
Abstract
Purpose
Despite international guidelines’ recommendations, spirometry is underutilized in the diagnosis and management of asthma and COPD. Spirometry may be an opportunity for trained pharmacists to meet the needs of patients with suspected or diagnosed lung conditions. The aim of this scoping review is to describe the literature including pharmacist provided spirometry services, specifically to identify: 1) the models of pharmacist provided spirometry services, and additional services commonly offered alongside spirometry, 2) pharmacist training and capability to obtain quality results, and (3) pharmacist, physician, and patient perspectives.
Methods
In September 2020, a comprehensive literature search in PubMed and EMBASE was conducted to identify all relevant literature on the topic of pharmacist provided spirometry services using the search term: “pharmacist or pharmacy” and “spirometry or pulmonary function test or lung function test.” Literature was screened using inclusion/exclusion criteria and selected articles were charted and analyzed using the themes above.
Results
A total of 27 records were included. The scoping review found that pharmacist provided spirometry has been conducted around the world in community pharmacies and clinic settings. Community pharmacists may increase access to spirometry screening; the lack of communication with primary care providers and remuneration are barriers that need to be overcome to optimize the utility of the service. Clinic-based services are interprofessional and collaborative, allowing a patient to receive the test, results, diagnosis, and medication changes in one visit. Following comprehensive training, pharmacists felt confident in their ability to perform spirometry and met quality standards at acceptable rates.
Conclusion
Spirometry is an opportunity for pharmacists to improve evidence-based practice for screening and diagnosing lung conditions along with providing comprehensive services to complement testing. Data around provider and patient perspectives is limited and should be further investigated to determine if providers and patients would value and collaborate with pharmacists providing spirometry services.
Plain Language Summary
Though recommended by guidelines, spirometry is underutilized in the diagnosis and management of asthma and COPD. The purpose of this scoping review is to describe the evidence around spirometry services provided by pharmacists. We describe the models for service implementation, other services offered in conjunction with spirometry, pharmacist training, the quality of pharmacist provided spirometry, and pharmacist, provider, and patient perspectives. Pharmacist provided spirometry has been studied around the world in community pharmacies and clinic settings. Challenges with payment and lack of communication with primary care providers are barriers that were commonly faced in community pharmacy settings, but not in clinic settings. Spirometry was often offered alongside smoking cessation, inhaler education, and medication management services. Spirometry services are an opportunity for pharmacists to expand patient access and improve the quality of care for patients with lung conditions, especially when offered as a package with other clinical pharmacy services.
Introduction
Chronic Obstructive Pulmonary Disease (COPD) has an estimated global prevalence of 11.7% and causes around 3 million deaths annually.Citation1 COPD is a leading cause of morbidity and mortality worldwide and has far reaching economic and social implications.Citation1 The prevalence and burden of COPD are projected to rise over the coming decades.Citation1 Asthma has an estimated worldwide prevalence of 262 million and it is estimated that asthma caused 461,000 deaths worldwide in 2019.Citation2 Poorly controlled asthma is also associated with socioeconomic burden including higher medical costs, productivity loss, and substantial reductions in quality of life.Citation3 Optimal management of these diseases depends on early and accurate diagnosis.Citation1,Citation3 Numerous international guidelines recommend spirometry as the gold standard for diagnosis of COPD and asthma.Citation1,Citation3–Citation5
Spirometry is the most reproducible and objective measurement of airflow limitation.Citation1 It is a noninvasive test that measures the maximal volume of air that an individual can inspire and expire with maximal effort. A spirometry test measures the impact of a disease on lung function, assesses airway responsiveness, and is useful for monitoring disease progression, the effect of therapeutic interventions and determining a prognosis.Citation5
Despite widespread recommendations for spirometry, it is often underutilized in the diagnosis and management of COPD and asthma. Lack of spirometry results can lead to underdiagnosis and misdiagnosis, inappropriate treatment, and missed opportunities to alter disease progression.Citation6 Across the world, studies have shown that only 18–45% of patients diagnosed with COPD received a spirometry test at diagnosis and 7–56% have ever had a spirometry test.Citation6,Citation7 Use of spirometry for asthma diagnosis and management is underwhelming, as well. Only 25% of patients with an asthma diagnosis had evidence of completing spirometry in a study of Canadian primary care practicesCitation8 and a survey of office-based family physicians and pediatricians in the US demonstrated that only 21% routinely use spirometry for all guideline recommended clinical situations.Citation9
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) calls for all healthcare workers who care for patients with COPD to have access to spirometry.Citation1 Global Initiative for Asthma guidelines (GINA) highlight the importance of building the capacity of primary care physicians for asthma diagnosis and management that includes spirometry.Citation3 It is known that good quality spirometry is possible in any healthcare settingCitation1 and the National Lung Health Education Program recommends that “spirometry for screening and case finding should be available in primary care settings and be used for patients at risk for COPD or asthma”.Citation4 In some countries, efforts are being made to improve the access to spirometry in primary care practices,Citation10 but there are still some barriers. The uptake of spirometry in primary care may be limited by primary care providers’ familiarity with guidelines, uncertainty regarding usefulness of test results, and lack of training.Citation4 A study by Saad et al identified challenges to implementing spirometry in primary care practices, which included the need for health professionals to be trained to provide the service, the lack of time of professionals to provide this service, and the lack of confidence when providers do not have sufficient exposure. Family practices involved in the study concluded that it was best to have a trained professional dedicated to performing spirometry and that this facilitated access to the test.Citation11 Other challenges include logistical problems, such as appropriate space within the office to conduct the test and the need for regular calibration of the spirometer.Citation7
Cawley et al have previously introduced spirometry as an opportunity for pharmacists to expand patient care services.Citation12 Trained pharmacists may be well placed to address some of the barriers to implementing spirometry in primary care practices and could serve to expand access and improve the evidence-based use of spirometry for patients with and at risk of COPD and asthma. Previous reviews of pharmacist provided spirometry services have been conducted, but focused narrowly on the ability of pharmacists to meet quality standards for spirometryCitation13 or specifically in the context of COPD services in the community pharmacy setting.Citation14 The purpose of this scoping review was to identify and summarize the available evidence around pharmacist provided spirometry services in all settings.
Methods
This study employed a scoping review methodology, which takes into account all relevant literature, including qualitative, quantitative, mixed methods and unpublished literature.Citation15,Citation16 Unlike a systematic review, which is conducted to answer a specific research question, a scoping review is conducted to answer broader questions, such as “What is the nature of the evidence around this topic?”Citation15,Citation16 The research team discussed and determined the following inclusion criteria to answer the question posed for this review: “What is known about pharmacist provided spirometry services?” Articles and published conference abstracts were included only when a pharmacist was involved in the provision of the spirometry test or in the interpretation and utilization of spirometry test results. Only articles available in English were included. There was no restriction on publication date because the authors wanted to determine the full volume of research on the topic. One reviewer (AV) conducted a comprehensive literature search in PubMed (in titles and abstracts) and EMBASE (in titles, abstracts, and author keywords) using Boolean logic with the following search term: “pharmacist or pharmacy” and “spirometry or pulmonary function test or lung function test.” The initial search was undertaken on September 11, 2020, with location of full text articles and reports for some records identified in the initial search continuing through April 2021. All reviewers also manually searched the references of included articles.
The final search results were imported into ZoteroCitation17 and duplicates were removed. One reviewer (AV) initially screened all abstracts to determine if they potentially met inclusion criteria and those that did not were removed. All reviewers screened the remaining abstracts and reviewers reached consensus on which articles and abstracts met inclusion criteria for the full text review. All reviewers were assigned a subset of the included articles to review and abstract data from using an initial standardized data abstraction form. Reviewers then met to discuss the findings from the articles and to revise the data abstraction tool. Based on the findings, the data abstraction tool was revised to gather data to answer the following questions: (1) What are the models of pharmacist provided spirometry services and what additional services are commonly offered alongside spirometry? (2) How are pharmacists trained to provide spirometry and what is pharmacists’ capability to obtain quality spirometry results? and (3) What are pharmacist, physician, and patient perspectives on pharmacist provided spirometry services? All reviewers used the revised data abstraction tool to abstract data from their assigned articles. A second reviewer was assigned to each article to examine and confirm the data abstracted within the form. As this article was not designed as a systematic review, no papers were excluded on the basis of quality.Citation16 The authors describe all of the relevant literature identified and highlight some of the quality limitations of the existing evidence throughout the findings below.
Findings
As shown in , the initial search yielded 154 articles and conference abstracts. After removing duplicates, 111 unique articles and abstracts were reviewed. After screening for inclusion and exclusion criteria, the authors reviewed and analyzed 26 papers (23 original articles, 2 reviews, and 1 commentary) and one conference abstract. Of those, 24 describe pharmacist provided services in community pharmacy settings (n=16) and clinic-based settings (n=8), such as primary care practices, federally qualified health centers, and an internal medicine multi-specialty practice. Additionally, this review includes two review papers and one paper describing a survey of physicians’ perspectives on the theoretical involvement of pharmacists in spirometry. Included articles described spirometry services in Australia (n=9), Canada (n=1), Italy (n=1), Spain (n=2), the United Kingdom (n=3), and the United States (n=8). With the international nature of this review, it is important to note that the pharmacy practice scope, payment opportunities, relationships with providers (including physicians, nurse practitioners, and physician assistants), and public perception of pharmacists may vary from country to country. describes country, setting, characteristics of spirometry services and additional services provided by the pharmacist.
Figure 1 Flow diagram of the search and selection process used for a literature search for articles on pharmacist-provided spirometry services for a scoping review.
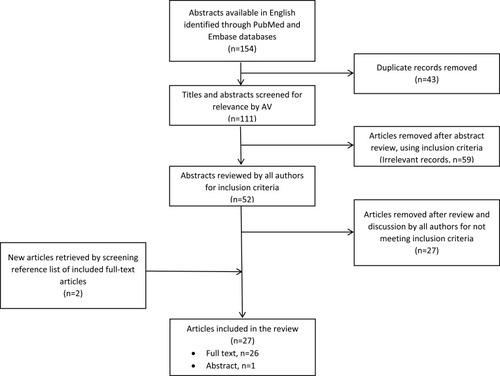
Table 1 Characteristics of Pharmacist-Provided Spirometry Services and Complementary Services
Community Pharmacy Models
A total of 16 papers and reports describing spirometry services in community pharmacy settings were included in this review.Citation18–Citation33 Most community pharmacy spirometry services were pre-bronchodilator tests for screening purposes to identify patients at high risk of COPD,Citation18,Citation23,Citation24,Citation26–Citation29,Citation32 obstructive lung conditions,Citation22,Citation31 or poor asthma outcomesCitation20 (n=11). Additionally, a group of studies conducted in Australia described and assessed implementation of spirometry services for the purposes of asthma management in the community pharmacy setting (n=5).Citation19,Citation21,Citation25,Citation30,Citation33
In community pharmacies, the spirometry service was often incorporated into the normal workflow of the pharmacy.Citation18,Citation23–Citation25,Citation29,Citation30 Additionally, some studies describe other models, such as special booths, screening days or appointment-based models within the pharmacyCitation18,Citation25,Citation27,Citation29 or community pharmacists participating in community health fairs or health screening events at corporate offices.Citation28 Several studies required that participating pharmacies have a private area where the pharmacist could meet with the patient to perform the testCitation20,Citation24–Citation26,Citation30 (n=5) and that at least two pharmacists were on duty at all times (n=4).Citation19,Citation20,Citation25,Citation29 Where it was not required, there was a trend of higher screening rates when a second pharmacist or an intern was on duty.Citation26
Most often patients were recruited for the spirometry service by convenience from customers entering the pharmacy,Citation28,Citation31 though specific customers were typically targeted, usually because they were filling prescriptions for respiratory drugs, purchasing cough medications or smoking cessation products, or endorsed respiratory symptoms or smoking (n=12).Citation18–Citation20,Citation22–Citation26,Citation30,Citation32 Patients were also recruited through advertisements in the newspaper and flyers or posters in the pharmacy.Citation18,Citation22,Citation28,Citation30
For those community pharmacy programs offering a screening service, a screening questionnaire was typically utilized to identify patients’ level of risk for COPD. These questionnaires were either used to identify patients who were eligible to receive the spirometry testCitation18,Citation23,Citation24,Citation29 or were reviewed in addition to the spirometry test results for a comprehensive risk assessment.Citation26,Citation28,Citation32 The eligibility criteria used in these screening programs varied widely. See for eligibility criteria and screening questionnaires used in COPD case-finding studies. It is important to note that screening recommendations for COPD have changed over time. There is also some disagreement between expert guidelines and recommendations vary by geographic location. The GOLD Guidelines recommend spirometry for any patient over age 40 with symptoms and/or risk factors consistent with COPD,Citation1 while the US Preventive Services Task Force recommends against screening for COPD for any patient without symptoms.Citation34 While studies varied in their consistency with these guidelines, they did demonstrate an opportunity for pharmacists to be involved in identifying patients at risk of obstructive lung disease.
Table 2 Outcomes from COPD Case-Finding Spirometry Services in Community Pharmacies
A major challenge that community pharmacists faced was communicating with patients’ primary care providers (PCPs) to provide screening results and recommendations for diagnostic spirometry. In some studies, pharmacists attempted to send recommendations directly to PCPs, while other services required patients to take recommendations back to their PCP. Castillo et al noted that the lack of communication between the PCPs and community pharmacists was a weakness in their study; of 244 patients referred to their PCPs for abnormal results, pharmacists received a communication back from the PCP for only 39.Citation24 Similarly low response rates from PCPs were found in other studies, as well.Citation18,Citation26
Reported outcomes related to pharmacist-provided spirometry services varied across studies, though many reported on quality, as we describe below. For the subset of studies related to a COPD case-finding spirometry service in a community pharmacy setting, common outcome measures were related to patients’ COPD risk, abnormal spirometry results, referrals and recommendations to PCPs and the outcomes of those pharmacist actions.Citation18,Citation23,Citation24,Citation26,Citation28,Citation29,Citation31,Citation32 () The primary goal of a COPD screening service is to identify patients with the condition, and unfortunately, the response rates for determining patient diagnoses were low across studies. While identifying patients at risk of COPD and referring them to primary care are important intermediary steps, it is difficult to determine the ultimate impact on the outcome of interest, which is COPD diagnosis and proper management. Future studies should address this issue. Health information technology and interoperable electronic medical records may help to facilitate this communication between PCPs and community pharmacists and may be an intervention worth assessing in future research.
Several papers from the community pharmacy setting did not specifically address reimbursement for the spirometry service (n=3).Citation23,Citation26,Citation30 For those that did describe it, most often payment was associated with participation in the research study and the funding came from government agencies or drug manufacturers (n=5).Citation18,Citation19,Citation21,Citation25,Citation28 In one study, patient participants paid $10 plus tax to receive the spirometry service.Citation22 In a study in Italy, pharmacists received payments for the spirometry screening service through their National Health Service.Citation31 Another study in the UK evaluated potential cost savings to the National Health Service for the spirometry and smoking cessation service.Citation32 Pharmacists did not receive any incentives or remuneration in some studies, thus the spirometry service was provided to patients at no cost and the costs of the service were subsidized by the pharmacy (n=2).Citation24,Citation29 The service offerings varied across studies, but pharmacists in the study by Allan et al reported that initial and follow-up visits averaged 31 and 15 minutes, respectively, with an additional 28 minutes for paperwork.Citation18
Many authors concluded that trained community pharmacists could effectively perform spirometry services for the purposes of COPD case-finding (n=7).Citation18,Citation23,Citation24,Citation26,Citation28,Citation31,Citation32 Authors also identified that some challenges would need to be addressed for the service to be optimized and sustainable in community pharmacies.Citation18,Citation26,Citation27,Citation29 In one study of pharmacist experiences with a COPD case-finding service, 74% of pharmacists reported that they were likely or very likely to continue providing the service beyond the research study and 89% indicated that they would charge a fee between $5–40 to patients.Citation27 However, most articles describing services in the community pharmacy setting did not mention plans for continuation of the service beyond the study period. Another review identified that community pharmacist motivation for providing spirometry screening services is not well established and that this would need to be addressed for successful broad scale implementation.Citation14 While pharmacists in the community setting may increase access to screening services for patients, the logistical challenges, communication deficiencies with PCPs, and lack of remuneration for spirometry in this setting are barriers that have likely prevented wide-scale implementation.
Clinic-Based Models
Pharmacist provided spirometry services in outpatient, primary care practicesCitation12,Citation35–Citation40 and a multispecialty medical group practiceCitation41 have also been described (n=8). In these settings, spirometry services are more commonly offered for both screening and disease management.Citation35,Citation36,Citation38,Citation40 Models for pharmacist provided spirometry in clinic settings varied, though most utilized an appointment-based model (n=5).Citation35,Citation36,Citation38,Citation39,Citation41 Some clinics offered dedicated days for the spirometry serviceCitation35–Citation37 while others included spirometry in the mix of services offered by the pharmacists.Citation12,Citation38 In the medical practice setting, identifying patients for spirometry services is quite different from the community pharmacy setting. Some studies describe proactive pharmacist identification of patients that may be eligible using information from the electronic medical record (EMR),Citation39,Citation41 while others describe primary care provider referrals as the major driver of patient recruitment.Citation35,Citation38 In the studies that included pharmacist recommendations for spirometry testing, PCP acceptance rates varied from 47% in a COPD case-finding and case-confirming approachCitation39 to 75% for patients already diagnosed with COPD.Citation41 PCPs’ choice of guidelines may impact acceptance rates and they may be less likely to accept recommendations for spirometry for asymptomatic patients without a current respiratory diagnosis.
In the outpatient clinic setting, the typical pharmacist-provided spirometry service included: the spirometry test, an assessment of pulmonary symptoms, medication use, and the results of the spirometry test, medication recommendations, and patient education on the proper use of respiratory devices.Citation35,Citation36,Citation39–Citation41 These visits were scheduled for 60–90 minutesCitation12,Citation35 and often included interprofessional collaboration during the visit.Citation35,Citation36,Citation39,Citation41 Access to the electronic medical record (EMR) is an important component of spirometry services in this setting. In addition to identifying patients, the EMR was utilized to communicate recommendations to providers and to document spirometry results, patient symptoms, and pharmacist assessments and recommendations.Citation35,Citation38,Citation39,Citation41
One major difference between the screening services described in community pharmacy settings and the diagnostic spirometry tests provided in clinic settings was the inclusion of a post-bronchodilator test.Citation35,Citation36 This certainly adds to the length of the visit, as the visit includes administration of the bronchodilator and a waiting period before the post-bronchodilator maneuvers can be performed. For patients who are identified as at risk for obstructive lung conditions, having a diagnostic spirometry test (rather than a screening) saves a step in the process and could result in a patient receiving evidence-based therapies sooner.
Among the studies in clinic settings, Cawley and Warning and Whitner et al included the results of pharmacist provided spirometry tests. In Cawley and Warning, among patients that were able to complete the test to satisfactory standards, 52% had abnormal results and pharmacists aided in identifying reversible airway disease, COPD, restrictive defects, and mixed obstructive/restrictive defects.Citation36 Whitner et al describe correcting inappropriate or misdiagnosis of COPD, new COPD diagnosis, and confirmation of existing COPD diagnosis.Citation39 The interprofessional, collaborative nature of the spirometry services in clinic-based settings allows for immediate diagnosis by the PCP. With a spirometrically-confirmed diagnosis, pharmacists can go on to make guideline-driven recommendations for pharmacotherapy all in the same visit with the patient.
In most cases, remuneration for pharmacist services in clinic settings were not addressed, however, two papers described the average reimbursement for a spirometry visit as $101.12Citation38 and $144.43 ± 36.34,Citation40 which may include the additional medication management services provided. Cawley and Warning specifically call for pharmacists to become familiar with procedural codes for billing spirometry services and suggests pharmacists work with their clinic’s reimbursement specialists.Citation35 The sustainability of spirometry services in these settings is evidenced by the longevity of the programsCitation36,Citation39 and expansion of the service to additional clinic sites.Citation39 Pharmacist consult agreements are cited as an opportunity for further expansion of spirometry services.Citation36,Citation39
Clinic-based spirometry services provided by pharmacists may increase patient access to testing and PCP access to results. Whitner et al found that among patients eligible for spirometry testing based on GOLD guideline criteria for age and smoking status, spirometry was ordered significantly more when a pharmacist proactively recommended the test as compared to usual care (47.2% vs 7.7%, P < 0.001). This resulted in significantly more eligible patients completing a spirometry test (23.2% vs 3.1%, P< 0.001).Citation39 Just the existence of a pharmacist providing spirometry services in their clinic may increase provider referrals. Mueller et al found a significant difference in the percent of all patients with a spirometry referral (1.13% and 0.59%, respectively, P < 0.0001) and the percent of all patients with spirometry results (0.55% and 0.27%, respectively, P = 0.0002) between sites with and without the pharmacist service. Mueller et al also demonstrated a significantly higher completion rate for spirometry when referred to the pharmacist service compared to external pulmonary function testing facilities (70.0% and 40.9%, respectively, P = 0.0004). These results indicate that patients may be more likely to complete spirometry when it is conveniently located in the primary care provider’s office,Citation38 a finding that was also supported by the experiences of pharmacist-managed spirometry in primary care in Minnesota.Citation12 Prospective studies specifically designed to assess the impact of pharmacist-provided services on patient access to spirometry could provide further evidence to support these findings.
Several authors highlight the pharmacist as uniquely positioned to provide spirometry services within clinic settings because of the value-added services they can provide including gathering patient history, assessing spirometry results and medication lists, making guideline-driven medication recommendations, and assessing and educating patients on proper inhaler technique.Citation12,Citation35,Citation38,Citation39 Mueller et al and Mann and Zaiken both concluded that a pharmacist-provided spirometry service within the clinic may increase patient access through increasing referrals for and completion of spirometry tests.Citation38,Citation41 Similar to the studies conducted in community pharmacy settings, these studies identified that existing relationships between the primary care providers and pharmacists led to higher referral rates and recommendation acceptance rates.Citation38,Citation41 Spirometry may be an area of future growth for sustainable, clinic-based pharmacist services. Spirometry testing provides an opportunity for pharmacists to improve evidence-based practice for screening and diagnosis of lung conditions and can provide a pipeline of patients for chronic disease management services under consult agreements.
Pharmacist Training and Ongoing Support
The American Thoracic Society (ATS) and European Respiratory Society (ERS) Standardization of Spirometry 2019 Update highlights a motivated and trained operator as a key element for obtaining high quality spirometry test results.Citation5 The 2019 ATS/ESR guidelines do not endorse any specific training program for spirometry but acknowledge that there are many training programs available and that short term follow-up and supplementary training are integral to maintaining spirometry quality.Citation5 For studies included in this review, initial training for pharmacists varied in the modality, length, accreditation, content, and instructors. Most studies report training pharmacists in person through workshops (n=10).Citation19–Citation21,Citation23–Citation25,Citation28,Citation30,Citation37,Citation41 Some studies describe online training modulesCitation27 or a mixture of online and in person training.Citation18,Citation26 Examples of training content included: disease state pathophysiology and overview (asthma or COPD), spirometry device use, spirometry interpretation, and study protocol. The length of training varied from a couple hours to 4-day (16 hour) workshops. Only one of the studies described having a training program that was accredited,Citation24 and several others noted that their training materials were based on the ATS/ERS quality guidelines or National Institute for Occupational Safety and Health (NIOSH) training material.Citation19,Citation23,Citation36,Citation37 One study noted that training was provided by the National Respiratory Training Center (NRTC).Citation41 Five of the studies reference a cumulative examination after training, in which pharmacists had to demonstrate mastery.Citation21,Citation24–Citation26
Ongoing support, after the initial training, to pharmacists who were providing spirometry services varied greatly in the described studies. Support in some studies consisted of follow-up phone calls to the pharmacists but mainly consisted of patient recruitment and study protocol support.Citation25–Citation27 Other support offered to pharmacists providing spirometry included ongoing access to specialists through telephoneCitation19,Citation22,Citation37 and in person visits by respiratory specialistsCitation22 or nurses.Citation29 Some pharmacists had support in the interpretation of results from physicians/pulmonologist,Citation35,Citation36 physician assistants,Citation41 and respiratory specialists.Citation13,Citation22 The utility of providing ongoing support to the pharmacists was not evident in the reviewed studies. One group of studies mentioned follow-up phone calls from investigators as helping with patient recruitmentCitation26,Citation27 and another mentioned that support was helpful but did not provide specifics.Citation29
Further description and evaluation of the spirometry training provided to pharmacists would be useful to identify programs that demonstrate outcomes that balance the cost and time commitment involved. Future work to evaluate currently available training programs and their effect on the quality of spirometry would be a helpful addition to the literature. For a practitioner desiring to receive training there are a variety of training programs available internationally including: the HERMES spirometry training program developed for practitioners across Europe,Citation42 the Australian and New Zealand Society of Respiratory Science spirometry training program,Citation43 the American Lung Association practitioner training program,Citation44 and the NIOSH spirometry training program.Citation45
Quality
To determine the utility of pharmacist provided spirometry services, it is important to establish that pharmacists can conduct spirometry tests that meet established criteria for quality. The quality of spirometry is generally determined by the accuracy and reproducibility of the spirometry test. There have been several important guidelines that have been largely accepted in rating the quality of spirometry tests,Citation46,Citation47 with the most recent update in 2019 providing a grading system (A, B, C, D, E, U, F) to assess the quality of the test.Citation5 The grading system should help in the interpretation of the results and with the probability that the same result would happen if the test was attempted again. Practitioners should aim for “A” quality, but in cases where that is not possible the results may still be useful.Citation5
Ten of the articles in this review included some information about the quality of the spirometry provided by pharmacists.Citation19,Citation20,Citation22–Citation24,Citation28,Citation33,Citation35–Citation37 describes the devices, quality criteria and results from these articles. It is important to note that there was not consistency in how quality was measured, given the changing parameters of the ATS/ERS guidelines over time. For studies included in this review, 66–94% of pharmacist performed spirometry met the quality standard utilized in the study. A review of pharmacists’ quality of spirometry in 2015, including many of the same studies as this review, noted that pharmacists performed quality spirometry at similar rates to other healthcare professionals.Citation13 In one highlighted study of 13,599 patients, trained healthcare providers maintained ATS/ERS standards in 70–88% of tests performed.Citation48 This current review confirms that pharmacists were able to perform spirometry that met similar quality standards to other healthcare providers, but there is work to be done in assuring that all literature is reporting the same quality data. Future studies should use the most recent quality standards and report outcomes consistent with those standards, allowing for statistical analysis of the spirometry data across the literature.
Table 3 Quality of Pharmacist Provided Spirometry Tests
Complementary Pharmacist Services
Both the GINA and GOLD practice guidelines recognize the value of pharmacists in respiratory disease management, specifically in assessing inhaler technique, providing adherence support, and educating patients about their disease.Citation1,Citation3 In 2011, the American Pharmacists Association Foundation published three opportunities for pharmacists involved in the care of patients with COPD, which also translate to asthma: improving medication adherence, smoking cessation, and medication therapy management.Citation49 These outlined areas of opportunity also appeared to be the most common services offered alongside spirometry throughout the studies included in this review. A summary of the complementary services can be found in .
Many of the pharmacist spirometry services emphasized proper inhaler technique to improve adherence and disease outcomes (n=12).Citation12,Citation18–Citation21,Citation25,Citation30,Citation32,Citation35,Citation36,Citation39,Citation40 The extent of inhaler technique counseling was not thoroughly described in all these programs. Armour et al studies cited utilizing “device-specific checklists” to assess inhaler use,Citation19–Citation21 while others were less descriptive of teaching modalities. It has been established that errors in inhaler technique are associated with poorer disease control and that pharmacists can offer proper interventions and counseling to improve adherence.Citation50 This education is well within the scope of pharmacists and spirometry results could help to measure the impact of proper inhaler use or identify patients who may need additional medication counseling.
Similar to proper inhaler use, it is reasonable to assume that pharmacists managing patients with respiratory disease would prioritize addressing smoking cessation. The review by Twigg and Wright specifically states that
Due to the relationship between smoking and the development of COPD, it is potentially inappropriate to deliver a screening service without having the expertise to deliver (or refer to) a smoking cessation service.Citation14
Within this review, history of smoking was a common part of initial inclusion parameters for screening patients who may benefit from spirometry. Pharmacists commonly provided smoking cessation literature or counseling, with the majority of studies reporting 97–100% of patients identified as smokers receiving this service.Citation23,Citation24,Citation28,Citation35,Citation39 Like adherence efforts, authors noted the existence of smoking cessation interventions, but they were not described in full detail. Aspects of the services such as if pharmacotherapy was offered, or what kind of counseling was given, were unavailable. One study specifically mentioned utilizing the results of spirometry as an objective measure of a patient’s lung health in providing cessation recommendations and counseling.Citation28 A 2019 review by Westerdahl et al concluded that while
studies conducted to date have shown mixed results, there is currently limited evidence in the literature that smoking cessation counseling that includes feedback from spirometry and a demonstration of lung age promotes quit rates.Citation51
However, a recent randomized controlled trial demonstrated that brief smoking cessation advice plus spirometry information doubled prolonged abstinence at 12 months compared to brief advice alone.Citation52 While the data supporting spirometry in smoking cessation is not yet well established, this could be an opportunity for pharmacists to include information such as lung age provided by spirometry, as part of their smoking cessation education services.
The extent of pharmacist involvement in medication management varied across studies. In some studies, pharmacists would review medication lists and provide evidence-based recommendations for altering medication therapy. The strongest evidence of these interventions came from studies of pharmacists in outpatient clinics, where diagnostic spirometry results were utilized.Citation35,Citation36,Citation38,Citation39,Citation41 In these studies, pharmacists recommended medication changes in 46–69% of patients based on evidence-based guidelines.Citation36,Citation38,Citation41 These changes included adding therapy (55%), discontinuing therapy (26%), and/or adjusting doses of medications (12%).Citation35,Citation36 Follow-up data on these recommendations was limited. However, Mueller et al reported 87% of pharmacists’ recommendations were accepted by providers, suggesting they value pharmacist input.Citation38 Medication management services offered in conjunction with spirometry may increase patient engagement and improve clinical and humanistic outcomes. Simpson et al compared an asthma service with and without spirometry and found that patients that had spirometry were more likely to see their PCP when referred by the pharmacist (75% compared to 33%).Citation30 Two cluster randomized controlled trials in Australia demonstrated that a pharmacist asthma management program that includes spirometry positively impacted asthma severity/control, inhaler technique, action plan ownership, asthma-related quality of life, and medication adherence.Citation19,Citation21 It is difficult to discern if these outcomes should be attributed to spirometry or the medication management and patient education components of the service.Citation19,Citation21 Future studies comparing the effectiveness of pharmacist respiratory management services with and without spirometry would provide additional information on the utility of including spirometry in pharmacy-based medication management services.
Overall, there was a lack of details for these other services, their depth, and outcomes. The dearth of outcomes data could be explained by the difference in settings for the services reviewed: community versus outpatient clinic practice. Outpatient clinic practices had access to the EMR, which facilitated communication between pharmacists and providers and allowed for researchers to access additional data that studies in community pharmacy settings did not have access to. Future studies, especially in community pharmacy settings, should seek to streamline communication and ensure access to outcomes data relevant to the services provided.
Lastly, a benefit of spirometry may lie in its ability to attract patients and draw attention to other services. Allan et al revealed pharmacists believed spirometry services served to increase awareness of the pharmacy’s other services.Citation18 Similar to other point of care tests utilized in pharmacy practice, like blood pressure, spirometry could offer an opportunity for pharmacists to collect objective patient information as a part of a comprehensive, evidence-based patient care service. Spirometry services may add the most value when they are complementary and offered in conjunction with other services that leverage pharmacist expertise, like smoking cessation, disease-state and medication education, and collaborative medication management.
Pharmacist Perspectives on Spirometry
Six studies specifically sought to gather feedback from pharmacists offering spirometry services, all of which were in the community pharmacy setting. Survey methods were used in four studies, with response rates varying from 58–100%.Citation18,Citation26–Citation28 Three studies utilized focus groups and/or interviews with participating pharmacists, with sample sizes of 4,Citation29 15,Citation27 and 32.Citation25 Some papers had stronger qualitative research methodology,Citation25,Citation27 while others were designed for the purposes of evaluating the program and did not employ rigorous research methods.Citation18,Citation29 For most studies included in this paper, pharmacists opted in to providing the spirometry service so pharmacist responses may be biased and not reflective of the general pharmacist population.
Several studies found that pharmacists were confident in their ability to provide spirometry services following comprehensive training,Citation28,Citation29 including identifying patients at risk, conducting the test, interpreting results, and referring to primary care providers.Citation26 Fuller et al found that pharmacists with lower comfort had performed fewer spirometriesCitation28 and Allan et al described the importance of initiating the service soon after training to enhance pharmacist confidence.Citation18
Community pharmacists commonly cited patient recruitment as a challenge and some pharmacists felt that they needed more training or support in how to approach patients for this clinical service.Citation25,Citation27,Citation28 Pharmacists identified patients’ lack of awareness of COPD as a barrier to recruitment.Citation27 A known facilitator to patient recruitment is marketing and promotion of the pharmacy service. When the services were well advertised in local media and through screening days supported by the Australian Lung Foundation, pharmacists were inundated with patients requesting spirometry.Citation18
Challenges with pharmacist availability were commonly cited by the community pharmacists as barriers to service implementation and success. Pharmacists reported trying to schedule patients when two pharmacists were on duty so the service could be provided uninterrupted.Citation25,Citation29 Some pharmacies chose to do lung screenings days with a pharmacist dedicated to spirometry so that the service did not interrupt normal workflow of the pharmacy.Citation27 Good staff support is a facilitator to implementation. Pharmacists reported engaging technicians in identifying target patients, recruiting patients and having patients fill out the questionnaire.Citation27 Where pharmacists did not include technicians in the study, they reported envisioning similar roles for support staff if the service were to be continued.Citation18,Citation29
Pharmacists found the service to be professionally rewarding and most reported an interest in continuing the service.Citation18,Citation25,Citation27 Suggested changes for the service involved simplifying documentation,Citation18,Citation27 integrating spirometry with other health screening services,Citation27 addressing time constraints and scheduling issues,Citation25 and increasing demand through advertisements and public awareness campaigns.Citation27,Citation29 For many, remuneration for the service was necessary to continue offering spirometry in the future.Citation18,Citation25,Citation27
Provider Perspectives
One of the most challenging aspects noted in many of the publications was the communication and acceptance of pharmacists’ recommendations to PCPs. Physicians and other primary care providers, like the public, may not be aware of the capabilities and training of a pharmacist.
Tilly-Gratton et al examined Quebec physicians’ agreement on expanding the role of pharmacists in managing asthma. The survey generated a 56% response rate from 420 physicians specializing in family medicine, pediatrics, or emergency medicine. Physicians were asked to rank agreement with the statement
I am comfortable with the professional activities of pharmacists enabling them to offer pulmonary function tests (e.g., spirometry) in the pharmacy to monitor my patient’s therapy.
Only 49% of the physicians agreed by scoring a 4 or 5 on the 6-point Likert scale that pharmacists should offer spirometry for monitoring patients with asthma. The findings of this question should not be surprising. Many physicians may be concerned about the training of the pharmacists and the accuracy of the spirometer used. Other physicians may want to be more involved with the monitoring of their asthma patients and do not feel additional services are needed. This last statement is supported by the authors’ findings where pediatricians and family medicine doctors were more likely to disagree with pharmacists monitoring patients with spirometry compared to emergency department doctors agreeing with pharmacists helping to monitor asthma patients. One limitation noted by the authors was the survey was conducted prior to the passage of a law expanding the pharmacist professional activities, so physicians may not have experience working with pharmacists in these roles.Citation53
Cawley et al provided physician perspectives in a narrative review of successful pharmacist spirometry services at three different primary care settings.Citation12 Spirometry services provided by pharmacists in primary care settings enhanced interprofessional education for family medicine residents and medical students, improved testing convenience for patients and provided prompt results for physicians.Citation12
Future research to gather primary care provider’s perspectives on pharmacist-provided spirometry are warranted given the lack of data that is available. These studies could uncover important perspectives that could influence the design and implementation of spirometry services.
Patient Perspectives
Limited information is available on the patients’ perspectives of pharmacists providing spirometry. A few studies gathered patient feedback and indicated the service to be helpful and convenient. In one study, patients were asked about their satisfaction with the spirometry service and were very satisfied (4.64 standard deviation 0.5, on a scale 0–5, where 5 is very satisfied) and willing to pay for spirometry services that were provided by pharmacists working in Australian independent pharmacies.Citation18 Whereas, patients in the United States were more motivated to attempt quitting smoking after completing free testing in a community pharmacy setting.Citation28 However, patients were challenging to reach by phone and email, post-screening. The numbers of patients surveyed were minimal and bias was present with patients being selected to complete surveys and interviews. Most of the analysis about patient satisfaction came from the pharmacists providing the spirometry service. Overall, community pharmacists indicated patient engagement in testing and reviewing the results, and patient appreciation of free and convenient testing.Citation25,Citation27,Citation29 More analysis of the patient experience with pharmacist provided spirometry in community and other settings is warranted.
Limitations
Our scoping review has some limitations. Despite inclusion of papers describing pharmacist services in six countries, the search may have been limited by the inclusion criteria for records available in English. This scoping review utilized a modified approach in developing the search strategy that deviates from the recommendations for a scoping review from the Joanna Briggs Institute.Citation16 While one author did conduct an initial limited search and discuss the findings with the other authors to determine additional search criteria, a formal analysis of text words in the titles and abstracts and index terms was not done. This may have resulted in some useful terms being left out of our search and some articles may have been missed as a result. Another limitation is that the authors used PubMed and EMBASE databases for the search, which results in an approximate yield of 92%, meaning some articles may have been missed.Citation54 Including additional databases, such as Google Scholar and Web of Science may have resulted in an additional 1–2 articles being identified for inclusion.Citation54 Given that there were many common themes across the articles that were identified, the authors did not feel that an additional 1–2 articles would significantly alter the findings of this review.
Conclusion
Studies of pharmacist provided spirometry have been conducted around the world in community pharmacies and clinic-based practices. While community pharmacists may increase access to spirometry screening services for patients, the lack of communication with PCPs and lack of remuneration for spirometry in this setting are barriers that need to be overcome to optimize the utility of spirometry services in the community pharmacy setting. Clinic-based spirometry services provided by pharmacists may increase patient access to diagnostic testing and PCP access to results, as providers may be more likely to refer patients when a service exists in their practice and patients may be more likely to complete spirometry when it is conveniently located in the PCP’s office. Clinic-based services were often interprofessional and collaborative, allowing a patient to receive the test, test results, diagnosis, and medication changes all in one visit. Pharmacists were able to secure payment in clinic settings, making spirometry a potential area of future growth for sustainable pharmacist services.
Spirometry services were often offered with other clinical pharmacy services such as smoking cessation, inhaler technique assessment and adherence support, and medication management. Collaborative practice agreements for chronic disease management for pulmonary conditions and tobacco use are opportunities for pharmacists to leverage their expertise and spirometry could be a complementary service that supports those services.
This review confirmed that pharmacists can meet quality standards for spirometry at rates similar to other healthcare providers. Following comprehensive training, pharmacists felt confident in their ability to perform spirometry and found the service to be professionally rewarding. Data around provider and patient perspectives is limited and should be further investigated to determine if providers and patients would find value in and be willing collaborators for pharmacist provided spirometry services.
Spirometry testing provides an opportunity for pharmacists to improve evidence-based practice for screening and diagnosis of lung conditions and can provide a pipeline of patients for chronic disease management services under consult agreements.
Disclosure
The authors report no conflicts of interest in this work.
References
- Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease 2021 report; 2020. Available from: https://goldcopd.org/2021-gold-reports/. Accessed 730, 2021.
- VosT, LimSS, AbbafatiC, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-933069326
- Global Initiative for Asthma. Global strategy for asthma management and prevention 2020; 2020. Available from: www.ginasthma.org. Accessed 730, 2021.
- RuppelGL, CarlinBW, HartM, DohertyDE. Office spirometry in primary care for the diagnosis and management of COPD: national lung health education program update. Respir Care. 2018;63(2):242–252. doi:10.4187/respcare.0571029367384
- GrahamBL, SteenbruggenI, MillerMR, et al. Standardization of spirometry 2019 update. An official American Thoracic Society and European Respiratory Society technical statement. Am J Respir Crit Care Med. 2019;200(8):e70–e88. doi:10.1164/rccm.201908-1590ST31613151
- RadinA, CoteC. Primary care of the patient with chronic obstructive pulmonary disease-part 1: frontline prevention and early diagnosis. Am J Med. 2008;121(7):S3–S12. doi:10.1016/j.amjmed.2008.04.002
- YuWC, FuSN, TaiEL, et al. Spirometry is underused in the diagnosis and monitoring of patients with chronic obstructive pulmonary disease (COPD). Int J Chron Obstruct Pulmon Dis. 2013;8:389–395. doi:10.2147/COPD.S4865924009418
- TsuyukiRT, SinDD, SharpeHM, et al. Management of asthma among community-based primary care physicians. J Asthma. 2005;42(3):163–167. doi:10.1081/JAS-5461515962871
- DombkowskiKJ, HassanF, WasilevichEA, ClarkSJ. Spirometry use among pediatric primary care physicians. Pediatrics. 2010;126(4):682–687. doi:10.1542/peds.2010-036220819894
- GlasgowN. Systems for the management of respiratory disease in primary care - an international series: Australia. Prim Care Respir J. 2008;17(1):19–25. doi:10.3132/pcrj.2008.0001518322632
- SaadN, SedenoM, MetzK, BourbeauJ. Early COPD diagnosis in family medicine practice: how to implement spirometry?Int J Family Med. 2014;2014:1–6. doi:10.1155/2014/962901
- CawleyMJ, MoonJ, ReinholdJ, WilleyVJ, Warning IiWJ. Spirometry: tool for pharmacy practitioners to expand direct patient care services. J Am Pharm Assoc. 2013;53(3):307–315. doi:10.1331/JAPhA.2013.12134
- CawleyMJ, WarningWJ. Pharmacists performing quality spirometry testing: an evidence based review. Int J Clin Pharm. 2015;37(5):726–733. doi:10.1007/s11096-015-0160-x26148860
- TwiggMJ, WrightDJ. Community pharmacy COPD services: what do researchers and policy makers need to know?Integr Pharm Res Pract. 2017;6:53–59. doi:10.2147/IPRP.S10527929354551
- TriccoAC, LillieE, ZarinW, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-085030178033
- PetersMDJ, GodfreyCM, KhalilH, McInerneyP, ParkerD, SoaresCB. Guidance for conducting systematic scoping reviews. Int J Evid Based Healthc. 2015;13(3):141–146. doi:10.1097/XEB.000000000000005026134548
- Roy Rosenzweig Center for History and New Media at George Mason University. Zotero; 2021. Available from: https://www.zotero.org/. Accessed 730, 2021.
- AllanH, DiamandisS, SainiB, MarshallD, GavagnaG, Peterson-ClarkG. A collaborative screening, referral and management process to improve health outcomes in Chronic Obstructive Pulmononary Disease (COPD). Australian Government Department of Health and Ageing; 2021. Available from: https://6cpa.com.au/resources/fourth-agreement/a-collaborative-screening-referral-and-management-process-to-improve-health-outcomes-in-chronic-obstructive-pulmonary-disease-copd/. Accessed 35, 2021.
- ArmourC, Bosnic-AnticevichS, BrillantM, et al. Pharmacy Asthma Care Program (PACP) improves outcomes for patients in the community. Thorax. 2007;62(6):496–502. doi:10.1136/thx.2006.06470917251316
- ArmourCL, LeMayK, SainiB, et al. Using the community pharmacy to identify patients at risk of poor asthma control and factors which contribute to this poor control. J Asthma. 2011;48(9):914–922. doi:10.3109/02770903.2011.61543121942306
- ArmourCL, ReddelHK, LeMayKS, et al. Feasibility and effectiveness of an evidence-based asthma service in Australian community pharmacies: a pragmatic cluster randomized trial. J Asthma. 2013;50(3):302–309. doi:10.3109/02770903.2012.75446323270495
- BurtonMA, BurtonDL, SimpsonMD, GissingPM, BowmanSL. Respiratory function testing: the impact of respiratory scientists on the training and support of primary health care providers. Respirology. 2004;9(2):260–264. doi:10.1111/j.1440-1843.2004.00563.x15182279
- CastilloD, GuaytaR, GinerJ, et al. COPD case finding by spirometry in high-risk customers of urban community pharmacies: a pilot study. Respir Med. 2009;103(6):839–845. doi:10.1016/j.rmed.2008.12.02219200706
- CastilloD, BurgosF, GuaytaR, et al. Airflow obstruction case finding in community-pharmacies: a novel strategy to reduce COPD underdiagnosis. Respir Med. 2015;109(4):475–482. doi:10.1016/j.rmed.2015.02.00925754101
- EmmertonLM, SmithL, LeMayKS, et al. Experiences of community pharmacists involved in the delivery of a specialist asthma service in Australia. BMC Health Serv Res. 2012;12:164. doi:10.1186/1472-6963-12-16422709371
- FathimaM, SainiB, FosterJM, ArmourCL. Community pharmacy-based case finding for COPD in urban and rural settings is feasible and effective. Int J Chron Obstruct Pulmon Dis. 2017;12:2753–2761. doi:10.2147/COPD.S14507329075108
- FathimaM, SainiB, FosterJM, ArmourCL. A mixed methods analysis of community pharmacists’ perspectives on delivering COPD screening service to guide future implementation. Res Social Adm Pharm. 2019;15(6):662–672. doi:10.1016/j.sapharm.2018.08.00730131254
- FullerL, ConradWF, HeatonPC, PanosR, EschenbacherW, FredeSM. Pharmacist-managed chronic obstructive pulmonary disease screening in a community setting. J Am Pharm Assoc (2003). 2012;52(5):e59–e66. doi:10.1331/JAPhA.2012.1110022975798
- KrskaJ, CorlettS. Evaluation of NHS Health Checks provided by community pharmacists with the addition of spirometry. 2014. Available from: https://www.researchgate.net/profile/Janet-Krska/publication/272453266_Evaluation_of_NHS_Health_Checks_with_the_addition_of_spiromtery_testing_Lewisham_CCG/links/54e46d5b0cf2dbf606968cd3/Evaluation-of-NHS-Health-Checks-with-the-addition-of-spiromtery-testing-Lewisham-CCG.pdf. Accessed December 17, 2020.
- SimpsonMD, BurtonDL, BurtonMA, GissingPM, BowmanSL. Pharmaceutical care: impact on asthma medication use. J Pharm Pract Res. 2004;34(1):26–29. doi:10.1002/jppr200434126
- SolidoroP, BraidoF, BarattaF, et al. FEV6 assessment in spirometric abnormalities screening: the first population-based study in Italian pharmacies. Panminerva Med. 2013;55(1):87–92.23474666
- WrightD, TwiggM, ThornleyT. Chronic obstructive pulmonary disease case finding by community pharmacists: a potential cost-effective public health intervention. Int J Pharm Pract. 2015;23(1):83–85. doi:10.1111/ijpp.1216125371146
- Lei BurtonD, LeMayKS, SainiB, et al. The reliability and utility of spirometry performed on people with asthma in community pharmacies. J Asthma. 2015;52(9):913–919. doi:10.3109/02770903.2015.100468425563059
- SiuAL, Bibbins-DomingoK, GrossmanDC, et al.; US Preventive Services Task Force (USPSTF). Screening for chronic obstructive pulmonary disease: US Preventive Services Task Force recommendation statement. JAMA. 2016;315(13):1372–1377. doi:10.1001/jama.2016.2638.27046365
- CawleyMJ, PacittiR, WarningW. Assessment of a pharmacist-driven point-of-care spirometry clinic within a primary care physicians office. Pharm Pract (Granada). 2011;9(4):221–227. doi:10.4321/s1886-3655201100040000724198860
- CawleyMJ, WarningWJ. Impact of a pharmacist-driven spirometry clinic service within a community family health center: a 5-year retrospective review. J Res Pharm Pract. 2018;7(2):88–94. doi:10.4103/jrpp.JRPP_17_10130050962
- LicskaiCJ, SandsTW, PaolattoL, NicolettiI, FerroneM. Spirometry in primary care: an analysis of spirometery test quality in a regional primary care asthma program. Can Respir J. 2012;19(4):249–254. doi:10.1155/2012/65308422891184
- MuellerLA, ValentinoAS, ClarkAD, LiJ. Impact of a pharmacist-provided spirometry service on access to results in a primary care setting. J Prim Care Commun Health. 2018;9:2150132718759213. doi:10.1177/2150132718759213
- WhitnerJB, MuellerLA, ValentinoAS. Pharmacist-driven spirometry screening to target high-risk patients in a primary care setting. J Prim Care Commun Health. 2019;10:2150132719889715. doi:10.1177/2150132719889715
- WilleyVJ, SimonS, AkkineniS, et al. Pharmacist-led services to patients with respiratory diseases: feasible from a quality and reimbursement perspective?Value Health. 2013;16(3):A198. doi:10.1016/j.jval.2013.03.998
- MannRP, ZaikenK. Management of chronic obstructive pulmonary disease by pharmacists in an internal medicine department. Am J Health Syst Pharm. 2009;66(10):890, 892–893. doi:10.2146/ajhp08025819420305
- CooperB, SteenbruggenI, MitchellS, et al. HERMES spirometry: the European spirometry driving licence. Breathe. 2011;7(3):258–275. doi:10.1183/20734735.026310
- SwanneyMP, O’DeaCA, IngramER, RodwellLT, BorgBM. Spirometry training courses: content, delivery and assessment - a position statement from the Australian and New Zealand Society of Respiratory Science. Respirology. 2017;22(7):1430–1435. doi:10.1111/resp.1313328681980
- American Lung Association. Spirometry training; 2021. Available from: https://www.lung.org/professional-education/training-certification/spirometry-training. Accessed 56, 2021.
- RogersK, MartinM, ClarkK. National Institute for Occupational Safety and Health Spirometry Training Program. US Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No 2019-110. 2019. doi:10.26616/NIOSHPUB2019110.
- American Thoracic Society. Standardization of spirometry, 1994 update. Am J Respir Crit Care Med. 1995;152(3):1107–1136. doi:10.1164/ajrccm.152.3.7663792.7663792
- MillerMR, HankinsonJ, BrusascoV, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.0003480516055882
- EnrightPL, SklootGS, Cox-GanserJM, UdasinIG, HerbertR. Quality of spirometry performed by 13,599 participants in the world trade center worker and volunteer medical screening program. Respir Care. 2010;55(3):303–309.20196879
- BlumlBM; American Pharmacists Association Foundation null. White paper on expanding the role of pharmacists in chronic obstructive pulmonary disease: American Pharmacists Association Foundation. J Am Pharm Assoc. 2011;51(2):203–211. doi:10.1331/JAPhA.2011.11513
- HuddTR. Emerging role of pharmacists in managing patients with chronic obstructive pulmonary disease. Am J Health Syst Pharm. 2020;77(19):1625–1630. doi:10.1093/ajhp/zxaa21632699897
- WesterdahlE, EngmanKO, ArneM, LarssonM. Spirometry to increase smoking cessation rate: a systematic review. Tob Induc Dis. 2019;17:31. doi:10.18332/tid/10609031516474
- Martin-LujanF, Basora-GallisaJ, VillalobosF, et al. Effectiveness of a motivational intervention based on spirometry results to achieve smoking cessation in primary healthcare patients: randomised, parallel, controlled multicentre study. J Epidemiol Commun Health. 2021. doi:10.1136/jech-2020-216219
- Tilly-GrattonA, LamontagneA, BlaisL, et al. Physician agreement regarding the expansion of pharmacist professional activities in the management of patients with asthma. Int J Pharm Pract. 2017;25(5):335–342. doi:10.1111/ijpp.1232027774739
- BramerWM, RethlefsenML, KleijnenJ, FrancoOH. Optimal database combinations for literature searches in systematic reviews: a prospective exploratory study. Syst Rev. 2017;6(1):245. doi:10.1186/s13643-017-0644-y29208034