
Abstract
Regulatory T cells (Treg) are generally considered to be significant contributors to tumor escape from the host immune system. Emerging evidence suggests, however, that in some human cancers, Treg are necessary to control chronic inflammation, prevent tissue damage, and limit inflammation-associated cancer development. The dual role of Treg in cancer and underpinnings of Treg diversity are not well understood. This review attempts to provide insights into the importance of Treg subsets in cancer development and its progression. It also considers the role of Treg as potential biomarkers of clinical outcome in cancer. The strategies for monitoring Treg in cancer patients are discussed as is the need for caution in the use of therapies which indiscriminately ablate Treg. A greater understanding of molecular pathways operating in various tumor microenvironments is necessary for defining the Treg impact on cancer and for selecting immunotherapies targeting Treg.
Introduction
In cancer, regulatory T cells (Treg) appear to play an important, although somewhat controversial, role. In many human cancers and in most mouse models of tumor growth, the frequency of Treg and their suppressor functions are increased as compared to those reported for healthy subjects.Citation1–Citation3 Despite the general perception that Treg accumulations in cancer predict poor outcome,Citation4–Citation6 several reports have indicated that Treg numbers and activity are associated with improved prognosis.Citation7–Citation11 While the role of Treg in tumor growth, progression to metastasis, and the disease outcome continues to be debated, there is considerable experimental and clinical evidence in favor of Treg being engaged in suppression of antitumor immune responses and thus contributing to tumor escape from the host immune system.Citation11,Citation12
Treg are called upon to mediate suppression when immune cells activated by endogenous or exogenous agents threaten to destroy tissues or when a progressing tumor actively recruits and programs Treg to downregulate antitumor immune responses.Citation13,Citation14 The potential of Treg utilization either for protection from tissue damage by activated T cells or for aggression against antitumor effector immune cells has led to a more extensive consideration of mechanisms underpinning Treg recruitment to tissue sites. It is known, for example, that Treg express Toll-like receptors (TLRs), and that TLR ligands can regulate functions of Treg, presumably including their migration.Citation15 Treg recruitment to tumor sites is regulated by chemokines produced in the tumor microenvironment (TME) such as, for example, CCL22, a ligand for CCR4.Citation16 Activated Treg express several chemokine receptors (ie, CCR4, CCR5, CCR6, CCR7, and CCR10), which can mediate Treg trafficking to tissue sites.Citation17 In the presence of tumor-derived chemokines, Treg accumulate in the tumor, and once in place, proceed to prevent or blunt antitumor responses of immune cells infiltrating the TME. Thus, Treg which accumulate in situ and in the peripheral circulation of cancer patients can be viewed as one of multiple attempts by the tumor to promote its own escape from the host immune system by silencing antitumor immune effector cells. On the other hand, it seems equally likely that in tumors characterized by extensive inflammatory infiltrates, such as colon or breast cancers, Treg are necessary for control of chronic inflammation, prevention of tissue damage, and limiting of tumor development associated with inflammation.Citation18,Citation19 Interestingly, in patients with colon or breast carcinomas, the presence and frequency of Treg in the tumor are associated with improved prognosis.Citation11,Citation18,Citation20,Citation21 As a result of this potential dual role of Treg in limiting the process of chronic inflammation on the one hand and in promoting tumor escape from immune control on the other, a number of questions have emerged about the mechanisms that regulate these Treg activities. It could be surmised that the frequency and role of Treg in disease outcome depend on the tumor type and “immune signature” the tumor establishes in a given host. Today, the origin and phenotypic characteristics of Treg infiltrating human tumors are not entirely clear, and neither is the mechanism responsible for the apparent “division of labor” among these cells. This ambiguity is fueled by the rapidly emerging evidence for tremendous plasticity and phenotypic as well functional heterogeneity of Treg in man.Citation22,Citation23
Despite rapid progress made in our understanding of how Treg work, many aspects of their interactions with the tumor and other immune or nonimmune cells remain obscured. It is not clear, for example, that Treg found in the TME are the same cells that circulate in the periphery or that their functional repertoire is similar to or different from that of the cells in the peripheral circulation. Overexpression of multiple checkpoint receptors on Treg in the TME suggests that these cells acquire significantly different phenotype and functions once they enter the tumor.Citation24,Citation25 Because of their enhanced capability to suppress antitumor functions of effector T cells (Teff), Treg have been perceived as mediators of tumor escape that need to be unequivocally silenced or eliminated if antitumor functions are to be restored.Citation26,Citation27
The objective of this review is to address those aspects of the Treg biology that provide insights into the importance of Treg in cancer development and its progression. Another objective is to impress upon the reader a degree of caution for the use of Treg as biomarkers of cancer progression and for the use of therapies which indiscriminately ablate Treg. The review provides a rationale for exercising this caution and discusses alternative strategies for monitoring activities of human Treg that are based on the current understanding of their diversity.
Phenotypic characteristics of human Treg
Treg were first described by Sakaguchi et al as a circulating subset of murine CD4+ T cells expressing high levels of CD25 (the interleukin [IL]-2 receptor α chain), which upon adoptive transfers could prevent development of autoimmune disease.Citation28 Today, a high level of CD25 expression still remains one of the defining surface markers of Treg, although CD25 is also expressed by activated conventional T cells (Tconv) with non-regulatory properties. Therefore, it has been suggested that in man, only CD4+CD25hi Treg, which represent 2%–5% of CD25-expressing CD4+ T cells, represent genuine Treg.Citation29 Since the first description of Treg in 1995,Citation28 a number of additional Treg-specifying markers have been proposed, as discussed below, although today, a marker specific for human Treg is yet to be defined.
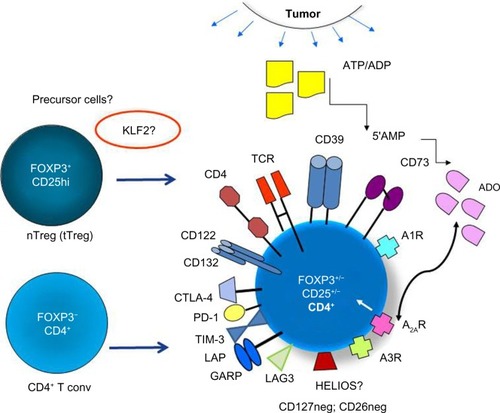
In general, human Treg have been difficult to study for two reasons. First, they represent only a minor subset of CD4+ T cells (about 5%) and thus are only available in a limited number for extensive examinations.Citation2,Citation29 Second, they lack a specific phenotypic marker that could confirm their identity and could facilitate their isolation and characterization. The transcription factor, FOXP3, a reliable Treg marker in mice, is not so reliable in man, for it may be absent from some Treg subsets and present on non-Treg, as recently discussed.Citation30,Citation31 Further, FOXP3 is an intracellular proteinCitation32 that is not expressed on the cell surface, and thus cannot be used for Treg isolation. In the absence of a single marker that defines Treg, various panels of markers have been used to phenotypically distinguish the two major subsets of human Treg, namely naïve (nTreg) or thymus-derived Treg (tTreg) and inducible (iTreg) or peripheral Treg (pTreg). The nomenclature of Treg recently recommended by Abbas et al attempts to classify Treg based on their origin as tTreg or Treg that arise in the periphery by conversion of CD4+ Tconv to T cells mediating suppression.Citation33 While these two Treg subsets share several phenotypic markers in common, they are not phenotypically identical. Specifically, the expression of surface markers such as CD25hi on the cell surface and intracellular FOXP3 has been used to differentiate between these two Treg subsets by flow cytometry, with pTreg exhibiting a much greater heterogeneity in levels of expression of these two markers,Citation34–Citation36 as indicated in . Upregulation on the pTreg surface of checkpoint inhibitory receptors, cytotoxic lymphocyte antigen-4 (CTLA-4), programmed death-1 (PD-1), T cell immunoglobulin mucin-3 (TIM-3), and lymphocyte activation gene-3 (LAG-3), and of transforming growth factor-beta (TGF-β)-associated molecules, latency-associated protein (LAP) and glycoprotein A repetitions predominant (GARP) or co-expression of ectonucleotidases, CD39 and CD73, is a characteristic feature that helps in distinguishing pTreg from tTreg.Citation25,Citation35,Citation37 These features of pTreg are especially evident at tumor sites and are interpreted as evidence of greater ability to mediate suppression.Citation37,Citation38 Further, these phenotypic features appear to emphasize that there is a division of labor among these cell subsets, with tTreg responsible for maintaining tolerance to self and pTreg regulating responses to non-self.Citation27 The absence on the Treg surface of markers such as CD127 or CD26 has often been useful for differentiating Treg from CD4+ Teff.Citation39,Citation40 However, due to Treg plasticity and the possibility that co-expression of certain phenotypic markers distinguishes subsets of Treg with quantitatively different suppressive functions, this differentiation is not simple or easy. In the absence of a single specific, stable marker for Treg, combinations of markers are often used to define Treg.Citation37 This need for the use of multiple marker panels further emphasizes the existence of considerable heterogeneity among human Treg populations.Citation37
Figure 1 The phenotypic profile and potential cellular origins of induced (i)Treg present in the tumor microenvironment.
Abbreviations: Treg, T regulatory cells; nTreg, näive Treg; tTreg, thymus-derived Treg; iTreg, inducible Treg; pTreg, peripheral Treg; 5′AMP, adenosine-5′-monophosphate; ADO, adenosine; CTLA-4, cytotoxic lymphocyte antigen-4; PD-1, programmed death-1; TIM-3, T cell immunoglobulin mucin-3; LAG-3, lymphocyte activation gene-3; TGF-β, transforming growth factor-beta; LAP, latency-associated protein; GARP, glycoprotein A repetitions predominant; NRP-1, Neuropilin-1; ADP, adenosine diphosphate; KLF2, Kruppel-like factor 2; TCR, T cell receptor; ATP, adenosine-5′-triphosphate.
Immunohistochemistry broadly used for Treg detection in formaldehyde-fixed paraffin-embedded human tissues depends entirely on selection of antibodies (Abs) that work well with such specimens, and as discussed elsewhere,Citation12 should not depend on expression of FOXP3 alone, as pTreg present in tumors may be negative for this marker.
Attempting to bring some measure of consensus to the field, a recent international workshop on Treg was organized by the Collaborative Immunoguiding Program.Citation41 The workshop made the following (soon to be published) suggestions regarding the flow cytometry panels to be used for human Treg assessments: a) a minimal definition of human Treg should include CD3, CD4, CD25, CD127, and FOXP3 markers, with an addition of Ki67 and CD45RA to clarify the Treg activation status; b) the sole use of any of the three most commonly used flow panels for the Treg phenotypic definition – 1) [CD25+CD127loFOXP3+ Treg], 2) [FOXP3+HELIOS+ Treg], and 3) [FOXP3hi CD45RAneg vs FOXP3intCD45RA+ to distinguish activated vs nTreg, respectively] – leads to underestimation of the Treg frequency ranging between 25% and 65%.Citation41 The same workshop concluded that CD39 and CTLA-4, which have been described as functional markers on Treg,Citation42,Citation43 denote activated or iTreg and thus are considered as “optional” markers.Citation15
However, a somewhat different view of identifying Treg subsets in cancer patients could be taken based on the observed differences between the phenotype of Treg in healthy donors vs that in patients with cancerCitation34 or between the phenotype of Treg at the tumor site vs that in the patients’ peripheral blood.Citation25–Citation38 Specifically, it appears that in cancer patients, the frequency of pTreg in the blood and tumor tissues is often elevated,Citation2,Citation34 and these accumulating Treg have high expression levels of surface markers associated with suppression such as CD39, CD73, LAP, GARP, COX-2, and others.Citation44,Citation45 These Treg also have intracytoplasmic expression of perforin, granzyme B, and/or IL-10, molecules associated with immune suppression.Citation25,Citation46 Expression by Treg of these “functional” markers is counterbalanced by the presence at tumor sites of Treg co-expressing inhibitory receptors, CTLA-4, PD-1, TIM-3, or LAG-3.Citation23–Citation25,Citation47,Citation48 In aggregate, these observations suggest that pTreg present in the TME may be phenotypically and functionally distinct from tTreg. Therefore, a broader Treg definition, one that allows for the more precise discrimination of tTreg from pTreg in patients with cancer, is needed. As pTreg populations, which likely include subsets of heterogeneous suppressor cells, predominate in cancer,Citation34,Citation45 their localization, numbers, phenotypic signatures, and suppressor functions are of utmost importance. While none of these markers are specific for Treg, when combined with surface CD25hi and/or intracytoplasmic FOXP3, they are useful because they allow for the assessment of the functional potential of Treg by flow cytometry without the need for Treg isolation required for conventional CFSE-based suppressor assays.Citation2,Citation34
More recently, efforts to identify a specific Treg marker that might distinguish tTreg from pTreg have focused on Kruppel-like factor 2 (KLF2), a transcription factor that regulates chronic inflammation and that is necessary for the development of pTreg but not of tTreg.Citation49 This finding not only emphasizes the phenotypic and functional distinction between these Treg subsets but also suggests that discrimination between them may have critical therapeutic implications for selective rather than “global” Treg depletion.
Functional attributes of Treg in patients with cancer
We and many others have commented on elevated suppressor functions mediated by Treg in the peripheral circulation of patients with solid or hematological malignancies.Citation2,Citation26,Citation50,Citation51 In the context of Treg, “suppressor functions” are generally defined as significant inhibition in responder cells of activation (including signaling via activating receptors), proliferation, cytokine/soluble factor production, or of gene expression levels. A number of in vitro assays have been developed to measure suppression mediated by Treg.Citation38,Citation52,Citation53 Some are based on multicolor flow cytometry to measure surface or intracytoplasmic expression levels by Treg of suppression-associated molecules (LAP, GARP, CD39, CD73), as discussed above. These flow-based assays do not require isolation or culture of Treg and thus are commonly used for monitoring of Treg in human specimens. Other assays require coculture of isolated Treg and CFSE-labeled responder T cells, to quantitate levels of suppression mediated by Treg.Citation52,Citation53 In such cocultures, suppression of responder cell activation, proliferation, cytokine production, or gene expression can be quantitatively determined.Citation2,Citation53–Citation55 Still other assays measure FOXP3 demethylation in Treg by MS-qRT-PCR to estimate Treg-specific demethylation region.Citation56 Methodological details for these functional Treg assays can be found in the references.Citation53,Citation54
With a recent more reliable detection and discrimination of Treg in tissues and the peripheral circulation of patients with cancer,Citation57,Citation58 it has become apparent that Treg accumulating in at the tumor site are phenotypically and functionally altered relative to circulating Treg.Citation25,Citation37,Citation48 We have recently reported that expression levels of inhibitory receptors, PD-1, CTLA-4, and TIM-3, as well as of CD39, an enzyme which participates in conversion of adenosine-5′-triphosphate (ATP) to immunosuppressive adenosine (ADO), were significantly elevated in Treg within TIL isolated from human head and neck squamous cell carcinomas (HNSCCs) relative to expression of these markers in paired peripheral blood Treg.Citation25 Others have observed similar upregulated expression of inhibitory receptors on TIL, including Treg, in various other solid tumors. For example, in human non-small-cell lung cancer, a majority of CD4+FOXP3+ TIL also expressed TIM-3,Citation47 and TIM-3+FOXP3+CD4+ Treg preferentially accumulated in the tumor nests in hepatocellular carcinoma.Citation48 Camisaschi et al reported that in melanoma and in colorectal carcinoma, LAG-3+CD4+CD25hiFOXP3+ Treg were preferentially expanded in PBMC as well as in TIL and mediated strong suppressor activity.Citation24 In aggregate, these data suggest that the tumor can induce changes in the receptor profile of Treg thus altering their functions. This may lead to Treg “activation” and upregulation of their suppressor functions or to downregulation of suppression by signaling of the inhibitory receptor expressed on Treg. The implication of these data is that highly suppressive Treg accumulating in the TME may need to be “restrained” via the upregulation of inhibitory checkpoint receptors from excessive suppression that might interfere with immunologic homeostasis.Citation59 Alternatively, it has been suggested that, in contrast to functional blockade induced by signals delivered via checkpoint receptors to all other immune cells, iTreg induction, proliferation, and suppressive functions are promoted by checkpoint receptor engagement.Citation23 Thus, co-expression of “activation” markers and inhibitory receptors on pTreg in the peripheral circulation of cancer patients, and especially at tumor sites,Citation60,Citation61 emerges as an important surrogate marker for Treg functions, and as such, should be included in monitoring of Treg.
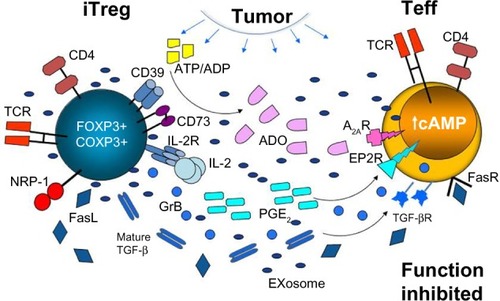
The emerging evidence further suggests that in the presence of tumor-derived signals, Treg might be regulated to preferentially use specific inhibitory molecular pathways.Citation37 As previously discussedCitation37 and illustrated in , Treg are known to utilize a variety of mechanisms for mediating suppression.Citation46,Citation55,Citation62–Citation64 However, it is unclear whether all Treg are capable of perusing these different mechanisms or whether Treg subsets specializing in one type of suppression exist. Therefore, it may be reasonable to envision the scenario where different solid tumors create microenvironments in which Treg are instructed to preferentially adopt the suppression pathway that best fits with environmental programming in situ. For example, HNSCCs are known to express COX-2 and secrete PGE2, which signals via four prostaglandin E receptors expressed on immune (as well as other) cells, upregulating 3′,5′-cyclic adenosine monophosphate (3′,5′-cAMP) levels in responder cells and thus inducing immune suppression.Citation45,Citation65 We have shown that human CD4+CD25neg T cells cocultured in the presence of COX-2+ HNSCC cells differentiated into highly suppressive FOXP3+COX-2+ Treg, which produced PGE2 and other suppressive factors.Citation45 In contrast, COX-2neg HNSCC induced Treg with a significantly lower expression of inhibitory receptors and lower output of immunosuppressive factors.Citation45 The TME of most tumors is enriched in ATP, and the ability of accumulating CD4+CD39+ Treg to hydrolyze ATP to AMP and then, upon upregulation of CD73, to ADO likely represents one of the most common mechanisms of tumor-induced immunosuppression. Expression on the Treg surface of markers such as LAP and GARP suggests the involvement of the TGF-β pathway in tumor-induced suppression by Treg, which is common for cancers producing this cytokine, for example, HNSCCsCitation66 (our unpublished data). These examples illustrate how human tumors regulate suppressive functions of Treg that are recruited to the TME.
Figure 2 Treg accumulating in the TME (activated iTreg) utilize various suppressive mechanisms to inhibit functions of Teff.
Abbreviations: Treg, T regulatory cells; TME, tumor microenvironment; iTreg, inducible Treg; Teff, T effector cells; IL, interleukin; ADO, adenosine; TGF-β, transforming growth factor-beta; GrB, granzyme B; NRP-1, Neuropilin-1; ATP, adenosine-5′-triphosphate; ADP, adenosine diphosphate; TCR, T cell receptor; cAMP, cyclic adenosine monophosphate.
The ADO-PGE2 pathway and Treg-mediated suppression
ADO is a well-known mediator of diverse regulatory processes in the endocrine, vascular, neurological, renal, pulmonary, and immunological systems.Citation67,Citation68 It plays a key role in various diseases, including cancer, chronic inflammation, infections, and autoimmune disorders.Citation45,Citation67 Exogenous ADO is a product of ATP hydrolysis by two ectoenzymes acting in sequence: CD39, an ectonucleoside triphosphate diphospho-hydrolase-1, which hydrolyzes ATP to ADP and AMP, and CD73, an ecto-5′-nucleotidase which catalyzes AMP conversion to ADO. Signaling via its four surface G-protein-coupled receptors, A1, A2A, A2B, and A3 which are widely distributed throughout tissues, ADO mediates regulatory effects via up- or downregulation of intracellular levels of 3′,5′-cAMP. Expression of CD39 and CD73 on Treg was first reported by Borsellino et alCitation69 and Deaglio et alCitation70 in 2007. Since then, we have studied the ability of human Treg to produce ADO and showed that in vitro-generated, cultured iTreg (the so-called Tr1 cells) upregulated surface expression of CD73, co-expressed CD39 and CD73, efficiently hydrolyzed ATP to 5′-AMP and ADO, secreted copious levels of ADO, and mediated suppression of Teff functions via the A2A R engagement.Citation55 In contrast, nTreg, which expressed CD39 but not CD73 on the cell surface, mainly produced 5′-AMP and produced ADO only when co-incubated with CD4+CD73+ T cells, CD73+ B cells, or tumor-derived exosomes, which carried membrane-tethered CD39 and CD73.Citation71 In contrast to CD4+ Teff, human Treg express little if any CD26, which is linked to ADO deaminase at the cell surface, and thus are inefficient in converting ADO to inosine.Citation72 Increased pericellular levels of ADO in Treg might facilitate autocrine signaling, potentially augmenting their suppressor activity. As the A2AR is expressed on Treg, ADO generated by Treg could signal via this ADO receptor to promote Treg functions.Citation72 These data suggest that the ADO pathway may not only be important for Treg proliferation and Treg-mediated suppression of other immune cells expressing ADO but, via its autocrine activity, might also play a key role in the upregulation of Treg suppressor functions.Citation72
In the immune system, ADO inhibits functions of immune cells and is considered to be a powerful anti-inflammatory factor.Citation65,Citation67,Citation68 In cancer, however, in addition to promoting migration of immune cells to the tumor and inhibiting antitumor functions of accumulating Teff, ADO promotes differentiation, expansion, and suppressor activity of Treg and myeloid-derived suppressor cells (MDSCs).Citation73,Citation74 As recently discussed, the ADO pathway in the TME ceases to be a protective pathway guarding against tissue damage by activated immune cells and becomes a tool for suppressing antitumor immune functions, and through its effects on the vasculature, for promoting metastasis.Citation37,Citation65 Importantly, as indicated above, these pro-tumor activities of Treg occur in cooperation with the tumor-driven PGE2 pathway,Citation72 as the ADO and PGE2 pathways converge at the adenylate cyclase, upregulating its activity and thus 3′,5′-cAMP levels in responder cells. Together, these two factors deliver powerful immunoinhibitory signals to antitumor responder cells.
Treg as potential biomarkers in cancer
The ADO/PGE2 pathway operating in the TME and discussed above is but one example of strategies that tumors employ in an attempt to utilize Treg for silencing of antitumor responses. Other mechanisms of suppression exercised by Treg include production of inhibitory cytokines (IL-10, TGF-β),Citation66,Citation75,Citation76 Fas/FasL-dependent apoptosis of activated CD8+ T cells,Citation46 or the engagement of the Neuropilin/semaphorin-4a pathway.Citation76,Citation77 Accumulations of Treg as well as MDSC in human tumors and their increased frequency in the circulation of cancer patients have been widely reported.Citation1–Citation3,Citation74 Many reports, but not all, link these accumulations of CD4+FOXP3+CD25hi Treg to poor prognosis due to suppression of antitumor responses by the accumulating Treg.Citation4–Citation11 Notably, in human colorectal cancer and in breast cancer, the presence and density of FOXP3+ Treg have been reported to predict favorable outcome and a better locoregional control of the tumor.Citation18,Citation20 Also, in human lymphomas, elevated circulating Treg predict better outcome.Citation8–Citation10 Thus, Treg frequency in the tumor or in the periphery is a potentially important prognostic biomarker in cancer. Treg enumeration and characterization in situ could provide important clues about the tumor’s immune signature, which currently is becoming recognized as an important prognostic factor in various human solid tumors.Citation79 As the TME is created and maintained by the tumor, phenotypic and functional characterization of Treg among TIL and in the peripheral circulation of patients with cancer might inform us about tumor itself, especially its aggressiveness or propensity to metastasize. Given recent emphasis on the tumor immune signature and emerging correlations of immunohistochemistry data to cancer patients’ survival,Citation79,Citation80 the phenotypic, and especially functional, characterization of Treg in situ assumes a new and potentially important role in establishing the prognostic significance of Treg. While Treg significance as a prognostic marker is best established in colorectal carcinoma,Citation81 investigations are in progress to extend and confirm these findings to other solid tumors.
Based on measures of the magnitude of immune response silencing by Treg in cancer (ie, Treg suppressor functions) rather than their phenotype in situ or in the peripheral circulation, it might be possible to arrive at an even better estimate of Treg prognostic significance. Similarly, measures of Treg functions might correlate better with responses to oncological therapies than does their phenotypic enumeration. However, because Treg are heterogeneous, consisting of many subsets of functionally distinct cells, and because no universal distinguishing marker for Treg is currently available, their use as a biomarker of prognosis is limited and has to be taken with caution. Furthermore, current attempts to therapeutically deplete Treg might enhance tumor immunity in some patients but be detrimental in others.Citation1,Citation7 It is necessary to remember that most of the studies examining the association of the Treg phenotype with prognosis or response to therapies were based on the use of FOXP3 as a “specific” Treg marker.Citation20 However, a recent comprehensive review of the prognostic significance of FOXP3+ T cells in 16 nonlymphoid cancers suggested that FOXP3 by itself is not a reliable marker of human Treg and that the tumor site, that is, the TME, has a major impact on biologic effects of FOXP3+ Treg.Citation30 Overall, the prognostic value of Treg in cancer remains questionable, although it is possible that introduction in the future of more specific high-throughput assays for Treg might provide a more discriminating approach for evaluating their value as surrogate markers of prognosis, outcome, or response to therapy.
It has been reported that expression of surface markers on Treg can be altered in diseaseCitation82 and in patients undergoing conventional therapies or immune therapies.Citation82–Citation84 Therefore, the selection of a panel of markers for measuring Treg is a critical task that will ultimately determine the Treg role as biomarkers of prognosis in cancer and other disease. As discussed earlier, there is still no consensus as to which marker panel (of several available) is best, and which subset of Treg should be monitored. Focusing on one functional subset, for example, on the CD4+CD39+CD25+ ADO-producing Treg, as is done in the author’s laboratory, may be limiting in scope but offers an advantage of following disease-associated changes in this subset of Treg and correlating these changes to disease progression.Citation85
Therapeutic approaches to eliminating Treg-induced suppression
If Treg play a role in promoting tumor escape, as suggested by many in vitro and in vivo studies, then elimination or silencing of Treg becomes a desirable therapeutic objective. Indeed, a considerable body of recent literature deals with various methods for Treg depletion.Citation86–Citation91 Treg express surface molecules that can be specifically targeted by Abs or pharmacologic inhibitors. lists the Treg-associated molecules that potentially could be targeted for Treg silencing either by Treg removal or impairment of Treg suppressor functions. To date, a variety of agents, including Abs (daclizumab: anti-CD25 Ab), IL-2 fusion toxins such as denileukin diftitox (Ontak), or drugs such as cyclophosphamide or tyrosine kinase inhibitors (sunitinib), have been tested in preclinical in vitro studies with human cells.Citation87–Citation91 Many in vivo studies in animal models of cancer have been performed testing for efficiency in depleting Treg.Citation86 Advantages and disadvantages of these depletion strategies have been extensively reviewed.Citation86
Table 1 Potential molecular targets for therapeutic depletion or re-programming of human Treg
Based on favorable preclinical results, some depletion strategies are being used alone or in combination with immunotherapies in human clinical trials (). The table lists clinical trials posted online at http://www.clinicaltrials.gov that have utilized one or more Treg-depleting strategies presented in . However, in contrast to successful and meaningful Treg depletion studies in mouse models, it has not been possible to convincingly correlate Treg depletion by these agents with clinical benefits in patients with cancer.Citation92 This may be due to inadequate depletion efficacy of the drugs, innate resistance of Treg to certain drugs, selective sensitivity of some but not all Treg subsets to the drugs being used, or the ability of the host to rapidly re-populate the depleted Treg. Recent experiments support the notion that not all Treg are the same, and that Treg mediating antitumor responses (ie, iTreg) represent a unique subset or subsets of CD4+ T cells with properties distinct from those of Treg responsible for mediating tolerance to self-antigens.Citation93 This argues against the concept of a “global” Treg depletion (eg, with high-dose cyclophosphamide) and for the use of more selective depletion strategies that would protect Treg-regulating autoimmunity and eliminate those that mediate suppression of antitumor immunity.Citation86,Citation94 However, because the phenotypic distinction between tTreg and iTreg is blurred at this time, it may be difficult to selectively target one Treg subset in preference of another. Surprisingly, there is evidence that CD4+CD25+FOXP3+CD45RA+ Treg were not altered by daclizumab administered prior to an antitumor vaccine in patients with breast cancer, while the depletion of CD4+CD25+FOXP3+CD45RAneg Treg has led to selective re-population of the partly depleted Treg compartment with re-programmed or newly minted CD4+IFN-γ+ T cells that no longer mediated suppression.Citation95 These studies suggest that interference with the Treg compartment by the Treg-depleting therapies may profoundly alter properties of Treg subsets, leading to re-population with T-cell subsets showing unexpected characteristics. In this context, our cross-sectional studies of patients with HNSCC treated with the standard-of-care chemoradiotherapy (CRT) showed that in a substantial proportion of these patients, circulating Treg become more resistant to CRT than conventional CD4+ Teff cells, persist for prolonged time periods in the circulation, upregulate expression of pro-survival molecules Bcl-2 and Bcl-xL, and might contribute to depressed antitumor immunity potentially associated with cancer recurrence.Citation85 Although effects of conventional or immune therapies on the Treg frequency and functions remain a subject of contention, it appears that much of this controversy arises from the tremendous plasticity of Treg, which in cancer is almost certainly orchestrated by the presence of the tumor and of various tumor-derived factors.
Table 2 Immunotherapy clinical trials incorporating strategies for Treg depletion in patients with solid or hematologic malignancies
In view of the existence of multiple inhibitory pathways in the TME, such as the ADO/PGE2, TGF-β, IL-2/IL-2R, and Neuropilin-1/semaphorin-4a pathways,Citation44,Citation76,Citation77,Citation96 and emerging evidence that Treg might selectively utilize these pathways for mediating immune suppression, the strategy of “blocking the inhibitors” with neutralizing Abs or pharmacologic inhibitors has been considered.Citation97 The strategy is based on the inhibitor ability to antagonize negative signaling ongoing between iTreg and Teff, and it calls for the delivery to patients of Abs or pharmacologic agents specific for key components of an inhibitory pathway operating in the TME and responsible for tumor-induced suppression.Citation97 The difficulty is to a priori discern which of the multiple inhibitory pathways plays a key role in immune escape of a given tumor. For example, in patients with tumors expressing COX-2 such as HNSCC, which are richly infiltrated with iTreg-producing PGE2, inhibitors of the PGE2 pathway (celecoxib, indomethacin, diclofenac, ibuprofen) have been clinically used with an intent to block immune suppression.Citation45 As ATP levels are generally high in the TME of human solid tumors,Citation98 and as tumor-associated iTreg overexpress CD39 and CD73 producing lots of ADO,Citation71 it is safe to predict that antagonizing this pathway at the ectoenzyme or the A2AR level would effectively reduce or eliminate ADO-mediated suppression. This approach has been shown to work both in vitro with human Treg–Teff coculturesCitation71 and in preclinical models of cancer.Citation99,Citation100 It is important to remember that antagonistic drugs or Abs with specificity for an antigen present on Treg and on tumor cells, as is the case with CD39 and CD73 ectonucleotidases, for example, will target not only Treg but also tumor cells, potentially amplifying their effectiveness. An additional benefit of antagonizing ADO-induced suppression may derive from the fact that it involves blocking of Treg suppressor functions without depletion of all Treg and risking the development of autoimmunity.Citation101
Currently, the most widely used strategy for reducing tumor-induced immune suppression is the immune checkpoint blockade with Abs specific for CTLA-4, PD-1, or PD-L1.Citation102,Citation103 The targeted molecules are negative inhibitors of immune responses mediated by activated Teff. However, Treg, especially those present in the TME, are known to express a variety of the same regulatory molecules.Citation24,Citation25 Therefore, it has been suggested that in addition to blocking negative signaling in Teff, the checkpoint blockade with, for example, anti-CTLA-4 (ipilimumab) or anti-PD-1 (nivolumab) Abs also eliminates Treg by a mechanism referred to as antibody-dependent cellular cytotoxicity (ADCC).Citation104 There is recent evidence that in vitro targeting of CTLA-4+ Treg with ipilimumab reduces suppression exerted by Treg on natural killer cells, which are now able to mediate ADCC and thus potentiate antitumor functions of ipilimumab.Citation64 The reported antitumor efficacy of checkpoint-blocking Abs in human clinical trials may be related to inhibition of activated T cells and also to the Ab-driven elimination of iTreg. The potential of ipilimumab for elimination of CTLA-4+ Treg is especially intriguing in view of current reports that some monoclonal Abs used for cancer therapy, for example, cetuximab approved for treatment of HNSCC, actually increase the frequency and suppressor functions of Treg and that these increases can be related with poor prognosis.Citation64 This would argue for a combination of cetuximab and ipilimumab in the future to improve antitumor effectiveness of immunotherapy.Citation64 As these cellular mechanisms of Ab cancer immunotherapy are potentially related to the observed clinical responses and outcome in patients with cancer, they remain under intense scrutiny.
Summary
The presence and functions of human Treg in cancer have been intensively investigated. Nevertheless, the role that these suppressor cells play in cancer progression remains controversial. It appears that while contributing to tumor escape from the host immune system, Treg are also involved in regulating immune responses to self and controlling inflammatory responses that threaten to disrupt tissue integrity. This small subset of CD4+ T cells is endowed with a remarkable characteristic of plasticity that allows Treg to rapidly respond to recruiting stimulatory signals by trafficking to sites requiring their interventions, rapid expansion, overexpression of surface receptors involved in their functions, and conversion to highly effective regulatory cells that can act in a paracrine as well as an autocrine manner. It appears that in cancer, expansion and activation of Treg occur in response to tumor-generated signals, leading to tumor escape. The remarkable plasticity of Treg infiltrating human tumors is reflected in their phenotypic and functional heterogeneity that may influence disease outcome. It appears that genetic and environmental factors promote variability in the expression of Treg cell signature genes,Citation10 so that Treg gene repertoire differs between individuals. If so, then Treg involvement in human cancer and other diseases will have to be viewed in the light of personalized medicine.Citation108
Recent insights into Treg accumulating at tumor sites and in the peripheral circulation of patients with cancer indicate that Treg responding to environmentally generated stimuli participate in already existing inhibitory molecular pathways, which characterize the TME created by a given tumor.Citation37 At the same time, Treg entering a TME rich in activated inflammatory cells can regulate inflammation, decreasing the potential for pro-tumor effects.Citation105 A better understanding of molecular pathways operating in the TME is needed to be able to discriminate “bad” Treg (promote tumor escape) from “good” Treg (restrict destructive chronic inflammation). This concept underlies the use of Treg as bio-markers of tumor progression and the selection of therapeutic strategies for Treg elimination to help restore antitumor immunity in cancer. The understanding of Treg diversity is critical for either of these strategies to be successful, and a sustained focus on the molecular pathways that Treg use in the TME is likely to facilitate future progress.
Disclosure
The author reports no conflicts of interest in this work.
References
- MougiakakosDChoudhuryALladserAKiesslingRJohanssonCCRegulatory T cells in cancerAdv Cancer Res20101075711720399961
- StraussLBergmannCGoodingWJohnsonJTWhitesideTLThe frequency and suppressor function of CD4+CD25highFoxp3+ T cells in the circulation of patients with squamous cell carcinoma of the head and neckClin Cancer Res2007136301631117975141
- WolfAMWolfDSteurerMGastlGGunsiliusEGrubeck-LoebensteinBIncrease in regulatory T cells in the peripheral blood of cancer patientsClin Cancer Res2003960661212576425
- CurielTJCoukosGZouLSpecific recruitment of regulatory T cells in ovarian carcinoma fosters immune privilege and predicts reduced survivalNat Med20041094294915322536
- WolfDWolfAMRumpoldHThe expression of T cell-specific forkhead box transcription factor FOXP3 is associated with poor prognosis in ovarian carcinomaClin Cancer Res2005118326833116322292
- DengLZhangHLuanYAccumulation of FOXP3+ T regulatory cells in draining lymph nodes correlates with disease progression and immune suppression in colorectal cancer patientsClin Cancer Res2010164105411220682706
- BadoualCHansSRodriguezJPrognostic value of tumor-infiltrating CD4+ T cell subpopulations in head and neck cancersClin Cancer Res200612246547216428488
- TzankovAMeierCHirschmannPWentPPileriSADirnhoferSCorrelation of high numbers of intratumoral FOXP3+ regulatory T cells with improved survival in germinal center-like diffuse large B-cell lymphoma, follicular lymphoma and classical Hodgkin’s lymphomaHaematologica20089319320018223287
- CarrerasJLopez-GuillermoAFoxBCHigh numbers of tumor-infiltrating FOXP3-positive regulatory T cells are associated with improved overall survival in follicular lymphomaBlood20061082957296416825494
- FarinhaPAl-TourahAGillKKlasaRConnorsJMGascoyneRDThe architectural pattern of FOXP3-positive T cells in follicular lymphoma is an independent predictor of survival and histologic transformationBlood201011528929519901260
- DroeserRZlobecIKilicEDifferential pattern and prognostic significance of CD4+, FOXP3+ and IL-17+ tumor infiltrating lymphocytes in ductal and lobular breast cancersBMC Cancer20121213422471961
- WhitesideTLWhat are regulatory T cells (Treg) regulating in cancer and why?Semin Cancer Biol20122232733422465232
- YamaguchiTWingJBSakaguchiSTwo modes of immune suppression by FoxP39(+) regulatory T cells under inflammatory or non-inflammatory conditionsSemin Immunol20112342443022055883
- WhitesideTLThe tumor microenvironment and its role in promoting tumor growthOncogene2008275904591218836471
- ObergHHJurickeMKabelitzDWeschDRegulation of T cell activation by TLR ligandsEur J Cell Biol20119058259221292344
- YoshieOMatsushimaKCCR4 and its ligands: from bench to bedsideInt Immunol2015271112025087232
- OndondoBJonesEGodkinAGallimoreAHome sweet home: the tumor microenvironment as a haven for regulatory T cellsFront Immunol2013419723874342
- LadoireSMartinFGhiringhelliFPrognostic role of FOXP3+ regulatory T cells infiltrating human carcinomas: the paradox of colorectal cancerCancer Immunol Immunother201160790991821644034
- RechAJMickRKaplanDEChangKMDomchekSMVonderheideRHHomeostasis of peripheral FOXP3(+)CD4(+) regulatory T cells in patients with early and late stage breast cancerCancer Immunol Immunother201059459960719855964
- SalamaPPhillipsMGrieuFTumor-infiltrating FOXP3+ T regulatory cells show strong prognostic significance in colorectal cancerJ Clin Oncol200927218619219064967
- FreyDMDroeserRAViehlCTHigh frequency of tumor-infiltrating FOXP3(+) regulatory T cells predicts improved survival in mismatch repair-proficient colorectal cancer patientsInt J Cancer20101262635264319856313
- DuhenTDuhenRLanzavecchiaASallustoFCampbellDJFunctionally distinct subsets of human FOXP3+ Treg cells that phenotypically mirror effector Th cellsBlood20121194430444022438251
- FranciscoLMSalinasVHBrownKEPD-1 regulates the development, maintenance and function of induced regulatory T cellsJ Exp Med20092063015302920008522
- CamisaschiCCasatiCRiniFLAG-3 expression defines a subset of CD4(+)CD25(high) Foxp3(+) regulatory T cells that are expanded at tumor sitesJ Immunol20101846545655120421648
- JieHBGildener-LeapmanNLiJIntratumoral regulatory T cells upregulate immunosuppressive molecules in head and neck cancer patientsBr J Cancer20131092629263524169351
- WhitesideTLSchulerPSchillingBInduced and natural regulatory T cells in human cancerExpert Opin Biol Ther2012121383139722849383
- AdeegbeDONishikawaHNatural and induced T regulatory cells in cancerFront Immunol2013419023874336
- SakaguchiSSakeguchiNAsanoMItohMTodaMImmunologic self-tolerance maintained by activated T cells expressing IL-2 receptor alpha chains (CD25). Breakdown of a single mechanism of self-tolerance causes various autoimmune diseasesJ Immunol1995155115111647636184
- Baecher-AllanCBrownJAFreemanGJHaflerDACD4+CD25 high regulatory cells in human peripheral bloodJ Immunol20011671245125311466340
- deLeeuwRJKostSEKakalJANelsonBHThe prognostic value of FOXP3+ tumor-infiltrating lymphocytes in cancer: a critical review of the literatureClin Cancer Res2012183022302922510350
- DevaudCDarcyPKKershawMHFoxp3 expression in T regulatory cells and other cell lineagesCancer Immunol Immunother20146386987625063364
- AllanSEPasseriniLBacchettaRThe role of 2FOXP3 isoforms in the generation of human CD4+ TregsJ Clin Invest20051153276328416211090
- AbbasAKBenoistCBluestoneJARegulatory T cells: recommendations to simplify the nomenclatureNat Immunol20131430730823507634
- BergmannCStraussLWangYT regulatory type 1 cells in squamous cell carcinoma of the head and neck: mechanisms of suppression and expansion in advanced diseaseClin Cancer Res2008143706371518559587
- SchulerPJSchillingBHarasymczukMPhenotypic and functional characteristics of CD4+ CD39+ FOXP3+ and CD4+ CD39+ FOXP3neg T-cell subsets in cancer patientsEur J Immunol2012421876188522585562
- deLeeuwRJKroegerDRKostSEChangPPWebbJRNelsonBHCD25 identifies a subset of CD4+FoxP3- TIL that are exhausted yet prognostically favorable in human ovarian cancerCancer Immunol Res2014319
- WhitesideTLInduced regulatory T cells in inhibitory microenvironments created by cancerExpert Opin Biol Ther201414101411142524934899
- StraussLBergmannCSzczepanskiMJLangSKirkwoodJMWhitesideTLExpression of ICOS on human melanoma-infiltrating CD4+CD25highFoxp3+ T regulatory cells: implications and impact on tumor-mediated immune suppressionJ Immunol200818052967298018292519
- MandapathilMSzczepanskiMHarasymczukMCD26 expression and adenosine deaminase activity in regulatory T cells (Treg) and CD4(+) T effector cells in patients with head and neck squamous cell carcinomaOncoimmunology20121565966922934258
- LiuWPutnamALXu-YuZCD127 expression inversely correlates with FOXP3 and suppressive function of human CD4+ Treg cellsJ Exp Med20062031701171116818678
- SantegoetsSDijkgraafEBattagliaAMonitoring regulatory T cells in clinical samples: consensus on an essential marker set and gating strategy for regulatory T cell analysis by flow cytometryIn press2015
- SalomonBLenschowDJRheeLB7/CD28 costimulation is essential for the homeostasis of the CD4+CD25+ immunoregulatory T cells that control autoimmune diabetesImmunity20001243144010795741
- MandapathilMHilldorferBSzczepanskiMJGeneration and accumulation of immunosuppressive adenosine by human CD4+CD25highFOXP3+ regulatory T cellsJ Biol Chem20102857176718619858205
- MandapathilMSzczepanskiMJSzajnikMAdenosine and prostaglandin E2 cooperate in the suppression of immune responses mediated by adaptive regulatory T cellsJ Biol Chem2010285275712758020558731
- BergmannCStraussLZeidlerRLangSWhitesideTLExpansion of human T regulatory type 1 cells in the microenvironment of cyclooxygenase 2 overexpressing head and neck squamous cell carcinomaCancer Res2007678865887317875728
- StraussLBergmannCWhitesideTLHuman circulating CD4+CD25highFoxp3+ regulatory T cells kill autologous CD8+ but not CD4+ responder cells by Fas-mediated apoptosisJ Immunol20091821469148019155494
- GaoXZhuYLiGTIM-3 expression characterizes regulatory T cells in tumor tissues and is associated with lung cancer progressionPLoS One20127e3067622363469
- YanJZhangYZhangJPLiangJLiLZhengLTim-3 expression defines regulatory T cells in human tumorsPLoS One20138e5800623526963
- PabbisettySKRabacalWMasedaDKLF2 is a rate-limiting transcription factor that can be targeted to enhance regulatory T-cell productionProc Natl Acad Sci U S A2014111269579958424979767
- SzczepanskiMJSzajnikMCzystowskaMIncreased frequency and suppression by regulatory T cells in patients with acute myelogenous leukemiaClin Cancer Res2009153325333219417016
- SchmittEGWilliamsCBGeneration and function of induced regulatory T cellsFront Immunol2013415223801990
- RuitenbergJJBoyceCHingoraniRPutnamAGhanekarSARapid assessment of in vitro expanded human regulatory T cells functionJ Immunol Methods20113729510621781972
- CanavanJBAfzaliBScottàCA rapid diagnostic test for human regulatory T cell function to enable regulatory T cell therapyBlood2012119e57e6622219224
- WhitesideTLRegulatory T cell (Treg) assays: repertoire, functions and clinical importance of human TregDetrichBHamiltonRGFoldsJDManual of Molecular and Clinical Laboratory Immunology8th edWashingtonASM PressIn press2015
- WhitesideTLJacksonEKAdenosine and prostaglandin e2 production by human inducible regulatory T cells in health and diseaseFront Immunol2013421223898333
- PolanskyJKSchreiberLThelemannCMethylation matters: binding of Ets-1 to the demethylated Foxp3 gene contributes to the stabilization of Foxp3 expression in regulatory T cellsJ Mol Med (Berl)2010881029104020574810
- KalathilSLugadeAAMillerAIyerRThanavalaYHigher frequencies of GARP(+)CTLA-4(+)Foxp3(+) T regulatory cells and myeloid-derived suppressor cells in hepatocellular carcinoma patients are associated with impaired T cell functionalityCancer Res2013732435244423423978
- JacobsJFIdemaAJBolKFRegulatory T cells and the PD-L1/PD-1 pathway mediate immune suppression in malignant human brain tumorsNeuro Oncol20091139440219028999
- ButtAQMillsKHImmunosuppressive networks and checkpoints controlling antitumor immunity and their blockade in the development of cancer immunotherapeutics and vaccinesOncogene2014334623463124141774
- NirschiCJDrakeCGMolecular pathways: coexpression of immune checkpoint molecules: signaling pathways and implications for cancer immunoatherapyClin Cancer Res2013194917492423868869
- WooSRTurnisMEGoldbergMVImmune inhibitory molecules LAG-3 and PD-1 synergistically regulate T-cell function to promote tumoral immune escapeCancer Res20127291792722186141
- PandiyanPZhengLIshiharaSReedJLenardoMJCD4+CD25+Foxp3+ regulatory T cells induce cytokine deprivation-mediated apoptosis of effector CD4+ T cellsNat Immunol200781353136217982458
- CzystowskaMStraussLBergmannCSzajnikMRabinowichHWhitesideTLReciprocal granzyme/perforin-mediated death of human regulatory and responder T cells is regulated by interleukin-2 (IL-2)J Mol Med (Berl)20108857758820225066
- Hyun-BaeJSchulerPJLeeSCCTLA-4+ regulatory T cells are increased in cetuximab treated head and neck cancer patients, suppress NK cell cytotoxicity and correlate with poor prognosisCancer Res2015
- Muller-HaegeleSMullerLWhitesideTLImmunoregulatory activity of adenosine and its role in human cancer progressionExpert Rev Clin Immunol201410789791424871693
- KumaiTOikawaKAokiNTumor-derived TGF-β and prostaglandin E2 attenuate anti-tumor immune responses in head and neck squamous cell carcinoma treated with EGFR inhibitorJ Transl Med20141226525240937
- AntonioliLBlandizziCPacherPHaskoGImmunity, inflammation and cancer: a leading role for adenosineNat Rev Cancer20131384285724226193
- HaskoGLindenJCronsteinBPacherPAdenosine receptors: therapeutic aspects for inflammatory and immune diseasesNat Rev Drug Discov2008775977018758473
- BorsellinoGKleinewietfeldMDi MitriDExpression of ectonucleotidase CD39 by FoxP3+ Treg cells: hydrolysis of extracellular ATP and immune suppressionBlood20071101225123217449799
- DeaglioSDwyerKMGaoWAdenosine generation catalyzed by CD39 and CD73 expressed on regulatory T cells mediates immune suppressionJ Exp Med20072041257126517502665
- SchulerPJSazeZHongCSHuman CD4(+) CD39(+) regulatory T cells produce adenosine upon co-expression of surface CD73 or contact with CD73(+) exosomes or CD73(+) cellsClin Exp Immunol2014177253154324749746
- MandapathilMWhitesideTLTargeting human inducible regulatory T cells (Tr1) in patients with cancer: blocking of adenosine-prostaglandin E2 cooperationExpert Opin Biol Ther2011111203121421702720
- SzajnikMCzystowskaMSzczepanskiMJMandapathilMWhitesideTLTumor-derived microvesicles induce, expand and up-regulate biological activities of human regulatory T cells (Treg)PLoS One20105e1146920661468
- MarigoIDolcettiLSerafiniPZanovelloPBronteVTumor-induced tolerance and immune suppression by myeloid derived suppressor cellsImmunol Rev200822216217918364001
- ZhouAXKozhayaLFujiiHUnutmazDGarp-TGF-β complexes negatively regulate regulatory T cell development and maintenance of peripheral CD4+ T cells in vivoJ Immunol20131905057506423576681
- WhiteRAMalkoskiSPWangXJTGFβ signaling in head and neck squamous cell carcinomaOncogene2010295437544620676130
- DelgoffeGMWooSRTurnisMEStability and function of regulatory T cells is maintained by a neuropilin-1-semaphorin-4a axisNature201350125225623913274
- ChaudharyBKhaledYSAmmoriBJElkordENeuropilin 1: function and therapeutic potential in cancerCancer Immunol Immunother201463819924263240
- GalonJPagèsFMarincolaFMThe immune score as a new possible approach for the classification of cancerJ Transl Med201210122214470
- FridmanWHGalonJPagèsFTartourESautès-FridmanCKroemerGPrognostic and predictive impact of intra- and peritumoral immune infiltratesCancer Res201171175601560521846822
- NoshoKBabaYTanakaNTumour-infiltrating T-cell subsets, molecular changes in colorectal cancer, and prognosis: cohort study and literature reviewJ Pathol201022235036620927778
- LongSABucknerJHCD4+FOXP3+ T regulatory cells in human autoimmunity: more than a numbers gameJ Immunol20111872061206621856944
- KavanaghBO’BrienSLeeDCTLA4 blockade expands FOXP3+ regulatory and activated effector CD4+ T cells in a dose-dependent fashionBlood200811241175118318523152
- SimGCMartin-OrozcoNJinLIL-2 therapy promotes suppressive ICOS+ Treg expansion in melanoma patientsJ Clin Invest201412419911024292706
- SchulerPJHarasymczukMSchillingBEffects of adjuvant chemoradiotherapy on the frequency and function of regulatory T cells in patients with head and neck cancerClin Cancer Res201319236585659624097865
- ColomboMPPiconeseSRegulatory T-cell inhibition versus depletion: the right choice in cancer immunotherapyNat Rev Cancer2007788088717957190
- MoltedoBHemmersSRudenskyAYRegulatory T cell ablation causes acute T cell lymphopeniaPLoS One20149e8676224466225
- LeDTJaffeeEMRegulatory T-cell modulation using cyclophosphamide in vaccine approaches: a current perspectiveCancer Res201272143439344422761338
- RechAJVonderheideRHClinical use of anti-CD25 antibody daclizumab to enhance immune responses to tumor antigen vaccination by targeting regulatory T cellsAnn N Y Acad Sci200911749910619769742
- BaurASLutzMBSchiererSDenileukin diftitox (ONTAK) induces a tolerogenic phenotype in dendritic cells and stimulates survival of resting TregBlood2013122132185219423958949
- FinkeJHRiniBIrelandJSunitinib reverses type-1 immune suppression and decreases T regulatory cells in renal carcinoma patientsClin Cancer Res200814206674668218927310
- ElkordEAlcantar-OrozcoEMDovediSJT regulatory cells in cancer: recent advances and therapeutic potentialExp Opin Biol Ther20101015731586
- NishikawaHSakaguchiSRegulatory T cells in cancer immunotherapyCurr Opin Immunol2014271724413387
- WhitesideTLDisarming suppressor cells to improve immunotherapyCancer Immunol Immunother20126128328822146892
- RechAJMickRMartinSCD25 blockade depletes and selectively reprograms regulatory T cells in concert with immunotherapy in cancer patientsSci Transl Med20124134134ra62
- ChengGYuAMalekTRT cell tolerance and the multi-functional role of IL-2R signaling in T regulatory cellsImmunol Rev2011241637621488890
- WhitesideTLInhibiting the inhibitors: evaluating agents targeting cancer immunosuppressionExpert Opin Biol Ther2010101019103520415597
- StaggJSmythMJExtracellular adenosine triphosphate and adenosine in cancerOncogene2010305346535820661219
- OhtaAKiniROhtaASubramanianMMadasuMSitkovskyMThe development and immunosuppressive functions of CD4(+) CD25(+) FoxP3(+) regulatory T cells are under influence of the adenosine-A2A adenosine receptor pathwayFront Immunol2012319022783261
- StaggJDivisekeraUMcLaughlinNAnti-CD73 antibody therapy inhibits breast tumor growth and metastasisProc Natl Acad Sci U S A20101071547155220080644
- BastidJCottalorda-RegairazAAlbericiGBonnefoyNEliaouJFBensussanAENTPD1/CD39 is a promising therapeutic target in oncologyOncogene201332141743175122751118
- HodiFSO’DaySJMcDermottDFImproved survival with ipilimumab in patients with metastatic melanomaN Engl J Med201036371172320525992
- BrahmerJRTykodiSSChowLQSafety and activity of anti-PD-L1 antibody in patients with advanced cancerN Engl J Med20123662455246522658128
- CurranMAMontalvoWYahitaHAllisonJPPD-1 and CTLA-4 combination blockade expands infiltrating T cells and reduces regulatory T and myeloid cells with B16 melanoma tumorsProc Natl Acad Sci U S A20101074275428020160101
- WhitesideTLRegulatory T cell subsets in human cancer: are they regulating for or against tumor progression?Cancer Immunol Immunother201463677224213679
- WhitesideTLImmune modulation of T-cell and NK-cell (natural killer) cell activities by TEX (tumor derived exosomes)Biochem Soc Trans20134124525123356291
- ElkordEAl-RamadiBKHelios expression in FoxP3(+) T regulatory cellsExpert Opin Biol Ther2012121423142522827571
- FerraroAD’AliseAMRajTInterindividual variation in human T regulatory cellsProc Natl Acad Sci U S A2014111E1111E112024610777
- LitzingerMTFernandoRCurielTJGrosenbachDWSchlomJPalenaCIL-2 immunotoxin denileukin diftitox reduces regulatory T cells and enhances vaccine-mediated T-cell immunityBlood20071103192320117616639
- PerainoJSZhangHRajasekeraPVDiphtheria toxin-based bivalent human IL-2 fusion toxin with improved efficacy for targeting human CD25(+) cellsJ Immunol Methods2014405576624462799
- SmithALRobinTPFordHLMolecular pathways: targeting the TGF-β pathway for cancer therapyClin Cancer Res2012184514452122711703
- WeberJImmune checkpoint proteins: a new therapeutic paradigm for cancer – preclinical background: CTLA-4 and PD-1 blockadeSemin Oncol20103743043921074057
- PardollDMThe blockade of immune checkpoints in cancer immunotherapyNat Rev Cancer20121225226422437870
- CallahanMKWolchokJDAt the bedside: CTLA-4- and PD-1-blocking antibodies in cancer immunotherapyJ Leukoc Biol201394415323667165
- ChenXBäumelMMännelDNHowardOMOppenheimJJInteraction of TNF with TNF receptor type 2 promotes expansion and function of mouse CD4+CD25+ T regulatory cellsJ Immunol200717915416117579033
- NagarMJacob-HirschJVernitskyHTNF activates a NF-kappaB-regulated cellular program in human CD45RA-regulatory T cells that modulates their suppressive functionJ Immunol20101843570358120181891
- CohenADDiabAPeralesMAAgonist anti-GITR antibody enhances vaccine-induced CD8(+) T-cell responses and tumor immunityCancer Res2006664904491216651447
- LutsiakMESemnaniRTDe PascalisRKashmiriSVSchlomJSabzevariHInhibition of CD4(+)25+ T regulatory cell function implicated in enhanced immune response by low-dose cyclophosphamideBlood20051052862286815591121
- van der MostRGCurrieAJMahendranSTumor eradication after cyclophosphamide depends on concurrent depletion of regulatory T cells: a role for cycling TNFR2-expressing effector-suppressor T cells in limiting effective chemotherapyCancer Immunol Immunother2009581219122819052741
- ZhaoJCaoYLeiZYangZZhangBHuangBSelective depletion of CD4+CD25+Foxp3+ regulatory T cells by low-dose cyclophosphamide is explained by reduced intracellular ATP levelsCancer Res2010704850485820501849
- BeyerMKochanekMDarabiKReduced frequencies and suppressive function of CD4+CD25hi regulatory T cells in patients with chronic lymphocytic leukemia after therapy with fludarabineBlood20051062018202515914560
- AliKSoondDRPiñeiroRInactivation of PI(3)K p110δ breaks regulatory T-cell-mediated immune tolerance to cancerNature201451040741124919154
- BachanovaVCooleySDeforTEClearance of acute myeloid leukemia by haploidentical natural killer cells is improved using IL-2 diphtheria toxin fusion proteinBlood20141233855386324719405
- HuijtsCMSantegoetsSJvan den EertweghAJPhase I-II study of everolimus and low-dose oral cyclophosphamide in patients with metastatic renal cell cancerBMC Cancer20111150522129044