
Abstract
A 31-year-old man presented to our clinic for an ocular trauma to his left eye. His best-corrected visual acuity was 20/200 OS (left eye). Anterior segment examination showed an epithelial defect, which implies a direct injury to the cornea. A marked focal stromal edema accompanied by Descemet’s membrane folds were located at 10 o’clock in the paraxial area, about 4 mm apart from the corneal center. Anterior segment optical coherence tomography (AS-OCT) revealed marked corneal swelling of the lesion. Five days later, the patient’s best-corrected visual acuity improved to 20/50 OS. The stromal edema resolved showing no signs of epithelial defect, although small opacity remained. AS-OCT revealed complete resolution of corneal swelling. Despite the resolution of corneal edema, however, specular microscopy showed substantially decreased endothelial cell density in the lesion compared to the fellow eye. Here we report a case of traumatic corneal stromal edema discovered by AS-OCT.
Keywords:
Introduction
Ocular trauma, although relatively rare, is a proven etiology of focal corneal stromal edema. A notable example of corneal edema caused by trauma is traumatic corneal endothelial rings. Not many cases have been reported since it was described in 1978 by Cibis et al.Citation1 Ocular manifestations include lesions of transient, gray-white, endothelial ring-shaped opacities with focal corneal stromal edema and most cases show remission within a few days with conservative management.Citation2 Here we report a case of traumatic corneal stromal edema discovered by anterior segment optical coherence tomography (AS-OCT).
Case report
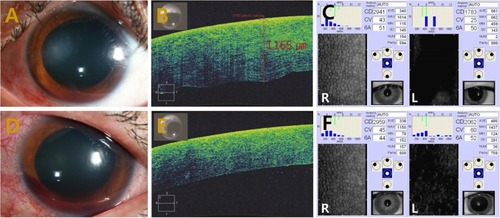
A 31-year-old man presented to our clinic for an ocular trauma to his left eye. The patient had a blast injury which occurred on the previous day by a plastic bottle cap when trying to open a beverage bottle. Past medical history was unremarkable. His best-corrected visual acuity (BCVA) was 20/200 OS (left eye). Anterior segment examination showed an epithelial defect, which implies a direct injury to the cornea. A marked focal stromal edema accompanied by Descemet’s membrane folds were located at 10 o’clock in the paraxial area, about 4 mm apart from the corneal center (). Grade 1 gross hyphema was observed. AS-OCT (AS-OCT; Carl Zeiss Meditec AG, Jena, Germany) revealed marked corneal swelling of the lesion (). Endothelial cell density was 1783 cells/mm2 (). Funduscopic examination showed clear vitreous with normal optic disc and retina. The patient was given topical cycloplegics and 1% prednisolone acetate every 2 hours. Five days later, his BCVA improved to 20/50 OS. The stromal edema resolved, showing no signs of epithelial defect, although small opacity remained (). AS-OCT revealed complete resolution of corneal swelling (). Despite the resolution of corneal edema, however, specular microscopy (SP-9000; Konan Medical, Tokyo, Japan) showed substantially decreased endothelial cell density in the lesion compared to the fellow eye (2,062 versus 2,959 mm2) (). The patient’s condition was observed while tapering the topical steroid. One month later, the patient’s 2959 cells/mm2 BCVA improved to 20/25 OS. There were no signs of corneal edema and no further decrease in endothelial cell density.
Figure 1 Marked focal corneal edema → marked focal stromal edema.
Discussion
A diffuse corneal edema and its recovery is often observed in patients with eye injury caused by ocular trauma. The main etiologies of transient diffuse stromal edema include post-traumatic inflammation inside the anterior chamber and persistently increased intraocular pressure. However, a local corneal edema accompanied by substantially decreased endothelial cell is a rare and notable case. This case differs from traumatic corneal endothelial rings in that there is no distinct endothelial ring lesion on slit lamp examination. Furthermore, despite the difference in corneal morphology, this case shares a similarity with the traumatic corneal endothelial rings: the corneal lesion was caused by traumatic endothelial cell damage in this case. To our knowledge, only one case of traumatic corneal endothelial rings with imaging of AS-OCT has been reported,Citation3 in which the AS-OCT revealed a ruffled disruption to the endothelial cells directly posterior to the stromal thickening. We too discovered a similar ruffled endothelial disruption from imaging (). Endothelial cells around the traumatic lesion undergo the greatest torsion and energy absorption as the cornea moves axially posterior and then relaxes to its original position.Citation4 This process could have induced the damage and inflammation of the corneal endothelial cells. Another possible mechanism that caused the injury would be a direct contact between the corneal endothelium and a lens or iris. Dysfunction of damaged endothelial cells are replaced with circumferential normal endothelial cells. The proper functioning of the corneal endothelium is regarded to be crucial to the maintenance of corneal clarity. Once damaged, the endothelium is not able to recover from the injury. Therefore, significant endothelial damage may lead to severe complications such as persistent corneal edema and bullous keratopathy at a later stage.
Conclusion
In conclusion, permanent corneal endothelial cell loss could occurs by traumatic mechanism, which manifests as corneal stromal edema in the early phase of trauma. Corneal endothelial layer evaluation using specular microscopy and AS-OCT can be useful for diagnosing and monitoring the damage to cornea.
Disclosure
The authors report no conflicts of interest in this work.
References
- CibisGWWeingeistTAKrachmerJHTraumatic corneal endothelial ringsArch Ophthalmol1978963485488415710
- NgSKRudkinAKGalanopoulosATraumatic corneal endothelial rings from homemade explosivesInt Ophthalmol201333439539723474743
- ReidGAMusaFOCT Imaging of a Traumatic Endothelial RingCornea201433995295425014155
- MaloneyWFColvardMBourneWMGardonRSpecular microscopy of traumatic posterior annular keratopathyArch Ophthalmol197997916471650475633