
Abstract
Women and couples continue to experience unintended pregnancies at high rates. In the US, 45% of all pregnancies are either mistimed or unwanted. Mishaps with contraceptives, such as condom breakage, missed pills, incorrect timing of patch or vaginal ring application, contraceptive nonuse, forced intercourse, and other circumstances, place women at risk of unintended pregnancy. There is a critical role for emergency contraception (EC) in preventing those pregnancies. There are currently three methods of EC available in the US. Levonorgestrel EC pills have been available with a prescription for over 15 years and over-the-counter since 2013. In 2010, ulipristal acetate EC pills became available with a prescription. Finally, the copper intrauterine device remains the most effective form of EC. Use of EC is increasing over time, due to wider availability and accessibility of EC methods. One strategy to expand access for both prescription and nonprescription EC products is to include pharmacies as a point of access and allow pharmacist prescribing. In eight states, pharmacists are able to prescribe and provide EC directly to women: levonorgestrel EC in eight states and ulipristal acetate in seven states. In addition to access with a prescription written by a pharmacist or other health care provider, levonorgestrel EC is available over-the-counter in pharmacies and grocery stores. Pharmacists play a critical role in access to EC in community pharmacies by ensuring product availability in the inventory, up-to-date knowledge, and comprehensive patient counseling. Looking to the future, there are opportunities to expand access to EC in pharmacies further by implementing legislation expanding the pharmacist scope of practice, ensuring third-party reimbursement for clinical services delivered by pharmacists, and including EC in pharmacy education and training.
Introduction
Women and couples continue to experience unintended pregnancies at high rates. In the US, 45% of all pregnancies are unintended, either mistimed or unwanted.Citation1 Nearly all (95%) of unintended pregnancies are due to nonuse or incorrect/inconsistent use of contraception.Citation2
Condoms and oral contraceptive pills remain the most commonly used methods of contraception in the US, with typical use-failure rates of 18% and 9%, respectively, in the first year of use.Citation3 Both of these commonly used contraceptive methods have potential for mishaps, such as condom breakage and missed pills. Such mishaps as these, in addition to contraceptive nonuse, forced intercourse, and other circumstances, place women at risk of unintended pregnancy. There is a critical role for emergency contraception (EC) in preventing unintended pregnancies.
EC is any form of contraception, hormonal or nonhormonal, that prevents pregnancy after sexual intercourse. There are currently two methods of EC approved by the US Food and Drug Administration (FDA) and a third that is used off-label (see ). Previously, there was a dedicated combination EC product and some combination oral contraceptives used in larger doses for EC, known as the Yuzpe regimen. The Yuzpe regimen fell out of favor, because it was less effective than methods available currently and was associated with increased adverse effects, such as nausea, vomiting, and breast tenderness.
Table 1 Overview of emergency contraception methods
Use of EC is increasing over time, due to wider availability and accessibility of EC methods. Whereas only 1% of women of reproductive age had ever used EC in 1995, 11% had as of 2006–2010.Citation4 Among women who have used EC, most (59%) have only used it once, 24% have used it twice, and 17% have used it three or more times.Citation4 EC users are more likely to be young, never married, and have some college education.Citation4 Similarly, in the last decade, EC use has increased from 8% of teens in 2002 to 22% of teens in 2011–2013.Citation5 A recent study among uninsured adolescents found a high rate of EC awareness and low EC knowledge.Citation6 Increasing EC use is due in part to new products being approved (ie, ulipristal acetate [UPA]) and changing regulations on existing products, namely removal of age and identification restrictions for over-the-counter (OTC) levonorgestrel.
To increase knowledge and use of EC, one strategy utilized has been expansion of access points for both prescription and nonprescription products to include pharmacies. Direct access to prescription drugs from pharmacists is called pharmacist prescribing or pharmacy access. See explanations for the various models of access in . In eight states, pharmacists are able to prescribe and provide EC directly to women (). This paper aims to review the role of the community pharmacist in EC counseling and delivery in the US. Historical and current trends are reviewed, then future prospects and opportunities presented.
Table 2 Models of access to emergency contraception in the US
Table 3 States allowing pharmacist prescribing of EC
Trends
Levonorgestrel
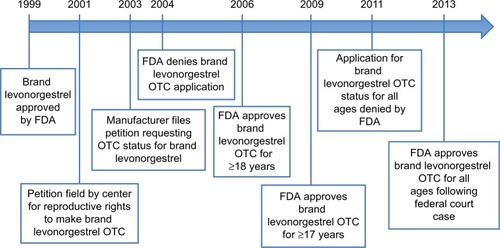
The first dedicated progestin-only EC product was approved in the US in 1999 by the FDA. The effectiveness of levonorgestrel EC products for preventing pregnancies is up to 89%, and is primarily thought to be due to the suppression of ovulation. Other possible mechanisms of action include thickening of cervical mucus and prevention of sperm transport.Citation7–Citation9 Effectiveness is greater the sooner levonorgestrel EC is taken after unprotected intercourse, and declines with time.Citation7,Citation10 The first dedicated product consisted of two tablets of 0.75 mg levonorgestrel, each to be taken 12 hours apart. Soon after FDA approval, the manufacturer pursued switching the product to OTC in 2003. It took several years to overcome politically charged hurdles before approval was obtained in 2006 for OTC status for women and men aged 18 years and older with government-issued identification.Citation11
With the 2006 FDA approval of brand levonorgestrel for OTC sales for consumers aged 18 years and older, the medication itself was kept behind the pharmacy counter and required a visit to a pharmacy and an interaction with a pharmacy employee to purchase it. In addition, government-issued photo identification was required to prove the age of the consumer. In 2009, following a federal court case, the minimum age to obtain EC OTC was lowered from 18 to 17 years. Ultimately, after another legal challenge, in 2013 the FDA removed the age restriction. See for a timeline of levonorgestrel EC.
Figure 1 History of levonorgestrel EC. Data fromCitation65,Citation66
Before levonorgestrel EC became available OTC, multiple states (Alaska, California, Hawaii, Maine, Massachusetts, New Hampshire, New Mexico, Vermont, and Washington) passed legislation allowing pharmacists to prescribe EC and improve access. Since this time, New Hampshire and Vermont have allowed their legislation to expire; however, the authority may be incorporated into future legislative proposals for pharmacist prescribing of hormonal contraceptives. Pharmacist prescribing of EC enabled pharmacists who underwent additional training under individual collaborative or statewide protocols to prescribe and dispense EC directly to patients. Studies examining availability of and access to EC through pharmacist prescribing have shown variable results and persistent barriers to access, in particular for adolescents.
A study in California found that English- and Spanish-speaking adolescents who called pharmacies listed as participating in pharmacist prescribing of EC (listings on www.ec-help.org) inquiring about anything that could be taken after unprotected sex to prevent pregnancy were told to come in to obtain EC 48% and 28% of the time, respectively.Citation12 A 2012 study found that although EC was available at a majority of pharmacies (80%), adolescent mystery callers posing as 17-year-olds were only given the correct information about age requirements half the time, and misinformation was more common in low-income neighborhoods.Citation13 More recent studies have also shown persistent barriers to access. A minority (20%) of Colorado pharmacies had EC in stock and on the shelf in 2014.Citation14 A study published in 2016 that examined availability and access in community pharmacies in Wyoming showed that although 88% of pharmacies stocked EC, only 16% had it in stock and on the shelf.Citation15
While levonorgestrel EC pills have been available with a prescription for over 15 years, multiple studies have shown that physician knowledge and prescribing of EC is not ideal and there is an opportunity for pharmacists to fill the gaps. A recent national multispecialty survey found that while 95% of health care providers had heard of levonorgestrel, providing it to patients was not as common. Family medicine (69%) and emergency medicine (74%) providers self-reported higher rates of providing levonorgestrel to their patients when compared to internal medicine (42%) and pediatrics (55%).Citation16 Studies of pediatric emergency department providers have shown further evidence of knowledge deficits and underutilization of EC in emergency department settings.Citation17,Citation18 A survey of family medicine physicians found that in 1 year, an average of 3.3 EC prescriptions were written and only 63% correctly answered the question regarding the timeframe in which EC should be taken.Citation19 A national survey of obstetrician–gynecologists found that only half (51%) offered EC to all women and a small proportion (6%) never offered it or only offered it after sexual assault (6%).Citation20
Though pharmacists are accessible providers for patients seeking information and care regarding EC, some pharmacists also have knowledge deficits regarding levonorgestrel EC. Past reports in the media and medical literature have described pharmacists as uneducated regarding EC and unwilling to dispense or stock EC.Citation21–Citation25 However, as levonorgestrel EC availability has grown, so has pharmacist knowledge and awareness increased. Other literature has been published showing pharmacists as more educated and engaged in the provision of levonorgestrel EC.Citation26–Citation28
Pharmacists as accessible health care providers should be knowledgeable regarding different methods of EC. One study found that the most important predictor of pharmacists’ dispensing EC was individual pharmacists’ understanding correct information about EC, particularly mechanism of action.Citation29 Recent regulatory status changes, including the elimination of a minimum age for OTC sales of levonorgestrel EC, make the pharmacist’s role in provision of EC education to patients more crucial than before. Studies have shown that a brief pharmacist-driven counseling session about EC had a positive effect on patients’ knowledge of EC and that EC counseling is feasible in a retail pharmacy setting.Citation30,Citation31 Given the influence that pharmacists may have on educating patients regarding EC, pharmacists should understand and be able to counsel on the proper use, side effects, advanced provision, and effectiveness of EC.
Women presenting within 120 hours of unprotected intercourse should be offered EC. There is some debate regarding possible decreased effectiveness of levonorgestrel in women with a body mass index (BMI) of 25 kg/m2 or greater.Citation9,Citation32.Citation33 The FDA is asking for more data, and at this time has not recommended any labeling changes for levonorgestrel EC in women with higher BMI. There are some recommendations, however, regarding women with BMI >25 that include referrals for UPA or copper intrauterine device (IUD) and for those with a BMI >35 to be referred to a trained provider for a copper IUD, if accessible in a timely fashion. Women with higher BMI should not be denied levonorgestrel or UPA EC, but should be made aware of the possible decrease in effectiveness and referred for optimal pregnancy prevention.Citation9
Ulipristal acetate
The availability of OTC levonorgestrel has opened the door for other prescription EC products to be available via pharmacist prescribing, such as UPA, known by the brand name Ella (Afaxys Inc, Charleston, SC, USA). This form of EC works as a progestin receptor antagonist, delaying or inhibiting ovulation when taken.Citation34,Citation35 UPA is a 30 mg tablet that is taken once within 120 hours after unprotected sex to prevent pregnancy. Given its different mechanism of action compared to levonorgestrel EC, its efficacy does not decrease with time. Therefore, it works equally well on day 1 after unprotected sex as it does on day 4.Citation36
UPA was approved for use as EC in the US in August 2010, and sales began in December of that year. However, in 2014 there were significant UPA access issues when the sole US distributor discontinued this product. The manufacturer then partnered with a new distributor.Citation37 Unfortunately, as a result of this disruption in the supply chain, there was approximately 1 year where major drug wholesalers were unable to obtain and distribute UPA to retail pharmacies.Citation38 The resulting shortage likely slowed integration of this product in clinical practice, because even if patients were able to obtain a prescription, they were unable to fill their prescription at the pharmacy. Additionally, while the company did promote UPA to health care providers once it was readily available through the supply chain again, it is reasonable to assume that some providers and patients were or still are unaware that UPA is again available in pharmacies.Citation38
Ultimately, there are many factors that play into pharmacy-stocking practices, but lack of consumer demand for a product is likely a significant component. A 2016 study demonstrated that the majority of clinicians were unfamiliar with UPA as EC, with only 50% of reproductive health providers and 15% of emergency medicine providers reporting that they were familiar with UPA.Citation16 Additionally, if patient and providers demand is low, it is less likely that the drug will be readily stocked in pharmacies. In a mystery caller study conducted in Hawaii in 2013–2014, 198 pharmacies were called and only 2.6% of pharmacies had UPA immediately available, although an additional 22.8% reported ability to order UPA and 82% had levonorgestrel in stock.Citation39 Another study conducted by Brant et al in Massachusetts in 2013 used a mystery caller to determine availability of Ella in 100 community pharmacies, of which 89% had levonorgestrel EC in stock compared to only 7% of pharmacies that had UPA in stock.Citation40 This disparity in EC product availability may be related in part to the previous disruption to the UPA supply chain.Citation39 In summary, these data suggest that although UPA is more effective than levonorgestrel as EC, most clinicians are not prescribing and may not be aware of UPA EC, and it is rarely immediately available in the pharmacy.
UPA remains prescription only, and seven states allow pharmacists to prescribe it under a collaborative practice agreement or statewide protocol. It is also available through several telemedicine providers and online pharmacies. These online providers do not require a face-to-face visit with a providers to obtain a prescription; instead, the patient is asked specific screening questions and the online pharmacy collaborates with a licensed prescriber and pharmacist to prescribe, fill, and ship UPA to the patient’s home.Citation41,Citation42 However, these online pharmacies are unable to ship to certain states.Citation42 Purchase from an online provider may be slightly more expensive, but may still be a valuable resource for many patients who are otherwise unable to access EC. This option is best for those who want to keep EC on hand for future use, rather than urgent use following an act of unprotected intercourse.
Lastly, studies have found that pharmacists may also benefit from additional training regarding UPA for EC. The Massachusetts study revealed that pharmacy staff members often provided incorrect information regarding UPA EC, as only 25% were able to identify Ella was the superior oral EC product 72–120 hours after intercourse.Citation40 Regarding EC in general, only 21% of pharmacy staff gave completely medically accurate information, while 30% gave a “mixture of accurate and inaccurate” information and 34% gave “mostly inaccurate” information.Citation40
Copper IUDs
Nonhormonal copper-containing IUDs have been used for EC for at least 40 years.Citation43 In the US, the copper IUD has been available since 1988. Contraception is effective immediately after IUD placement.Citation44 The most commonly reported adverse effects associated with this IUD are abnormal menstrual bleeding and increased frequency and/or intensity of cramps and pain. The benefit of using this method of EC is the continued contraception, which lasts 10 years, although evidence suggests that copper IUDs are highly effective up to 12 years.Citation45 Although progestin-releasing hormonal IUDs are available (Mirena®, Skyla®, Liletta®, and Kyleena®), none of these has been studied as EC. There has been one study evaluating pregnancy rates after the use of levonorgestrel EC and concomitant placement of a levonorgestrel IUD following unprotected intercourse.Citation46
Various mechanisms of action have been suggested for the IUD. Prefertilization effects, including decreased sperm motility and viability, change in the speed of ovum transport, and damage or destruction of the ovum, are the likely mechanisms of the copper IUD.Citation47 Postfertilization effects including damage and/or destruction of the fertilized ovum are additional possible mechanisms.Citation48 Both prefertilization and postfertilization effects occur prior to implantation.Citation44
A systematic review reported that copper IUDs are the most effective method of EC, with a failure rate of less than one per thousand.Citation49 This compares favorably to the reported failure rates of UPA and levonorgestrel. Unlike other methods of EC, the efficacy of the copper IUD appears to be unaffected by the user’s BMI, time of menstrual cycle at insertion (after a negative urine pregnancy test), or additional acts of unprotected intercourse after placement.Citation50 In addition to its superior efficacy, the IUD does not require ongoing efforts for proper use either.
The costs of IUDs have been a barrier to their use, for both patients and providers. Prices for an IUD typically range between US$500 and $1,000, in addition to provider visits for insertion, removal, and confirmation that the device was properly placed.Citation51 While many insurance plans have covered IUDs for years, prior to passage of the Affordable Care Act (ACA), women were likely to have out-of-pocket charges for the product and the associated visits. The ACA mandates coverage for the copper IUD without cost sharing. The ACA has eliminated these costs for many women. It remains to be seen if the ACA leads to increases in the use of the copper IUD as a form of contraception, including EC.Citation52 The pharmacist’s role pertaining to the copper IUD as EC is primarily in providing comprehensive counseling to women so they are aware of all of their options, as well as providing referrals to providers who can provide same-day or timely insertions.
Little is known about pharmacists’ knowledge of copper IUDs as EC; however, several studies have reported misconceptions of other health care providers regarding IUDs. A 2013 survey found that 33% of obstetrician–gynecologists who provide IUD services believed that this method of contraception is inappropriate for nulliparous women, and 57% believed IUDs should not be used in adolescents.Citation53 Further, this study found that 26% of participants did not agree that the copper IUD can be used as EC.Citation53 Currently, both the American College of Obstetricians and Gynecologists and the American Academy of Pediatrics promote IUD use as a first-line contraceptive option for all women, including young women and those who have never been pregnant.Citation54,Citation55 There is an inverse relationship between the effectiveness of various EC methods and pharmacist involvement, where pharmacists have the largest role with levonorgestrel.
Future prospects
Payment for pharmacist services
As the scope of practice for delivering clinical services expands for pharmacists, payment for the provision of these services must be received and models for payment sustainable. In a recent systematic review of payment to pharmacists for patient care, a majority (73%) of compensated or remunerated clinical services were paid for by government agencies, with the remainder funded by private insurance plans.Citation56 This highlights the importance of obtaining support at the federal level for payment of pharmacist EC services, such as patient visits where EC is prescribed. The concept of payment for chronic care-management services has been addressed by the Centers for Medicare and Medicaid Services, but clarity for EC services has not been provided.Citation57
Given that services for EC may not typically involve full medication review (or comprehensive medication management), time-dependent reimbursement may be most appropriate. This time would include screening and counseling to identify the most appropriate EC method, instructing patients about the proper use of EC, and potential discussion of routine contraceptive methods. In 2014, an evaluation of 60 remunerated pharmacist clinical care programs worldwide indicated time-dependent fees were reimbursed at $93.60 per hour.Citation56
Pharmacy education to include advance provision
Pharmacists must have the knowledge and confidence to provide information to patients regarding various methods of EC, their effectiveness, and how to use them properly. Studies have demonstrated gaps in pharmacist knowledge that may result in incorrect information or advice given to patients seeking EC.Citation15,Citation58,Citation59 Furthermore, education is needed to allow access to EC in a timely manner.Citation15,Citation60 In one small study, educating pharmacists about the use of the copper IUD for EC increased referral and uptake by women of the copper IUD almost threefold.Citation61 Suggestions to improve knowledge and behavior include standardized protocols at the community pharmacy when patients are seeking EC, updated training (eg, continuing professional education) of pharmacists, and mandatory private consultation areas to enhance the counseling environment. These types of educational initiatives have the potential to reduce unintended pregnancies now and in the future.
Additionally, advance provision of EC may increase timely use. Pharmacists should be educated to inform women and men of having EC available prior to occasions when sexual intercourse is unprotected or underprotected. EC can be purchased online for privacy and at low cost, but is not a viable option for immediate use. Furthermore, caution should be used with online purchases, as EC products may be fraudulent. In a systematic review of 17 articles, any use of EC pills was found to be two to seven times greater among women who received an advance supply of EC pills. However, four randomized controlled trials did not show a significant reduction in unintended pregnancy over 12 months when advance provision was compared with standard provision of EC (risk ratio =0.9, 95% confidence interval: 0.69–1.18).Citation62
Legislation to expand access in pharmacies
Since the late 1990s, individual states have taken different paths to expand access to EC.Citation63 In the early stages of access, it was limited to women who had been sexually assaulted. Whereas levonorgestrel EC is now available OTC, UPA remains available by prescription only. Although access to oral EC has expanded in many ways, access remains restrictive in some areas. Legislation to expand pharmacist-prescribing authorities in individual states can help increase access to both OTC and prescription EC products. Some states have regulations for pharmacists’ (or pharmacies’) right to refusal based on moral or ethical grounds. Legislation at the state level can ensure patient access is prioritized while respecting individual beliefs whenever possible.
Pharmacist counseling practices
Community pharmacists can help promote IUD use for EC by providing accurate information, dispelling myths, such as increased risk of pelvic inflammatory disease (associated with the no longer-available Dalkon Shield), and counseling about the risks and benefits. Pharmacists can further help by being familiar with local providers that can place IUDs in a timely manner. The aforementioned UK pilot program, in which trained community pharmacists evaluated women for EC IUD eligibility and referred if appropriate nearly, tripled the uptake of this EC method.Citation61 Community pharmacists in the US are in a prime position to provide EC counseling. Given its safety, efficacy, and cost-effectiveness, the copper IUD should be included in all discussions of possible EC options if feasible and appropriate. See for counseling points for EC.
Table 4 Patient counseling points for EC
Conclusion
Use of EC is increasing over time, due to the wider availability and accessibility of EC methods. Levonorgestrel EC is available OTC without any restriction. Further, in eight states, pharmacists are able to prescribe and provide oral EC directly to women. Pharmacists play a critical role to access to EC in community pharmacies by ensuring product availability in the inventory, up-to-date knowledge, and patient counseling. There are opportunities to expand access to EC in pharmacies further by implementing legislation expanding pharmacist scope of practice, ensuring third-party reimbursement for clinical services delivered by pharmacists, and including EC in pharmacy education and training.
Disclosure
SR is on the clinical advisory board for Afaxys Inc. The other authors report no conflicts of interest in this work.
References
- FinerLBZolnaMRDeclines in unintended pregnancy in the United States, 2008–2011N Engl J Med2016374984385226962904
- JonesRKDarrochJEHenshawSKContraceptive use among U.S. women having abortions in 2000–2001Perspect Sex Reprod Health200234629430312558092
- TrussellJContraceptive failure in the United StatesContraception201183539740421477680
- DanielsKJonesJAbmaJUse of emergency contraception among women aged 15–44: United States, 2006–2010NCHS Data Brief201311218
- MartinezGMAbmaJCSexual activity, contraceptive use, and childbearing of teenagers aged 15–19 in the United StatesNCHS Data Brief201520918
- YenSParmarDDLinELAmmermanSEmergency contraception pill awareness and knowledge in uninsured adolescents: high rates of misconceptions concerning indications for use, side effects, and accessJ Pediatr Adolesc Gynecol201528533734226148784
- TrussellJSchwarzEBEmergency contraceptionHatcherRATrussellJNelsonALCatesWKowalDPolicarMSContraceptive Technology20th edAlpharetta (GA)Bridging the Gap Communications2011113146
- No authors listedPractice bulletin no. 152: emergency contraceptionObstet Gynecol20151263e1e1126287787
- TrussellJRaymondEGClelandKEmergency contraception: a last chance to prevent unintended pregnancy2016 Available from: http://ec.princeton.edu/questions/ec-review.pdfAccessed July 20, 2016
- PiaggioGKappNvon HertzenHEffect on pregnancy rates of the delay in the administration of levonorgestrel for emergency contraception: a combined analysis of four WHO trialsContraception2011841353921664508
- WoodAJDrazenJMGreeneMFA sad day for science at the FDAN Engl J Med2005353121197119916141387
- SampsonONavarroSKKhanABarriers to adolescents’ getting emergency contraception through pharmacy access in California: differences by language and regionPerspect Sex Reprod Health200941211011819493220
- WilkinsonTAFaheyNSutherECabralHJSilversteinMAccess to emergency contraception for adolescentsJAMA2012307436236322182591
- MooreAStammCBorgeltLSeeking emergency contraception in Denver, CO: a health impact assessment2014 Available from: http://www.ucdenver.edu/academics/colleges/medicalschool/departments/medicine/GIM/education/PrimaryCare/Documents/Resident%20Research/2014-MooreA-EmergencyContraception-Poster.pdfAccessed January 30, 2017
- GaffaneyMSecor-TurnerMStammCOutdated counseling in the pharmacy? A qualitative analysis of emergency contraception access in WyomingJ Pediatr Adolesc Gynecol2016292177178
- BaturPClelandKMcNamaraMWuJPickleSEmergency contraception: a multispecialty survey of clinician knowledge and practicesContraception201693214515226363429
- MillerMKPlantzDMDowdMDPediatric emergency health care providers’ knowledge, attitudes, and experiences regarding emergency contraceptionAcad Emerg Med201118660561221676058
- ReedJLVaughnLMPomerantzWJAttitudes and knowledge regarding emergency contraception among emergency department adolescents and providersPediatr Emerg Care201228877577922858752
- WallaceJLWuJWeinsteinJGorenfloDWFettersMDEmergency contraception: knowledge and attitudes of family medicine providersFam Med200436641742215181554
- LawrenceRERasinskiKAYoonJDCurlinFAObstetrician-gynecologist physicians’ beliefs about emergency contraception: a national surveyContraception201082432433020851225
- HellerstedtWLVan RiperKKEmergency contraceptive pills: dispensing practices, knowledge and attitudes of South Dakota pharmacistsPerspect Sex Reprod Health2005371192415888399
- BennettWPetraitisCD’AnellaAMarcellaSPharmacists’ knowledge and the difficulty of obtaining emergency contraceptionContraception200368426126714572889
- HopkinsDWestDArkansas pharmacists’ perceptions toward emergency contraception and nonprescription Plan BPharm Pract20086298102
- FuentesECAzize-VargasYKnowledge, attitudes and practices in a group of pharmacists in Puerto Rico regarding emergency contraceptionP R Health Sci J200726319119718035810
- FrenchACKaunitzAMPharmacy access to emergency hormonal contraception in Jacksonville, FL: a secret shopper surveyContraception200775212613017241842
- El-IbiarySYRaineTMcIntoshJDarneyPDHarperCCPharmacy access to emergency contraception: perspectives of pharmacists at a chain pharmacy in San FranciscoJ Am Pharm Assoc (2003)200747670271018032132
- SommersSDChaiyakunaprukNGardnerJSWinklerJThe emergency contraception collaborative prescribing experience in Washington StateJ Am Pharm Assoc (Wash)2001411606611216115
- BorregoMEShortJHouseNGupchupGNaikRCuellarDNew Mexico pharmacists’ knowledge, attitudes, and beliefs toward prescribing oral emergency contraceptionJ Am Pharm Assoc (2003)2006461334316529339
- RichmanARDaleyEMBaldwinJKromreyJO’RourkeKPerrinKThe role of pharmacists and emergency contraception: are pharmacists’ perceptions of emergency contraception predictive of their dispensing practices?Contraception201286437037522386228
- RaglandDPayakachatNOunpraseuthSPateAHarrodSOttREmergency contraception counseling: an opportunity for pharmacistsJ Am Pharm Assoc (2003)201151675676422068198
- RaglandDPayakachatNStaffordREmergency contraception counseling in a retail pharmacy setting; a pilot studyJ Pharm Pract201528326126524429294
- GlasierACameronSTBlitheDCan we identify women at risk of pregnancy despite using emergency contraception? Data from randomized trials of ulipristal acetate and levonorgestrelContraception201184436336721920190
- US Food and Drug AdministrationPlan B (0.75 mg levonorgestrel) and Plan B one-step (1.5 mg levonorgestrel) tablets information2016 Available from: http://www.fda.gov/Drugs/DrugSafety/Postmarket-DrugSafetyInformationforPatientsandProviders/ucm109775.htmAccessed January 30, 2017
- FinePMathéGindeSCullinsVMorfesisJGainerEUlipristal acetate taken 48–120 hours after intercourse for emergency contraceptionObstet Gynecol20101152 Pt 125726320093897
- StrattonPHartogBHajizadehNA single mid-follicular dose of CDB-2914, a new antiprogestin, inhibits folliculogenesis and endometrial differentiation in normally cycling womenHum Reprod20001551092109910783359
- KimABridgemanMBUlipristal acetate (Ella): a selective progesterone receptor modulator for emergency contraceptionP T201136632533121785549
- HRA PharmaHRA Pharma and Afaxys join forces on emergency contraceptive Ella® in the USA2014 Available from: http://www.hra-pharma.com/index.php/en/you_are/media/hra_pharma_and_afaxys_join_forces_on_emergency_contraceptive_ella_in_the_usaAccessed April 7, 2016
- Afaxys, IncAfaxys announces wider national availability of Ella® emergency contraceptive2014 Available from: http://www.afaxys.com/news-and-media/emergency-contraceptive.phpAccessed April 7, 2016
- BullockHSteeleSKurataNPharmacy access to ulipristal acetate in Hawaii: is a prescription enough?Contraception201693545245426689477
- BrantAWhiteKMariePStPharmacy availability of ulipristal acetate emergency contraception: an audit studyContraception2014903338339
- Ella® (ulipristal acetate) [prescribing information]Charleston (SC)Afaxys Inc2015
- PRJKT Ruby [website on the Internet] https://www.prjktruby.comAccessed April 7, 2016
- LippesJMalikTTatumHJThe postcoital copper-TAdv Plan Parent19761112422976578
- American College of Obstetricians and GynecologistsPractice bulletin no. 121: long-acting reversible contraception: implants and intrauterine devicesObstet Gynecol2011118118419621691183
- DeanGSchwarzEDIntrauterine contraceptionHatcherRATrussellJNelsonALCatesWStewartFKowalDPolicarMSContraception Technology20th edAlpharetta (GA)Bridging the Gap Communications2011
- TurokDKSandersJNThompsonISRoyerPAEggebrotenJGawronLMPreference for and efficacy of oral levonorgestrel for emergency contraception with concomitant placement of a levonorgestrel IUD: a prospective cohort studyContraception201693652653226944863
- RiveraRYacobsonIGrimesDThe mechanism of action of hormonal contraceptives and intrauterine contraceptive devicesAm J Obstet Gynecol19991815 Pt 11263126910561657
- StanfordJBMikoljckykRTMechanisms of action of intrauterine devices: update and estimation of post-fertilization effectsAm J Obstet Gynecol200218761699170812501086
- ClelandKHaopingZGoldstruckNChengLTrussellJThe efficacy of intrauterine devices for emergency contraception: a systematic review of 35 years of experienceHum Reprod2012271994200022570193
- TurokDKGodfreyEMWojdylaDDermishATorresLWuSVCopper T380 intrauterine device for emergency contraception: highly effective at any time in the menstrual cycleHum Reprod201328102672267623945595
- YoostJUnderstanding benefits and addressing misperceptions and barriers to intrauterine device access among populations in the United StatesPatient Prefer Adherence2014894795725050062
- Kaiser Family FoundationIntrauterine devices (IUDs): access for women in the U.S.2016 Available from: http://kff.org/womens-health-policy/fact-sheet/intrauterine-devices-iuds-access-for-women-in-the-usAccessed March 26, 2016
- LuchowskiATAndersonBPowerMLRaglanGBEspeyESchulkinJObstetrician-gynecologists and contraception: practice and opinions about the use of IUDs in nulliparous women, adolescents and other patient populationsContraception201489657257724679477
- Committee on Gynecologic Practice Long-Acting Reversible Contraception Working GroupCommittee opinion no. 642: increasing access to contraceptive implants and intrauterine devices to reduce unintended pregnancyObstet Gynecol20151264e44e4826393458
- OttMASucatoGSContraception for adolescentsPediatrics20141344e1257e128125266435
- HouleSKGrindrodKAChatterleyTTsuyukiRTPaying pharmacists for patient care: a systematic review of remunerated pharmacy clinical care servicesCan Pharm J20141474209232
- ThompsonCACMS explains Medicare payment for chronic care management servicesAm J Health Syst Pharm201572751451525788502
- HigginsSJHattinghHLRequests for emergency contraception in community pharmacy: an evaluation of services provided to mystery patientsRes Social Adm Pharm20139111411922554398
- QueddengKChaarBWilliamsKEmergency contraception in Australian community pharmacies: a simulated patient studyContraception201183217618221237344
- BellDLCamachoEJVelasquezABMale access to emergency contraception in pharmacies: a mystery shopper surveyContraception201490441341525081865
- ClementKMMansourDJImproving uptake of the copper intrauterine device for emergency contraception by educating pharmacists in the communityJ Fam Plann Reprod Health Care2014401414523645564
- RodriguezMICurtisKMGaffieldMLJacksonEKappNAdvance supply of emergency contraception: a systematic reviewContraception201387559060123040139
- Guttmacher InstituteEmergency contraception Available from: https://www.guttmacher.org/state-policy/explore/emergency-contraceptionAccessed April 25, 2016
- OrtizMECroxattoHBCopper-T intrauterine device and levonorgestrel intrauterine system: biological bases of their mechanism of actionContraception2007756 SupplS16S3017531610
- RafieSMcIntoshJGardnerDKOver-the-counter access to emergency contraception without age restriction: an opinion of the Women’s Health Practice and Research Network of the American College of Clinical PharmacyPharmacotherapy201333554955723450827
- Princeton UniversityHistory of Plan B OTC Available from: http://ec.princeton.edu/pills/planbhistory.htmlAccessed April 4, 2016