
Abstract
Purpose
To demonstrate the successful clinical identification and management of rhino-orbital mucormycosis, a fungal infection with a high mortality rate.
Patients and methods
A diabetic male patient with a headache and orbital apex syndrome in the right eye was examined using computed tomography (CT) and magnetic resonance imaging (MRI) for a possible fungal infection. Endoscopic surgical resection was performed and a pathology sample was taken. Specimens were prepared with Gömöri methenamine silver and hematoxylin and eosin staining. The patient was treated with liposomal amphotericin B 400 mg daily, followed by posaconazole 400 mg twice daily.
Results
CT and MRI revealed a mass of the right sphenoid spreading into the orbit, indicative of a fungal infection. The biopsy confirmed the diagnosis of mucormycosis. Complete recovery of eyelid and oculomotor function was achieved after 10 months of treatment, although the patient continues to suffer from irreversible blindness in the right eye due to optic nerve atrophy. He has been without signs or symptoms of recurrence.
Conclusion
Patients with rhino-orbito-cerebral mucormycosis need extensive surgical and medical treatment to maximize outcomes. Success requires multidisciplinary management.
Introduction
Orbital apex syndrome (OAS) is an uncommon clinical presentation consisting of complete ophthalmoplegia with vision loss, involving cranial nerves II, III, IV, V1, and VI.Citation1 OAS may result from trauma, malignancy, infection, inflammation, or vascular origins. Some of these conditions, particularly among the infectious causes, can be life-threatening with delayed diagnosis and treatment. Rhino-orbito-cerebral mucormycosis (ROCM) is an invasive and often fatal fungal infection. The incidence of mucormycosis is increasing,Citation2,Citation3 with a current estimate of 1.7/1,000,000 cases in the US annually.Citation4 In the emergent setting, any patient with OAS who is either immune compromised or diabetic should be evaluated for the presence of mucormycosis. We present a case of a successfully treated diabetic patient with OAS resulting from rhino-orbital mucormycosis who presented to the emergency department for treatment of headache symptoms.
Case report
A 68-year-old Hispanic male presented to the Emergency Department for severe headache, dizziness, and nausea. He had a past history of prostate cancer with 48 days of ongoing radiotherapy, and an acoustic neuroma that was treated with gamma knife surgery 3 years prior to this presentation. Current medical history revealed poorly diet-controlled type 2 diabetes. He was noted to have significantly decreased ocular motility and loss of vision in his right eye. Ophthalmologic examination revealed no light perception and ophthalmoplegia in the right eye () with impairment of cranial nerves II, III, IV, V1, and VI, culminating in a diagnosis of OAS. Funduscopic examination showed no significant abnormalities.
Figure 1 External examination of extraocular eye movements.

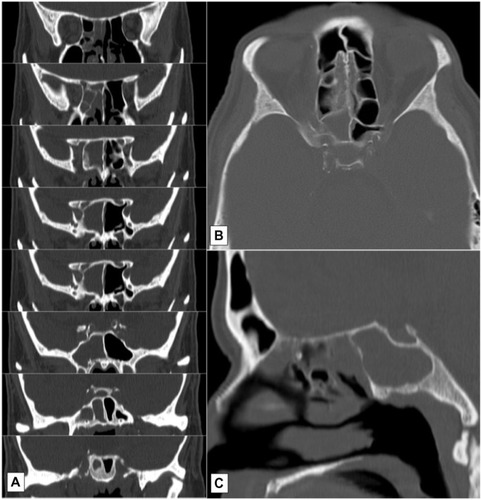
A computed tomography (CT) scan of the brain showed bilateral opacification of the ethmoids, near complete opacification of the right sphenoid, and mild mucosal thickening in the left sphenoid and maxillary sinuses (). Hyperintense T2 signals of the right sphenoid sinus shown on MRI suggested the presence of fungal involvement. ENT evaluated the patient and concurred with the possible diagnosis of mucormycosis.
Figure 2 CT scan of the brain, without contrast.
Abbreviation: CT, computed tomography.
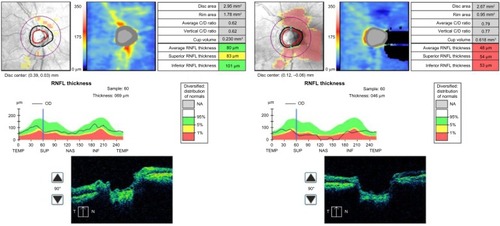
Endoscopic surgical resection was performed by ENT, and a pathology sample was taken. Histopathology of tissue stains showed positivity for mucormycosis (). The patient subsequently underwent aggressive endoscopic removal of the involved tissue. The patient was treated with liposomal amphotericin B 400 mg, IV, postsurgery. After 3 weeks, he experienced some minor nephrotoxicity as a side effect of the liposomal amphotericin B, and was switched to posaconazole 400 mg twice daily for 2 months. After 10 months, there was complete resolution of ophthalmoplegia, although there was evidence of presynaptic atrophy of the right optic nerve ().
Figure 3 Histopathology slides.
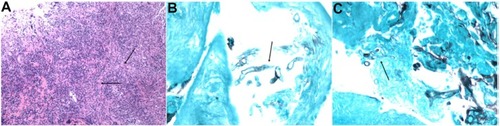
Figure 4 Optical coherence tomography.
Abbreviations: RNFL, retinal nerve fiber layer; C/D, cup to disc; T/TEMP, temporal; SUP, superior; N/NAS, nasal; INF, inferior; HD, high definition; OD, right eye; NA, not available.
Written informed consent was obtained from the patient to allow the publication of photographs for educational purposes. This study adhered to the tenets of the Declaration of Helsinki and was Health Insurance Portability and Accountability Act (HIPAA) compliant. Dignity Health Institutional Review Committee ruled that approval was not required for this study.
Discussion
OAS is a common presentation of ROCM, but unfortunately blindness is permanent and the risk of mortality is increased at this stage of progression. Mucormycosis is the third most frequent fungal disease after candidiasis and aspergillosis,Citation3 and is more likely to cause OAS.Citation5 Prime susceptibility factors for ROCM include diabetes mellitus, ketoacidosis, immunosuppression, and elevated levels of serum iron.Citation5,Citation6 Elevated blood glucose levels and change in acidity levels nourish fungal colonies, and increased availability of unbound serum iron in acidotic conditions aids in the growth of fungus and development of vascular invasion.Citation7 Angioinvasion with thrombus and further tissue necrosis is the most likely mechanism of the sinus disease spreading into the orbit and brain.
Mucormycosis can be difficult to identify if indicators such as thrombosis and necrotic tissue are absent or are late in presentation. Thurtell et alCitation5 reported 14 patients with biopsy proven ROCM and OAS, with only one patient being correctly diagnosed at presentation. In diabetics, OAS secondary to ROCM may initially present as a sixth nerve palsy or partial ophthalmoplegia and is felt to represent microvascular disease, particularly when there is minimal disease sinus findings by CT.Citation8 When any sinus disease with OAS is observed in a diabetic or immunocompromised patient by CT or MRI, a fungal etiology should be suspected. MRI is an effective technique in diagnosing OAS, with biopsy being the most reliable.
Mucormycosis is a highly aggressive infection known to have a high mortality rate when not treated. Survival rates depend on the interval period from appearance of symptoms to onset of treatment or surgery, extent and location of the infection, type of treatment, and amount of immunosuppression. Roden et alCitation2 published a review of infectious patterns and outcomes of 929 patients with zygomycosis between 1885 and 2005. The most common sites of infection were sinus (39%), pulmonary (24%), and cutaneous (19%). Of the sinus infections, 21% of patients had rhinocerebral involvement, 8% had sino-orbital involvement, and 8% had sinusitis. Of these, the mortality rates were 62%, 24%, and 16%, respectively. Orbital involvement is unilateral,Citation9 and the survival rate decreases dramatically with bilateral sinus involvement.Citation6
Amphotericin B has been the antifungal of choice since the first successful treatment of this disease by Gass in 1961.Citation6,Citation10 Liposomal amphotericin B has similar or better survival rates than amphotericin B with less nephrotoxicity.Citation4,Citation6,Citation9 However, in this case the patient still developed mild nephrotoxicity and was switched to posaconazole. Posaconazole is useful as a secondary treatment when kidney function is affected, and is more effective against Mucorales in vitro than other triazoles.Citation4,Citation9 Optimal therapy requires a multidisciplinary approach between internists and ENT, ophthalmology, and infectious disease specialists.
Disclosure
The authors report no conflicts of interest in this work.
References
- AndersUMTaylorEJMartelJRMartelJBPseudo-orbital apex syndrome in the acute trauma setting due to ipsilateral dissection of internal carotid arteryOphthal Plast Reconstr Surg Epub9112014
- RodenMMZaoutisTEBuchananWLEpidemiology and outcome of zygomycosis: a review of 929 reported casesClin Infect Dis200541563465316080086
- Di CarloPPirrelloRGuadagninoGMultimodal surgical and medical treatment for extensive rhinocerebral mucormycosis in an elderly diabetic patient: a case report and literature reviewCase Rep Med2014201452706224982678
- GamaletsouMNSipsasNVRoilidesEWalshTJRhino-orbital-cerebral mucormycosisCurr Infect Dis Rep201214442343422684277
- ThurtellMJChiuALGooldLANeuro-ophthalmology of invasive fungal sinusitis: 14 consecutive patients and a review of the literatureClin Exp Ophthalmol2013416567576
- YohaiRABullockJDAzizAAMarkertRJSurvival factors in rhino-orbital-cerebral mucormycosisSurv Ophthalmol19943913227974189
- SravaniTUppinSGUppinMSSundaramCRhinocerebral mucormycosis: pathology revisited with emphasis on perineural spreadNeurol India201462438338625237943
- BalchKPhilipsHPNewmanNJPainless orbital apex syndrome from mucormycosisJ Neuroophthalmol19971731781829304530
- ToumiALarbi AmmariFLoussaiefCRhino-orbito-cerebral mucormycosis: five casesMed Mal Infect2012421259159823116703
- SponslerTASassaniJWJohnsonLNTowfighiJOcular invasion in mucormycosisSurv Ophthalmol19923653453501566236