
Abstract
Objective
Acute appendicitis and incarcerated hernia rarely present in the same episode. Our study reports patient presentation, diagnosis method, and treatment of an unusual case at the Chiang Mai University Hospital.
Method
Case report.
Result
A 20-year-old man visited the Chiang Mai University Hospital with right lower quadrant pain and a right groin mass which could not be reduced. The computerized tomography scan showed acute appendicitis and omentum in the hernia sac. Operative treatment was an appendectomy and herniorrhaphy. The treatment was successful, and the patient was discharged from our hospital without any complications.
Conclusion
Concurrent acute appendicitis and incarcerated hernia are very rare, but should be kept in mind if a patient presents with right lower quadrant pain and a right groin mass. Further investigation may be helpful if the diagnosis is uncertain. Operative priority treatment depends on each individual case.
Introduction
Acute appendicitis is an inflammation of the vermiform appendix, one of the most common causes of an acute abdomen and most frequent indications for an emergent abdominal surgical operation. The inflammatory process in the appendix presents as pain, which initially is of a diffuse visceral type, and later becomes localized, shifting to peritoneal irritation of the right lower quadrant.
Incarcerated hernia occurs when the hernia contents cannot be reduced, and urgent or emergent hernia repair should be undertaken to reduce the risk of strangulation.
The combination of the two conditions in one patient is rare. After reviewing the literature and other case reports, no case report similar to that of this patient was found, except some studies that reported Amyand’s hernia (inflamed or normal appendix in the sac of inguinal hernia)Citation1–Citation4 and incarcerated appendix within the femoral hernia.Citation5–Citation7 With no epidemiological data for acute appendicitis and incarcerated inguinal hernia in Thailand, we calculated the probability of the two conditions occurring together at approximately nine per 1,000,000 patients, based on studies of Lee et alCitation8 and van den Heuvel et al.Citation9
Case report
A 20-year-old man visited our hospital due to periumbilical pain lasting approximately 20 hours, followed by localized pain in the right lower quadrant for 6 hours with nausea and vomiting. The patient had a history of underlying pectus excavatum which had been corrected by Nuss procedure (minimally invasive repair of the pectus excavatum) and a right inguinal mass that reduced 4 years ago, although the patient never visited a hospital for this latter condition. At the outpatient department, the patient presented with a right groin mass that could not be reduced. Vital signs included an oral temperature of 37.7°C, a regular pulse of 113 beats per minute, blood pressure of 180/100 mmHg, and a respiratory rate of 18 breaths per minute. Physical examination revealed, marked tenderness and voluntary guarding at the right lower quadrant with a right inguinal mass, 7×10 cm, extending to the scrotal sac with no skin redness, and mild tenderness at the groin mass which was irreducible. Both testes were normal.
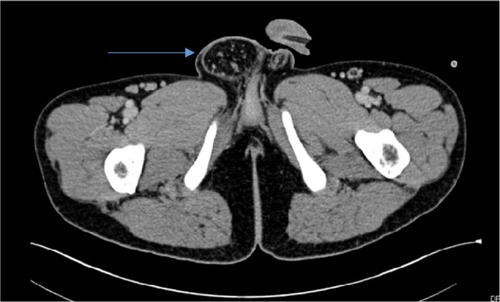
Because diagnosing these two diseases at the same time was uncommon, we requested an abdominal computerized tomography (CT) scan to confirm the diagnosis. The CT scan reported circumferential enhancing wall thickening and dilated fluid-filled appendix, 1.5 cm in maximal diameter () and a herniation sac containing omental fat through the right inguinal canal, compatible with indirect inguinal hernia with no evidence of bowel obstruction ().
Figure 1 Dilated appendix, size 1.5 cm in maximal diameter (arrow).

Figure 2 Computerized tomography scan showing hernia extending through the scrotal sac (arrow).
After the CT scan, the patient was prepared for surgery with hydration and intravenous antibiotics (2 g of ceftriaxone and 500 mg of metronidazole). Intraoperatively, the patient was in a supine position under general anesthesia.
The first procedure was an appendectomy, utilizing the Lanz skin incision; the external oblique aponeurosis was divided, followed by the muscle split technique, entering the peritoneum into the abdominal cavity. We found an acute gangrenous-type appendix, a divided and ligated mesoappendix, and the appendiceal artery was ligated with silk No. 5–0. Appendectomy was done by the double ligation technique, with silk No 0.
After finishing the appendectomy, we tried to reduce the omentum, that is the content of the incarcerated hernia, from the hernia sac, but we were unsuccessful. Before starting the second procedure, all drapes were changed and a sterile scrub was repeated. An incision to repair the hernia was separated by a transverse skin incision at the right inguinal area (), two-finger breadth above the inguinal ligament, then the external oblique aponeurosis was divided and identified, and the iliohypogastric and ilioinguinal nerves were preserved. The spermatic cord was encircled to isolate it from the posterior wall of the inguinal canal with a penrose drain, after which we opened the hernia sac. The content of the hernia was omentum, without intestine; a partial omentectomy was performed, due to adhesions in the hernia sac. The remaining omentum was reduced into the abdominal cavity. A herniotomy was performed by the purse-string technique with atraumatic silk 2-0. The inguinal floor was repaired by “Bassini” technique and the skin was closed with nylon 3/0 vertical mattress.
Figure 3 Surgical incisions.

The total operative time was 2.5 hours, with minimal blood loss (appendectomy 1 hour and incarcerated hernia operation 1.5 hours). The pathology report confirmed acute necrotizing appendicitis. The patient was discharged without any complications on postoperative day 7. The Research Ethics Committee of Chiang Mai University approved the study. Written, informed consent was obtained from the patient.
Discussion
Acute appendicitis and incarcerated hernia are two of the most common acute abdominal conditions requiring surgical intervention. Although common individually, these conditions are very rare concurrently – we could not find any case report of their simultaneous presentation in the literature. Our patient, in contrast, presented with both conditions simultaneously. A review article of Meinke about appendicitis in groin herniasCitation7 reported 45 cases of hernial appendix (appendicitis in hernial sac), that were clinically similar to incarcerated hernia and typical of clinical acute appendicitis. However, the patients in the review article presented with acute appendicitis in the abdominal cavity, rather than the hernia sac like our patient, and the review article did not discuss surgical procedures.
Given the rarity of our case, we have reported this patient’s case history here. From history taking and physical examination of this patient, we were uncertain of the diagnosis, particularly given the rarity of the concurrent symptoms, so we requested a CT scan for definite diagnosis. From the CT scan result, we diagnosed acute appendicitis and incarcerated indirect inguinal hernia. Incarcerated hernia may be precipitated condition by acute appendicitis explained from abdominal pain, which increases intra-abdominal pain caused by acute appendicitis. To reduce the risk of perforation, we performed the appendectomy first, particularly given the CT scan showed that the hernia was less urgent due to the omentum content of the sac. Since intraoperative, acute gangrenous appendicitis was found during the appendectomy, all drapes and surgical instruments were changed before repairing the hernia. A separate incision was performed at the right groin region; finding omentum in the sac confirmed the imaging from the CT scan. A partial omentectomy was performed due to adhesions, followed by a reduction of the mass into the abdominal cavity and herniorrhaphy with “Bassini” technique. The total operative time was 2.5 hours, with minimal blood loss.
Some surgeons in our department had suggested that the herniorrhaphy should be performed first, because they were concerned about wound contamination. They recommended that a clean wound in a herniorrhaphy should be followed by the clean contaminated wound in an appendectomy to avoid the risk of surgical site infection. The final discussion regarding the order of the procedures was that the priority of the operation depended on the individual case.
Disclosure
The authors report no conflicts of interest in this work.
References
- AliTICase report: Amyand’s hernia (incarcerated right congenital indirect inguinal hernia due to inflamed appendix)Int J Collab Res Intern Med Public Health201245478484
- BannisterSLWongALLeungAKCAcute appendicitis in an incarcerated inguinal herniaJ Natl Med Assoc2001931248748911800278
- Hrushets’kyǐMMKurtashLASkoropadTIPelekhanOIAcute gangrenous-perforative appendicitis simulating incarcerated inguinal herniaKlin Khir2006106417269414
- KouskosEKomaitisSKouskouMDespotellisMSanidasGComplicated acute appendicitis within a right inguinal hernia sac (Amyand’s hernia): report of a caseHippokratia2014181747625125958
- SaylamBGülserenMOŞimşekBCoşkunFIncarcerated appendix within femoral herniaFormos J Surg2014476231232
- TancrediABellagambaRCotugnoMDe Garengeot’s hernia: a diagnostic challengeIndian J Surg201577214714926139970
- MeinkeAKReview article: appendicitis in groin herniasJ Gastrointest Surg200711101368137217394046
- LeeJHParkYSChoiJSThe epidemiology of appendicitis and appendectomy in South Korea: national registry dataJ Epidemiol20102029710520023368
- van den HeuvelBDwarsBJKlassenDRBonjerHJIs surgical repair of an asymptomatic groin hernia appropriate? A reviewHernia201115325125921298308