
Abstract
We report a rare case of sling shot injury that presented with a gunshot-like wound with preseptal cellulitis, in a toddler. An 11-month-old Malay child presented with a gunshot-like wound over the forehead following sling shot injury. On examination, he had a deep circular laceration wound over the forehead, measuring 2.0 cm in diameter, with minimal bleeding. There was no obvious foreign body seen inside the wound and no palpable foreign body surrounding the wound. The gunshot-like wound was associated with left preseptal cellulitis. A skull X-ray showed a white opaque foreign body in the left frontal bone. Computed tomography (CT) scan of orbit and brain revealed a left comminuted fracture of the left orbital roof, and left frontal brain contusion with prelesional edema. Wound exploration was performed and revealed a 0.5 cm unshattered marble embedded in the left frontal bone. The marble and bone fragments were removed. The left preseptal cellulitis responded well to intravenous antibiotic and topical antibiotic.
Introduction
Sling shots, also known as hand catapults or wrist cannons, are a small hand-powered weapon invented and used since the 18th century as a military weapon. It is an impressive hunting weapon as it is generally easy to use and launches projectiles at high velocities. Over the years, it has become popular among children and preteens, used in games or as a toy. Steel balls are usually used as sling shot ammunition, but some use stones, marbles, and air gun pellets.Citation1 We report a case of sling shot injury that presented with a gunshot-like wound with preseptal cellulitis.
Case report
An 11-month-old boy was brought in to the emergency department following a sling shot injury over the forehead. The mother was unsure of the mechanism of injury. She mentioned that she was busy in the kitchen and told her eldest child, an 11-year-old daughter, and her 6-year-old son to look after the 11-month-old baby boy. They were playing with a sling shot during that time. She only rushed out when she heard a loud cry from the living room and noticed both her older children running away to their room. Her baby was crying on the floor, and there was profuse bleeding from his forehead.
On examination at the emergency unit, the child was alert and conscious. He had a deep circular laceration wound over the forehead, just above the left eyebrow, measuring 2.0 cm in diameter and resembling a gunshot-like wound, with minimal bleeding (). There was no obvious foreign body seen inside the wound and no palpable foreign body surrounding the wound. The left upper eyelid was swollen and erythematous. Anterior segment examination showed subconjunctival hemorrhage superiorly, associated with chemosis. The cornea and sclera were normal, with a deep anterior chamber and reactive pupil. There was no relative afferent pupillary defect, suggesting no optic nerve involvement. Posterior segment examination was unremarkable.
Figure 1 Gunshot-like wound over the forehead with left preseptal cellulitis.

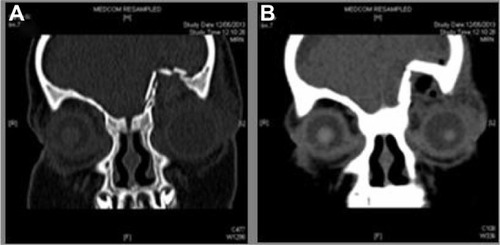
The child was treated with intravenous ceftriaxone 500 mg, every 12 hours for 1 week, and a topical eye drop combination of betamethasone sodium phosphate and gentamicin sulfate, every 8 hours, for left eye preseptal cellulitis. A skull X-ray was performed to rule out any retained foreign body at the wound region. The skull X-ray showed the presence of a round opaque foreign body measuring 0.5 cm in diameter, in the left frontal bone region (). Computed tomography (CT) scan of the orbit and brain revealed comminuted fracture of the left orbital roof, and left frontal brain contusion with prelesional edema ().
Figure 2 Skull X-ray showed a round opaque foreign body in the left frontal bone region (A) lateral view, (B) antero-posterior view.
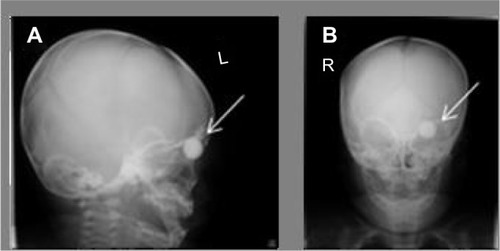
Figure 3 Computed tomography scan of orbit and brain showed comminuted fracture of the left orbital roof (A) and left frontal brain contusion with prelesional edema (B).
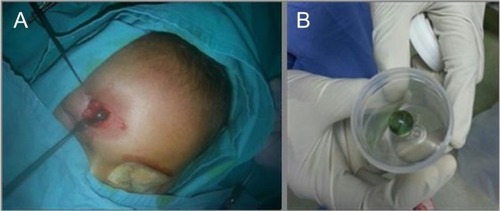
On the following day, the infant underwent a wound debridement, foreign body removal and suturing under general anesthesia. The operation was performed and comanaged by the Plastic Surgery and Neurosurgery teams. A 0.5 cm diameter marble was discovered, which remained unshattered, embedded in the left frontal bone (). The left frontal bone surrounding the marble was fractured into small, multiple pieces. The marble and bone fragments were removed. With help from the Plastic Surgery team, we were able to reconstruct the wound, and the wound was closed with interrupted sutures.
Figure 4 Wound exploration revealed a marble embedded in the left frontal bone (A) which is unshattered (B).
The skin covering the circular laceration wound was well-apposed at day 2 postsuturing (). At 1 week, after completing intravenous ceftriaxone, the left eye preseptal cellulitis was improved, with resolving eyelid swelling and conjunctival chemosis. The patient was discharged with a topical eye drop combination of betamethasone sodium phosphate and gentamicin sulfate, every 8 hours, for the left eye.
Figure 5 The skin covering the circular laceration wound was well-apposed at day 2 postsuturing.

At follow-up at 2 weeks, the left forehead wound was well apposed. The left eye swelling and conjunctival chemosis were completely resolved. Topical antibiotic was discontinued, and the infant was given 6 months of follow-up for cyclorefraction.
Discussion
Noncongenital unilateral visual disability and blindness following ocular trauma is a leading ophthalmic morbidity among the pediatric age group.Citation2 A study conducted in America showed that pediatric eye injuries are a common presentation to the emergency department.Citation3
There are various pediatric eye injuries that have been reported, involving the use of different devices and various presentations of eye injury. The vision- and life - threatening injuries inflicted by other devices besides sling shots are stone, stick, wire, bottle, belt buckle, knife, fist, nail, toy guns, sword fighting, and water balloon.Citation4–Citation7 Podbielski et al mentioned that ocular injuries are the most common type of injury that occurs when children are playing.Citation6 The types of common ocular injuries among children that have been reported are contusion, open globe, lid laceration, foreign body in orbit or ocular adnexa, corneal abrasion or rupture, and burns.Citation4,Citation6,Citation7 Bacterial infection at the break in the skin following trauma to the eyelid can lead to preseptal cellulitis.Citation8
Preseptal cellulitis is potentially a severe infection of the ocular adnexa in the pediatric age group.Citation9 Improper treatment of preseptal cellulitis may progress to orbital cellulitis and worsen the condition. Complications, such as subperiosteal abscess, orbital abscess, cavernous sinus thrombosis, intracranial infections, and loss of vision, may occur and could lead to death.Citation8 It is extremely important to promptly recognize and diagnose the condition and treat accordingly in order to save the child’s vision and life. Our patient developed left eye preseptal cellulitis as a complication from the break in the skin at the frontal region, just above his left eyebrow, following the sling shot injury.
Mowatt et al reported that ocular injury involving the pediatric age group can be age-specific, with males being predominant compared with females.Citation4 Injuries occurring at home are more frequent compared with those at school, which is where maximum number of hours is spent playing.Citation4,Citation5,Citation10 There are several factors that are linked to the risk of unintentional injury among siblings, like family characteristics, behavioral problems, temperament, and stressful life events, and it is also associated with sociodemographic traits.Citation11 Poor supervision at home could also be a contributing factor.Citation4,Citation5,Citation10
Most of the injuries involving the pediatric age group are preventable if there is proper and close adult supervision, good safety measures, barrier methods to prevent toddler access to hazards at home, and education of children in schools regarding the hazards associated with playing with firecrackers, catapults, and stones. Using toys inappropriate for age and underdeveloped motor skills predisposes the younger age group to injuries.Citation12 Parents should play a role in allowing only age-appropriate, recommended toysCitation13 to their children. Media, such as videos, brochures, newsletters, radio, television, and the mail, deliver information and may play a role in parental education about and awareness of injury prevention. Such material, for instance, may educate the parents to modify the physical space to control access to hazards; prevent the child from reaching the top of the stove by installing a safety device; while cooking, use the back burners or turn the pot handles around; and cover all the sharp edges of furniture with rubber material.Citation1
In summary, ocular traumas are devastating in children and can lead to lifelong suffering and disability.Citation14 Pediatric ocular injury, not only affects the cost of care for parents but also, consumes time away from school and parents’ time from work (related to time needed for subsequent follow-up visits at the clinic). The quality of life in a young child with serious ocular trauma and subsequent loss of vision will be definitely impaired, as the injury imposes a lifelong burden.Citation15 If the child has a blinding outcome, this would affect him physically, psychologically, and psychosocially, and would also affect the choice of profession and level of integration into society in future.Citation4 Prevention is better than cure, and this can be achieved by education and encouraging parental or adult supervision, and by putting a stop to access to sharp and dangerous toys or objects, thus decreasing the occurrence of childhood ocular injuries.
Disclosure
The authors report no conflicts of interest in this work.
References
- MorrongielloBAOndejkoLLittlejohnAUnderstanding toddlers’ in-home injuries: I. Context, correlates, and determinantsJ Pediatr Psychol200429641543115277585
- MayDRKuhnFPMorrisREThe epidemiology of serious eye injuries from the United States Eye Injury RegistryGraefes Arch Clin Exp Ophthalmol2000238215315710766285
- WongTYTielschJMEpidemiology of ocular traumaTasmanWJaegerEADuane’s Ophthalmology5 Available from: http://www.eyecalcs.com/DWAN/pages/v5/v5c056.htmlAccessed January 16, 2015
- MowattLMcDonaldAFerron-BootheDPaediatric ocular trauma admissions to the University Hospital of the West Indies 2000–2005West Indian Med J201261659860423441354
- BabarTFJanSGulLTariqMKhanMYZamanMDPattern of paediatric ocular trauma in Hayatabad Medical Complex, PeshawarPak J Med Res20064569 Available from: http://www.pmrc.org.pk/pediatric-ocular.htm. Accessed January 16, 2015..
- PodbielskiDWSurkontMTehraniNNRatnapalanSRatnapalanSRPediatric eye injuries in a Canadian emergency departmentCan J Ophthalmol200944551952219789585
- BullockJDJohnsonDABallalDRBullockRJOcular and orbital trauma from water balloon slingshots. A clinical, epidemiologic, and experimental studyOphthalmology199710458788879160038
- ClarkeWNPeriorbital and orbital cellulitis in childrenPaediatr Child Health20049747147219657411
- DevrimIKanraGKaraAPreseptal and orbital cellulitis: 15-year experience with sulbactam ampicillin treatmentTurk J Pediatr200850321421818773664
- AritürkNSahinMOgeIErkanDSüllüYThe evaluation of ocular trauma in children between ages 0–12Turk J Pediatr1999411435210770675
- RodriguezJGChildhood injuries in the United StatesAm J Dis Child199014466276462189296
- PoonASNgJSLamDSFanDSLeungATEpidemiology of severe childhood eye injuries that required hospitalisationHong Kong Med J19984437137411830699
- MacEwenCJBainesPSDesaiPEye injuries in children: the current pictureBr J Ophthalmol199983893393610413696
- HosseiniHMasoumpourMKeshavarz-FazlFRazeghinejadMRSaloutiRNowroozzadehMHClinical and epidemiologic characteristics of severe childhood ocular injuries in southern IranMiddle East Afr J Ophthalmol201118213614021731324
- CoolingRJThe burden of serious ocular injuryBr J Ophthalmol19968075858795366