gas can mask incomplete fractures, and radiographs detect SIFs in less than 40% of cases.Citation20
Diagnostic difficulty is compounded by a history of malignancy in approximately 45% of patients with SIFs.Citation21 Consideration of this clinical entity is therefore paramount if overdiagnosis of osseous metastasis is to be avoided. Bone scintigraphy with technetium-99m-labeled medronic acid is one of the most sensitive (96%) examinations.Citation22 While present in less than 40% of patients, the H-sign is considered pathognomonic for SIFs.Citation23 However, isolated sacral metastases presenting with focal sacral uptake have also been reported.Citation24
MRI, with sensitivity approaching 100%, is considered to be the gold standard for identifying SIFs.Citation24 Most cases demonstrate both marrow edema and a fracture line, although the latter is absent in 7% of cases.Citation24 The absence of a fracture line can create uncertainty. Although less sensitive (60%–75%),Citation24 CT can be used in combination with MRI. Previous reports have noted that the absence of cortical destruction and/or a soft tissue mass effectively rules out bone metastases ().Citation25,Citation26
Table 1 Summary of articles published on the imaging modalities utilized for the investigation of SIFs
Traditionally, treatment of SIFs has been limited to conservative management strategies comprising bed rest, pain control, and physical therapy, with symptoms usually improving within 12 months.Citation27,Citation28 However, prolonged bed rest, particularly in elderly patients, has a significant morbidity. In particular, high incidences of deep vein thrombosis and pulmonary embolism have been reported.Citation29 Early physical therapy has been advocated as a means of reducing this morbidity and encouraging fracture healing through the promotion of osteoblast-mediated bone formation.Citation30 However, good quality prospective trials supporting early physical therapy in SIFs are currently lacking.
Sacroplasty has also emerged as a potential treatment and involves fluoroscopic or CT-guided injection of cement into the fractured sacrum. Initially used as a treatment for sacral metastases, it was first described as a treatment for SIFs in 2002 by Garant.Citation31 As yet, no randomized trials are available, and the literature is restricted to small retrospective case series with variable, and often invalidated, outcome measures. Whilst these need to be interpreted cautiously, they suggest a rapid and sustained improvement in pain, reduced use of narcotic analgesia, and improvement in mobility scores.Citation32,Citation33 In addition, an improved ability to perform activities of daily living has also been reported.Citation34 The main risk of sacroplasty is leakage of cement outside of the fracture line, with risk of neurological compromise. Leakage of cement has been reported but in only one case did this result in transient radiculopathy,Citation32 and in none were long-term sequelae described.Citation33 As a means of reducing complications, augmentation with a balloon-assisted technique, sacral kyphoplasty, has been proposed.Citation35 The creation of a compacted bony layer outside the balloon could, in theory, reduce cement extravasation. Supporting this technique, a cadaveric study demonstrated that cement deposition was better localized within the cortical boundaries.Citation36
Clearly, stronger evidence is required before the widespread use of sacroplasty over conservative management can be supported. It has also been suggested that since sacroplasty disrupts normal osseous healing, it may only be indicated in patients with delayed union or pain not responding to conservative measures.Citation37 However, the best method of conservative management remains equally uncertain. This is an area of much needed research ().
Table 2 A selection of previously reported case series on the various treatments of SIFs
Conclusion
The diagnostic difficulty of SIFs has previously been recognized. To our knowledge, this is the first report to highlight the full range of diagnostic hurdles; in particular, we draw attention to the limitations of each imaging modality. Awareness of SIFs is important if an erroneous misinterpretation for metastatic disease is to be avoided.
Consent
Written informed consent was obtained from the patient for publication of this manuscript and any accompanying images. A copy of the written consent is available for review from the Editor-in-Chief of this journal.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Acknowledgment
With thanks to Sarah Brice for her support and academic input.
Disclosure
The authors report no conflicts of interest in this work.
References
- PentecostRLMurrayRABrindleyHHFatigue, insufficiency, and pathologic fracturesJAMA19641871001100414102934
- PommeringTLKluchuroskyLOveruse injuries in adolescentsAdolesc Med State Art Rev200718195120 ix18605393
- LourieHSpontaneous osteoporotic fracture of the sacrum. An unrecognized syndrome of the elderlyJAMA198224867157177097924
- MammoneJFSchweitzerMEMRI of occult sacral insufficiency fractures following radiotherapySkeletal Radiol19952421011047747173
- BlomlieVRofstadETalleKSundførKWinderenMLienHHIncidence of radiation-induced insufficiency fractures of the female pelvis: evaluation with MR imagingAJR Am J Roentgenol19961675120512108911181
- WildAJaegerMHaakHMehdianSHSacral insufficiency fracture, an unsuspected cause of low back pain in elderly womenArch Orthop Trauma Surg20021221586011995886
- Gotis-GrahamIMcGuiganLDiamondTSacral insufficiency fractures in the elderlyJ Bone Joint Surg Br19947668828867983111
- De SmetAANeffJRPubic and sacral insufficiency fractures: clinical course and radiologic findingsAJR Am J Roentgenol198514536016063875262
- DasguptaBShahNBrownHGordonTETanquerayABMellorJASacral insufficiency fractures: an unsuspected cause of low back painBr J Rheumatol19983777897939714359
- RousièreMKahanAJob-DeslandreCPostpartal sacral fracture without osteoporosisJoint Bone Spine2001681717311235785
- SchmidLPfirrmannCHessTSchlumpfUBilateral fracture of the sacrum associated with pregnancy: a case reportOsteoporos Int1999101919310501786
- NewhouseKEel-KhouryGYBuckwalterJAOccult sacral fractures in osteopenic patientsJ Bone Joint Surg Am19927410147214771364816
- FinielsHFinielsPJJacquotJMStrubelDFractures du sacrum par insuffisance osseuse: meta-analyse de 508 cas [Fractures of the sacrum caused by bone insufficiency: meta-analysis of 508 cases]La Presse Medicale1997263315681573 French9452753
- MuthukumarTButtSHCassar-PullicinoVNMcCallIWCauda equina syndrome presentation of sacral insufficiency fracturesSkeletal Radiol200736430931317177021
- AretxabalaIFraizEPérez-RuizFRíosGCalabozoMAlonso-RuizASacral insufficiency fractures. High association with pubic rami fracturesClin Rheumatol200019539940111055834
- GrangierCGarciaJHowarthNRMayMRossierPRole of MRI in the diagnosis of insufficiency fractures of the sacrum and acetabular roofSkeletal Radiol19972695175249342810
- DenisFDavisSComfortTSacral fractures: an important problem. Retrospective analysis of 236 casesClin Orthop Relat Res198822767813338224
- SchindlerOSWaturaRCobbyMSacral insufficiency fracture: an under-recognized conditionCurr Orthopaed2003173234239
- MaynePDThakrarSRosalkiSBFooAYParbhooSIdentification of bone and liver metastasis from breast cancer by measurement of plasma alkaline phosphatase isoenzyme activityJ Clin Pathol19874043984033584482
- PehWCKhongPLShamJSHoWYYeungHWSacral and pubic insufficiency fractures after irradiation of gynaecological malignanciesClin Oncol (R Coll Radiol)1995721171227619761
- LundinBBjörkholmELundellMJacobssonHInsufficiency fractures of the sacrum after radiotherapy for gynaecological malignancyActa Oncol19902922112152334574
- FujiiMAbeKHayashiKHonda sign and variants in patients suspected of having a sacral insufficiency fractureClin Nucl Med200530316516915722819
- RiesTDetection of osteoporotic sacral fractures with radionuclidesRadiology198314637837856828693
- CabarrusMCAmbekarALuYLinkTMMRI and CT of insufficiency fractures of the pelvis and the proximal femurAJR Am J Roentgenol20081914995100118806133
- GacettaDJYandowDRComputed tomography of spontaneous osteoporotic sacral fracturesJ Comput Assist Tomogr198486119011916501631
- TsuchidaTKosakaNSugimotoKItohHSacral insufficiency fracture detected by FDG-PET/CT: report of 2 casesAnn Nucl Med200620644544816922475
- RawlingsCE3rdWilkinsRHMartinezSWilkinsonRHJrOsteoporotic sacral fractures: a clinical studyNeurosurgery1988221 Pt 172762449628
- WeberMHaslerPGerberHInsufficiency fractures of the sacrum. Twenty cases and review of the literatureSpine (Phila Pa 1976)19931816250725128303455
- BabayevMLachmannENaglerWThe controversy surrounding sacral insufficiency fractures: to ambulate or not to ambulate?Am J Phys Med Rehabil200079440440910892628
- ChaoEYInoueNKooTKKimYHBiomechanical considerations of fracture treatment and bone quality maintenance in elderly patients and patients with osteoporosisClin Orthop Relat Res2004425122515292783
- GarantMSacroplasty: a new treatment for sacral insufficiency fractureJ Vasc Interv Radiol200213121265126712471192
- FreyMEDepalmaMJCifuDXBhagiaSMCarneWDaitchJSPercutaneous sacroplasty for osteoporotic sacral insufficiency fractures: a prospective, multicenter, observational pilot studySpine J20088236737317981097
- BayleyESrinivasSBoszczykBMClinical outcomes of sacroplasty in sacral insufficiency fractures: a review of the literature. Eur Spine JSep200918912661271
- WhitlowCTMussat-WhitlowBJMatternCWBakerMDMorrisPPSacroplasty versus vertebroplasty: comparable clinical outcomes for the treatment of fracture-related painAJNR Am J Neuroradiol20072871266127017698526
- DeenHGNottmeierEWBalloon kyphoplasty for treatment of sacral insufficiency fractures. Report of three casesNeurosurg Focus2005183e715771397
- BettsASacral vertebral augmentation: confirmation of fluoroscopic landmarks by open dissectionPain Physician2008111576518196170
- EharaSPercutaneous sacroplasty for osteoporotic insufficiency fracturesAJR Am J Roentgenol20061862580 author reply 580–58116423974
- SchneiderRYacovoneJGhelmanBUnsuspected sacral fractures: detection by radionuclide bone scanningAJR Am J Roentgenol198514423373413871281
- ByunWMJangHWKimSWJangSHAhnSHAhnMWDiffusion-weighted magnetic resonance imaging of sacral insufficiency fractures: comparison with metastases of the sacrumSpine (Phila Pa 1976)20073226E820E82418091477
- LerouxJLDenatBThomasEBlotmanFBonnelFSacral insufficiency fractures presenting as acute low-back pain. Biomechanical aspectsSpine (Phila Pa 1976)19931816250225068303454
- BrookALMirskyDMBelloJAComputerized tomography guided sacroplasty: a practical treatment for sacral insufficiency fracture: case reportSpine (Phila Pa 1976)20053015E450E45416094265
- StrubWMHoffmannMErnstRJBulasRVSacroplasty by CT and fluoroscopic guidance: is the procedure right for your patient?AJNR Am J Neuroradiol2007281384117213421