
Abstract
Purpose
We describe a case of full-thickness corneal restoration after an acute corneal burn with an acid agent.
Methods
A 32-year-old male reported painful discomfort, redness, photophobia, and a decrease in visual acuity in the left eye after a unilateral burn with an acid agent. Slit-lamp examination revealed massive corneal melting involving necrotic sequestrum of the entire corneal surface. Surgical approach was carried out in order to preserve residual ocular tissues.
Results
Extensive corneal–conjunctival layer curettage of the necrotic tissue was performed showing perfectly clear undamaged deep lamellar corneal layers. The patient underwent multilayered amniotic membrane transplantation and total capsular–conjunctival flap in order to preserve ocular tissue from further melting or corneal perforation. A complete and spontaneous “restitutio ad integrum” of the corneal layers was shown during the follow-up. The cornea was perfectly clear with restored normal anatomical architecture.
Conclusion
In this case, a spontaneous full-thickness corneal tissue restoration occurred after an acute chemical burn. Studies about the mechanisms whereby different cells interact and replicate within the stroma may unveil the biology behind corneal regeneration and transparency.
Introduction
Ocular burns constitute true ocular emergencies, and both thermal and chemical burns represent potentially blinding ocular injuries. Recovery of ocular surface burns depends upon the causative agent and the extent of damage to corneal, limbal, and conjunctival tissues at the time of injury.Citation1 Developments in the management of ocular surface burns, such as amniotic membrane transplantation (AMT), have been used in the treatment of several ophthalmic disorders and conditions.Citation2 However, even amniotic membrane (AM) grafts, which work largely by providing a substrate for epithelial cells to grow on, fail when there are no surviving epithelial, conjunctival, or limbal cells. In this article, we report an unusual case of full-thickness corneal regeneration in a patient with an acute acid burn. This report adhered to the tenets of the Declaration of Helsinki.
Case report
A 32-year-old male reported painful discomfort, redness, photophobia, and a decrease in visual acuity in the left eye after a unilateral burn with ammonium defluoridate and sulfuric acid. The patient was referred to the Cornea Service of San Paolo Ophthalmic Center (San Antonio Hospital, Padova, Italy). The patient was initially treated with irrigation of saline to normalize the ocular surface pH, and for removal of remaining particulate matter, prophylactic topical antibiotics, lubricants, steroids, and cycloplegics were used. Three days after primary accident, slit-lamp examination revealed massive corneal involvement with an extensive necrotic/degenerative corneoconjunctival tissue covering the entire surface and obscuring both the iris details and anterior chamber. The entire limbus and conjunctiva were involved (). No Seidel’s phenomenon was shown on slit-lamp examination.
Figure 1 Ocular surface before and after necrotic tissue excision.
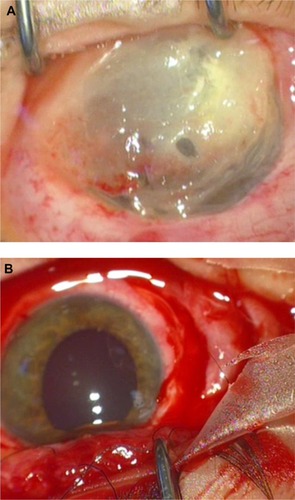
After an informed written consent was obtained, the patient underwent accurate surgical debridement (). The necrotic corneoconjunctival tissue was excised from the entire corneal surface under surgical microscopy. During this procedure, a clear and perfect corneal tissue was shown (∼90% of corneal stroma was removed by curettage, leaving Descemet’s membrane clearly seen in the central area; ). Multilayered AMT was performed in order to preserve the exposed corneal tissues and to stimulate both reepithelialization and regeneration of the corneal architecture. A sutureless AM was arranged in multiple layers so that the entire ocular surface was covered, as well as the peripheral corneal–limbal surface. AM patch was then covered by a full-thickness conjunctival flap, including Tenon’s capsule.Citation3 The rationale of this procedure was to control corneal inflammation and pain, as well as to ensure protection and healing efficacy. Penetrating keratoplasty was considered either as a surgical procedure at the time of flap removal or as a separate event in an eye with visual potential.
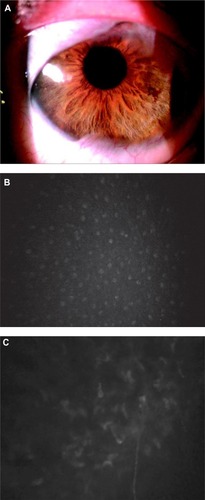
Postoperative treatment consisted of topical eyedrops (dexamethasone 0.15% and ofloxacin 0.3%) four times daily. Steroids were slowly tapered, while topical antibiotics were discontinued after a 4-week follow up period. AM flap retraction occurred spontaneously, leaving the ocular surface free during the follow-up (4–5 months). The cornea appeared clear and 90%–100% corneal stromal thickness was regained (). Optical coherence tomography showed a central corneal thickness of 508 µm measured at the apex of the corneal surface. To evaluate the changes in cell morphology in regenerated tissues, corneal epithelium was evaluated from the central area of regenerated cornea using confocal microscopy (). The flattened surface and smaller basal epithelial cells were normal in morphology and layer numbers also. Corneal nerve bundles regenerated in the corneal stroma. Anterior keratocytes and stroma were unevenly distributed, with bright nuclei and signs of opacity (). Best-corrected visual acuity was 20/40 OS.
Figure 2 Postoperative evaluation by means of slit-lamp and corneal confocal microscopy.
The cornea remained transparent with complete clearing over the 12-month follow-up period. A residual peripheral vascularized corneal pannus diffusion in three quadrants of the cornea, without involvement of the optic axis, was shown. There was a complete reepithelialization with no neovascularization or other ocular surface abnormality. A residual symblepharon confined to the upper fornix was also observed.
Ethical approval
A detailed explanation of the treatment was given to the patient, and informed written consent was obtained before any procedure. This protocol was approved by the institutional review board of the San Paolo Ophthalmic Center, San Antonio Hospital.
Discussion
Recovery of ocular surface burns depends upon the causative agent and the extent of damage to corneal, limbal, and conjunctival tissues at the time of injury.Citation1 Several procedures would be considered in order to manage such an event. Procedures including AMT, autolimbal transplantation, and allolimbal transplantation have been reported in several studies.Citation2,Citation4,Citation5 Some of these describe a partial and/or complete recovery of the stroma in patients who underwent AMT for corneal perforation and point out that AMT might influence the proliferation and migration of neighboring keratocytes, leading to stromal substance synthesis.Citation4,Citation5 AM undergoes subsequent progressive modification after integration because of the biological interactions that influence tissue healing and scar formation with incomplete clearing of the residual tissue, although a partial recovery of the AM tissue transparency, once integrated, is achieved. This limits any optical or visual benefits of stromal restoration.
We describe an unusual and complete restoration of the entire stromal thickness without reflectivity reduction in a patient exposed to acute burns caused by acid agents. We do not have a complete explanation to such a phenomenon. We hypothesize a remodeling of the stroma with new collagen formation and repopulating with corneal stroma-derived cells, fibroblasts, and myofibroblasts that layered down new collagen. Unknown trophic and regenerative factors might have induced mitotic effects on quiescent corneal keratocytes, which first underwent replication and then secreted normal corneal stroma components, including keratin sulfate and collagens (essential to build up new corneal stroma in a patient where only the Descemet’s membrane was preserved). Because it is a well-established fact that corneal stroma has minimal or no regenerative properties (sporadic corneal stroma in human restoration is anecdotal), the observation that, in some animal models, the cornea can regenerate does have scientific significance.Citation6 Indeed, we cannot also exclude the potential of human keratocytes to repopulate stromal tissue without scarring.Citation7 Keratocytes might not conform to the classic definition of terminal differentiation, and at least some cells in the stroma may respond and regenerate transparent corneal tissue.Citation7
Our report has several limitations. First, we were not able to demonstrate that some healthy residual corneal tissues were spared during chemical burning. Second, we were also unable to obtain complete corneal tissue thickness measurements before surgery. Given the severity of the original injury, it seems also surprising that limbal stem cell deficiency did not occur. It is hard to imagine how the limbus escaped significant injury, while the whole thickness of the stroma was destroyed. Both transient and limited limbal ischemia occurred soon after the injury but recovered in the ensuing days.Citation1 Surviving limbal stem cells are capable to recover, multiply, and repopulate the area. Whether multiple layers of amnion transplantation in combination with the conjunctival flap might be able to provide a scaffold for the formation of corneal stroma, or for migration and repopulation with derived keratocytes, cannot be determined at this stage.
Conclusion
This case report describes an unusual event, in which a full-thickness regeneration occurred after extensive corneal burning. Any evidence of the hypothesized regenerative properties of human corneal stroma during corneal wound healing would have vast and impressive implications and justifies future studies.
Author contributions
All authors contributed toward design and conduct of the study, collection, management, analysis, and interpretation of data, preparation, drafting, review, and revision of the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
- DuaHSKingAJJosephAA new classification of ocular surface burnsBr J Ophthalmol2001851379138311673310
- HanadaKShimazakiJShimmuraSTsubotaKMultilayered amniotic membrane transplantation for severe ulceration of the cornea and scleraAm J Ophthalmol200113132433111239864
- GundersenTPearlsonHRConjunctival flaps for corneal disease: their usefulness and complicationsTrans Am Ophthalmol Soc19696778955381310
- KenyonKRTsengSCLimbal autograft transplantation for ocular surface disordersOphthalmology1989967097232748125
- TsubotaKTodaISaitoHShinozakiNShimazakiJReconstruction of the corneal epithelium by limbal allograft transplantation for severe ocular surface disordersOphthalmology1995102148614969097796
- PinnamaneniNFunderburghJLConcise review: stem cells in the corneal stromaStem Cells2012301059106322489057
- AcostaACEspanaEMStoiberJCorneal stroma regeneration in felines after supradescemetic keratoprosthesis implantationCornea20062583083817068461