
Abstract
Background
The inhaled corticoteroid (ICS) ciclesonide (Cic), controls asthma symptoms in the majority of patients at the recommended dose of 160 µg/day. However, the relationship between the level of asthma control and increasing doses of Cic is unknown. This study investigated whether long-term treatment with higher doses of Cic would further improve asthma symptoms in patients with uncontrolled asthma despite ICS use.
Patients and methods
In a double-blind, randomized, parallel-group study, 367 patients were allocated to one of three treatment arms (Cic 160, 320 and 640 µg/day). After a single-blind, 3-week baseline period with Cic 160 µg/day, eligible patients were randomized to receive 52 weeks of treatment with Cic 160, 320 or 640 µg/day (double-blind period) during which forced expiratory volume in 1 second (FEV1), exacerbations and Asthma Control Questionnaire (ACQ) scores were measured.
Results
Treatment with all the three doses was associated with significant improvements in ACQ scores, FEV1 and asthma symptoms (P<0.01). There were no statistically significant differences between the three doses. The results of the primary end point analysis showed a numerical improvement in the ACQ score with Cic 640 µg/day compared with Cic 160 µg/day (least square [LS] mean: −0.122; two-sided P-value: 0.30). Post hoc subgroup analyses showed that the improvement in the ACQ score with Cic 640 µg/day compared with Cic 160 µg/day was statistically significant in subjects who experience at least one exacerbation per year (LS mean: −0.586; 95% confidence interval: −1.110, −0.062, P=0.0285). Adverse events were low and consistent with the known safety profile of Cic.
Conclusion
In patients with persistent, uncontrolled asthma, increasing the Cic dose from 160 to 640 µg/day provided no clear additional effect. Patients who experience more than one exacerbation per year may benefit from higher doses; however, further studies are necessary to confirm this. All Cic doses were well tolerated.
Keywords:
Introduction
The primary aim of asthma management is to achieve good overall asthma control, which consists of two domains.Citation1–Citation3 The first is current asthma control, which includes the day-to-day minimization of both daytime and nighttime symptoms, no activity limitation, minimal rescue bronchodilator use and no airway narrowing. The second domain includes minimizing the future risk of severe asthma exacerbations.
The Asthma Control Questionnaire (ACQ) is a validated composite score based on symptoms, activities, use of rescue medication and measurement of airway caliber over 1 week.Citation2 The score reflects the adequacy of asthma control and changes in asthma control that may occur spontaneously or as the result of treatment. Asthma is normally considered well controlled in patients with an ACQ score of <0.75. Patients with a score of ≥1.5 are considered to have poorly-controlled asthma.Citation3 The accepted minimal important difference in the ACQ score is 0.5.Citation4
Numerous studies have confirmed that treatment with inhaled corticosteroids (ICS) is associated with an increase in the level of asthma control. However, dose–response relationships between the level of asthma control and increasing doses of ICS have been less well studied. The Gaining Optimal Asthma ControL (GOAL) studyCitation5 compared the effect of increasing doses of fluticasone propionate (FP) and FP plus salmeterol on asthma control, as defined by the Global Initiative for Asthma (GINA) guidelines, in 3421 patients over 1 year. In patients pretreated with ≤500 µg beclomethasone dipropionate daily (or an equivalent ICS dose), the percentage that achieved well-controlled asthma increased by ~20% when the daily dose of fluticasone was increased from 200 to 500 µg/day, and by approximately another 10% following a further dose increase to 1000 µg/day. Post hoc analysis of asthma control in the Formoterol and Corticosteroids Establishing Therapy (FACET) study,Citation6 which included ~200 patients in each study arm, showed that the time with poorly-controlled (GINA-defined) asthma decreased from 21% to 15% of weeks when the dose of budesonide was increased from 200 to 800 µg/day.
The current recommended dose of ciclesonide (Cic) is 160 µg once daily.Citation7 This dose leads to asthma control in the majority of patients. In patients with severe asthma, a 12-week study found that a dose of 640 µg/day reduced the frequency of exacerbations without an improvement in lung function,Citation8 suggesting that the dose–response relationship may differ between different outcomes.
The current study (in patients with insufficient asthma control during treatment with Cic 160 µg/day) was designed to investigate whether long-term treatment with Cic 320 µg/day and Cic 640 µg/day for 1 year improves asthma control, measured by the ACQ score, lung function and exacerbations.
Patients and methods
Patients
Patients aged 12–70 years with a history of persistent asthma and on treatment for at least 6 months with an ICS at a stable dose (FP 200–1000 µg/day or equivalent) who were insufficiently controlled for a minimum of 12 weeks were enrolled. A list of prohibited medications is given in the Supplementary materials under the “Exclusion criteria” section. The ACQ criteria for inclusion in the baseline period are given in .
Table 1 ICS pretreatment dose and ACQ at the start of baseline
Study design
This was a multicenter, double-blind, randomized, parallel-group study, conducted at 39 centers in five countries: Argentina, Brazil, Germany, Israel and Russia. Patients were allocated to one of the three treatment arms (Cic 160, 320 and 640 µg/day) in a 1:1:1 randomization scheme, based on a blocked randomization scheme. Eligible patients were randomly assigned to treatment by means of a computerized Interactive Voice and Web Response System. During the treatment period and until the safety follow-up visit (30 days after the end of the study), patients, investigators, site personnel and any other parties involved in the study were blinded.
The study composed of a single-blind baseline period (3 weeks) during which all patients were treated once a week with Cic 160 µg/day to prevent the likelihood of a carryover effect from ICS pretreatment such as non-extra-fine particle budesonide or fluticasone. This was followed by a double-blind treatment period (52 weeks) during which all patients were treated twice daily with total daily doses of Cic 160, 320 or 640 µg/day. The visits took place at 6-week intervals, except for the first visit, which took place 4 weeks after patients were randomized into the study.
The study was approved by the Independent Ethics Committee for Clinical Pharmacology Trials, the Research Committee on Ethics and Pharmacology, the INAER Research Committee on Ethics (Argentina), the National Health Surveillance Agency and National Commission of Ethics in Research, the Ethics Committee on Research in Hosts of the Hospital Group Conception, the Research Ethics Committee of the Pontifical Catholic University of Rio Grande do Sul, the Research Ethics Committee of the Vila Heliopolis Hospital Complex, the Ethics Committee on Research of the ABC Medical School, the Research Ethics Committee of the Institute of Infectology Emilio Ribas, the Ethics Committee on Research in Human Beings of the Hospital Padre Bento de Guarulhos/SP, the Research Ethics Committee of the Center for Medical and PUC, the Federal University of Santa Catarina Ethics Committee on Research in Human Beings, the Ethics Committee on Research in Human Beings Pro-Cardiac-RJ (Brazil), the Ethics Committee of the State Chamber of Brandenburg, the Ethics Committee of the Bavarian State Chamber of Physicians, the Ethics Committee of the State of Berlin, the Ethics Committee of the Medical Chamber North Rhine, the Ethics Committee of Landesärztekammer Baden-Württemberg, the Federal Institute for Drugs and Medical products (Germany), the Institutional Helsinki Committee (Israel) and the Ethics Committees of the GBUZ NOS, the St. Petersburg State Medical University, the Siberian State Medical University, the City Clinical Hospital #2, the City Clinical Hospital n.a., the City Hospital #5, the Moscow Research Pulmonology Institute, the Novosibirsk State Medical Academy of Roszdrav Krasniy Prospect and the Medical Ethics Expert Committee at RMAPO (Russia) and was performed according to the Declaration of Helsinki and Good Clinical Practice Guidelines. All patients provided written informed consent. The clinical trial registration number is NCT01455194.
Study end points
The primary efficacy end point was the change from the end of the baseline period to the last value in the ACQ score. Throughout the study, patients completed the ACQ at weekly intervals either at investigational sites or at home. Secondary efficacy end points included time course of ACQ, analysis of asthma control (time to well-controlled asthma and well-controlled asthma over the course and at the end of the study; time to first ACQ improvement and ACQ improvement at the end of the study; frequency of patients below ACQ cutoff points [0.5, 0.75, 1.0, 1.25 and 1.5] and exploratory subgroup analysis to assess the impact of key demographic variables on the primary end point), asthma exacerbations and identification of patient subsets with markedly high benefits (ie, patient subsets that benefited from dose escalation).
Spirometry was performed using portable devices (SpiroPro), and it was mandatory that the same device was used for all measurements during the study (ie, at the site and at home). Forced expiratory volume in 1 second (FEV1) was recorded at weekly intervals at the site or at the patient’s home. All lung function measurements were performed prior to inhalation of the study medication. Rescue medication was withheld for at least 4 hours prior to each FEV1 measurement. All recordings were conducted between 06:00 and 10:00 in the morning and ±90 min of the first randomization visit time for each individual patient.
Patients recorded their asthma symptoms, compliance with study treatment and rescue medications in a diary. Asthma exacerbations were defined as a worsening of asthma requiring treatment with oral or other systemic glucocorticosteroids for at least 3 days, or a visit to the emergency room or hospitalization due to asthma. Inspection of the patient’s mouth and throat was performed if the patient reported an oropharyngeal adverse event (AE).
Safety
Safety monitoring included AEs, laboratory tests, urinalysis and vital signs.
Statistical analysis
For the primary efficacy end point, an analysis of covariance of the change in ACQ from baseline to last visit (including baseline ACQ and age as covariates, treatment, sex and ICS pretreatment dose as factors) was used.
For confirmatory statistical testing, two statistical tests were carried out in a hierarchical manner to address multiplicity. All other efficacy variables were evaluated using descriptive statistics. In addition, analyses of covariances or comparable nonparametric strategies were applied for continuous variables. A log-rank test and proportional hazards for the analysis of time-to-event variables and a Fisher’s exact test were used for dichotomous variables (“Statistical methods” section in the Supplementary materials).
Results
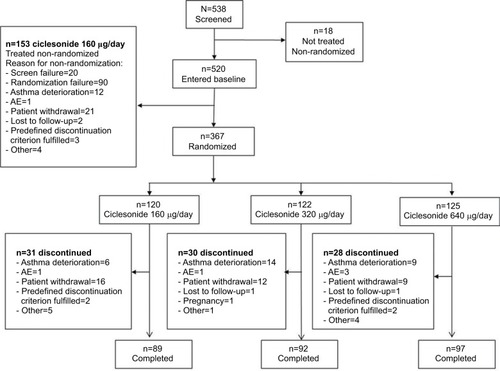
Of the 538 screened patients, 520 entered the baseline period and 367 were randomized. A total of 89 (24.3%) patients prematurely discontinued and 278 (75.7%) patients completed the study ().
Figure 1 Summary of all patients who were enrolled, randomized, completed and discontinued during the study.
Demographics
Demographic and baseline characteristics are summarized in and S1.
Table 2 Baseline demographics in the ITT population
Overall, patient demographics were similar between the three treatment groups. The mean age of patients was ~44 years, and ~63% were female. The majority of the patients were white (93.2%) and had never smoked (87.2%). The proportion of former smokers differed between treatment groups, with 8.3, 15.6 and 12.0% in the 160, 320 and 640 µg/day groups, respectively. The mean ACQ score at baseline was 2.2, reflecting poorly-controlled asthma. Mean baseline FEV1 reversibility (percentage of pre-bronchodilator FEV1) was 25.0%. The majority of patients had low-to-medium pre-study ICS doses (32.4% were on 201–250 µg/day and 59.1% were on 251–500 µg/day beclomethasone-equivalent ICS dose).
Concomitant medication
In general, the types of relevant asthma medications and the proportion of patients taking each relevant asthma medication were similar across the treatment groups. ICS was the most commonly used pre-study medication in all treatment groups. In line with the study inclusion criteria, where only inhaled salbutamol was allowed, the most commonly used medication during the baseline and randomized, double-blind treatment periods in all the treatment groups was short-acting beta 2-agonists (“Concomitant medication” section in the Supplementary materials and Table S2).
Primary end point ACQ
Mean ACQ scores improved significantly over the 52-week study period with all Cic doses (P<0.0001 in all treatment groups; ). However, there were no significant between-group differences in the change in ACQ scores with Cic 640 µg/day vs Cic 160 µg/day (least square [LS] mean: −0.122; 95% confidence interval [CI]: −0.353, 0.109; two-sided P-value=0.30).
Table 3 Change from baseline to last visit in ACQ score of within-treatment and between-treatment differences with three Cic doses
Subgroup analyses
Subgroup analyses to assess the impact of key baseline demographic variables (ACQ score, pre-study ICS dose, body mass index, smoking status, completers/withdrawals and FEV1) on the primary end point are given in the “Subgroup analyses” section of Supplementary materials and Table S3, and support the results of the intention-to-treat analysis.
Post hoc analyses were undertaken to examine the relationship between exacerbation history (categorized as: 0, ≥1 and unknown for the year prior to the study period) and change in the ACQ score. In the subgroups of no history of exacerbations and unknown history of exacerbations, changes in ACQ scores were similar across treatment groups. However, for subjects with a history of at least one exacerbation in the year prior to the study period, there was a significant difference between the mean change in ACQ scores in the Cic 640 µg/day treatment group and the Cic 160 µg/day treatment group (LS mean: −0.586; 95% CI: −1.110, −0.062, P=0.0285; ).
Table 4 LS mean change from baseline to last visit in ACQ score of between-treatment differences with Cic 640, 320 and 160 μg/day by exacerbation history subgroups (ITT)
Analysis of well-controlled asthma parameters
The time to well-controlled asthma was similar in all treatment groups ().
Figure 2 Kaplan–Meier plot of time from randomization to well-controlled asthma in the ITT population.
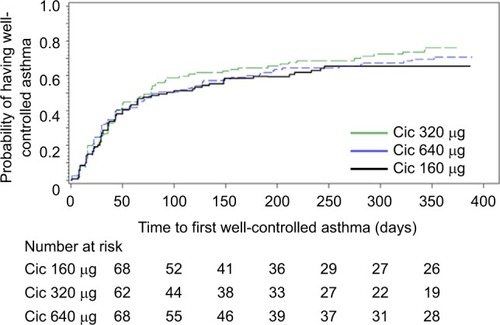
The number of patients with well-controlled asthma at the end of the study was similar across the three patient groups: 31.7, 36.9 and 40.8% of patients in the Cic 160, 320 and 640 µg/day treatment groups, respectively. The difference in the proportion of responders was not statistically significant by Fisher’s exact test (P=0.15 for comparison of the 160 and 640 µg/day groups, and P=0.60 for comparison of the 160 and 320 µg/day groups).
The difference in the number of weeks with well- controlled asthma over the 52-week study period was similar in all treatment groups ().
Table 5 Analysis of well-controlled asthma parameters over 52 weeks of treatment
FEV1
Overall, FEV1 results were similar across the double-blind treatment groups from baseline to last visit, and there were no significant differences ().
Table 6 Post hoc sensitivity analyses for change from baseline to last visit in FEV1 of between-treatment differences in the ITT population
Asthma exacerbations
The hazard ratio for the time to first asthma exacerbation was numerically in favor of Cic 640 and 320 µg/day vs Cic 160 µg/day, but the difference was not statistically significant. A total of 26 patients experienced exacerbations during this study: n=5, 11 and 10 in the Cic 160, 320 and 640 µg/day treatment groups, respectively. The majority of patients were treated with oral glucocorticosteroids, and two patients were hospitalized.
Safety findings
In total, 57.9% of patients treated with Cic experienced at least one AE, with no notable differences in AE frequency between treatment groups (Table S4). AEs occurring in at least 5% of patients in any treatment group are listed in the Supplementary materials.
Discussion
This study is, to our knowledge, the first to assess strict dose–response effects of the ICS Cic on asthma control, which is a patient-relevant outcome. The results showed that 160, 320 and 640 µg Cic were all associated with statistically significant improvements in ACQ. The differences between the three doses were marginal and not statistically significant. There were no statistically significant differences across the three Cic groups for any of the primary or secondary efficacy end points measured. However, post hoc subgroup analyses showed that in patients who experience more than one exacerbation per year, there was a statistically significant improvement in the ACQ score between the Cic 640 µg/day treatment group and the Cic 160 µg/day treatment group, suggesting that increasing the dose of ICS may improve asthma control in patients with frequent exacerbations.
Our findings mirror previous studies that investigated dose–response relationships of Cic.Citation8,Citation9 Bateman et alCitation8 treated 680 patients with Cic 160 or 640 µg/day over a 12-week period. The results demonstrated that statistically significant effects between the treatment groups were observed for some of the efficacy end points such as time to first exacerbation, morning peak expiratory flow and asthma symptom score. However, as in the current study, no statistically significant differences in FEV1 increases were seen between the groups treated with the two doses, while asthma control was not studied.Citation8 The 367 patients included in the current study had few exacerbations and it was not possible to observe differences between Cic doses on exacerbation frequency.
Previous research using ICS such as FP, budesonide and similar drugs at different doses has indicated that dose–response relationships are rather flat and may be affected by multiple factors including study design and the outcome parameter measured.Citation7,Citation10 Since an asthma control score is a composite of several individual outcomes, we anticipated that it might be possible to show dose–response relationships with this outcome, a hypothesis that had never been thoroughly studied. Interestingly, Cic was found to be effective on asthma control at the lowest dose tested (160 µg/day), but no dose–response was seen. Treating asthma patients, even those with insufficient control with the recommended 160 µg/day of Cic instead of prescribing a higher dose would reduce treatment costs. This approach to asthma treatment is in agreement with current GINA guidelines, which favor the use of the lowest dose possible to maintain asthma control. Once asthma control has been achieved and maintained, GINA recommends avoiding overtreatment by following their stepwise approach and reducing the ICS dose.Citation1 The current findings support this.
As previously mentioned, post hoc analysis of asthma control in the FACET studyCitation6 revealed that the time with GINA-defined poorly-controlled asthma decreased from 21 to 15% of weeks when the dose of budesonide was increased fourfold from 200 to 800 µg/day. However, the FACET studyCitation11 did not analyze whether patients with a history of frequent exacerbations would benefit more from the higher dose, and the number of exacerbations experienced by subjects in the year prior to study entry was not reported. Our data suggest that a further improvement in asthma control may be obtained with higher doses of Cic in case patients who have a history of more than one exacerbation per year, and this may be the subject for further study.
Responsiveness to ICS is generally much lower in smokers than nonsmokers with asthma.Citation12 Data published by Tomlinson et alCitation13 demonstrate that, compared with nonsmokers, smokers with mild persistent asthma are insensitive to the therapeutic effect of low-dose ICS. The disparity of the response between smokers and nonsmokers appeared to diminish with high doses of ICS. Only 12.8% of the total patient population (N=367) in the current study were current or ex-smokers, which made it difficult to detect any change in effect with increasing doses.
There are some limitations to the current study. One of the entry criteria was that the patients in spite of a medium-to-high dose ICS should have a poor ACQ score. It cannot be excluded that the lack of control shown by these patients may have reflected poor adherence rather than lack of efficacy of the ICS; therefore, increasing the ICS dose would be unlikely to improve their symptoms if the adherence was not improved by receiving a new treatment. However, the ACQ score increased and the asthma control decreased over the 3-week run-in period when all patients received Cic 160 µg/day. This finding does not support that poor adherence prior to the study was a reason for our findings.
The safety findings are in agreement with the findings of previous studies with Cic. Cic was well tolerated, and the side effects did not change with increasing dose. Cortisol levels, or other measures of hypothalamic–pituitary–adrenal (HPA) axis suppression, were not measured in this study; however, previous studies have shown that Cic doses do not significantly influence the HPA axis.Citation14–Citation16 Regarding pharyngitis, which is a known side effect of inhaled steroids,Citation17 there was no difference in its frequency or severity between the three treatment arms.
Conclusion
This study confirms that once-daily Cic is overall an effective and well tolerated treatment for persistent moderate-to-severe asthma. The recommended dose of Cic 160 µg/day improves asthma control, and no clear additional benefits are observed with higher doses of up to 640 µg/day. Patients who experience more than one exacerbation per year may benefit from higher doses; further studies are necessary to confirm this.
Author contributions
Dirkje S Postma and Søren E Pedersen contributed to the study design and protocol. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
We thank Renate Engelstaetter for the full support of setting up the study designs and protocol. We also thank her for her substantial contribution to the development of the protocol of this study and all the investigators who recruited and treated patients at the 37 centers involved in the CONTRAST study. Editorial support was provided by Caroline Loder and Rebecca Birch of Synergy Vision London and funded by Takeda Pharmaceuticals International AG and AstraZeneca.
Supplementary materials
Statistical methods
All the data were summarized using descriptive statistics. Statistical tests were two sided and conducted at the 5% significance level unless otherwise specified. Intention-to-treat (ITT) and per-protocol analyses were performed for the primary end point based on the full and valid case analysis sets, respectively. All other efficacy analyses were performed using an ITT analysis only.
The primary end point change from baseline to last visit in Asthma Control Questionnaire (ACQ) was analyzed using an analysis of covariance (ANCOVA) model including baseline ACQ and age as covariates, and treatment center, sex and pre-study inhaled corticosteroid (ICS) dose as factors.
To adjust for critical factors, a nonparametric ANCOVA was performed using the same factors and covariates as the ANCOVA model for the primary end point. Similar descriptive and graphical analyses were performed for the ACQ cutoff points 0.5, 0.75, 1.0, 1.25 and 1.5.
The number of weeks with well-controlled asthma was defined as the number of weeks that the patient had an ACQ score of 0.75 or lower over the course of the study. Treatment comparisons were carried out using an exact Wilcoxon–Mann–Whitney test for the percentage of weeks with well-controlled asthma.
The prevalence of patients with well-controlled asthma at the end of the study and the prevalence of patients with an ACQ improvement by at least 0.5 at the end of the study were analyzed using Fisher’s exact test.
To account for differences in the time to the first of these events, a log-rank test was used for the analysis of the time to the first measurement of well-controlled asthma and the time to the first ACQ improvement.
A Cox proportional hazards regression was computed using the same factors and covariates as the ANCOVA model for the primary end point.
Asthma exacerbation rates were analyzed using a Poisson regression model with the same factors and covariates as the ANCOVA model for the primary variable.
Confirmatory statistical testing was performed using a hierarchical approach to address multiplicity. All statistical analyses were performed using SAS Version 9.1.3 or later (SAS Institute Inc., Cary, NA, USA).
It was calculated that a sample size of 120 in each group would provide almost 90% power to detect a difference in mean values of 0.5, assuming that the common standard deviation is 1.2 using a two-group t-test with a 0.05 two-sided significance level.
Demographics
Additional demographic and baseline characteristics are summarized Table S1.
Concomitant medication
Exclusion criteria
Patients treated with an ICS at a stable dose between 200 and 1000 µg fluticasone propionate/day or equivalent for a minimum of 12 weeks could enter the study. The use of systemic glucocorticosteroids was not allowed for the entire duration of the study. If the administration of systemic glucocorticosteroids became necessary, the patient was withdrawn. Patients treated with one of the following nonsteroidal controllers (used either concurrently or in fixed combination with the ICS) in the 2 weeks prior to the first visit during the baseline period were not allowed to enter the study:
Chromones (eg, inhaled disodium cromoglycate and inhaled nedocromil)
Xanthines (eg, sustained-release theophylline and aminophylline)
Leukotriene antagonists (eg, montelukast and zafirlukast)
Lipoxygenase inhibitors (eg, zileuton)
Inhaled long-acting beta-agonists (LABAs; eg, formoterol and salmeterol)
Oral beta 2-agonists (eg, oral preparations of bambuterol, terbutaline, albuterol and salbutamol).
Subgroup analyses
Subgroup analyses to assess the impact of key demographic variables on the primary end point were performed (Table S3); data are presented for subgroups by ACQ score at baseline, pre-study ICS dose, body mass index, smoking status, completers/withdrawals and baseline forced expiratory volume in 1 second (FEV1).
Adverse events
Adverse events occurring in at least 5% of patients in any treatment group are shown in Table S4.
Table S1 Additional baseline demographics in the ITT population
Table S2 Concomitant use of short-acting beta 2-agonists in the ITT population
Table S3 Subgroup analyses of change from baseline to last visit in ACQ score of between-treatment differences with Cic 640 μg/day and Cic 160 μg/day (ITT)
Table S4 AEs occurring in at least 5% of patients in any treatment group
Disclosure
Dr Søren E Pedersen reports personal fees from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline and Sandoz. Dirkje S Postma reports grants for research (for the University of Groningen) from AstraZeneca, Chiesi, Genentech, GSK and Roche. Fees for consultancies were given to the University of Groningen by AstraZeneca, Boehringer Ingelheim, Chiesi, GSK, Takeda and TEVA. Niyati Prasad, Udo-Michael Goehring and Henrik Andersson were employees of Takeda Pharmaceuticals International GmbH during the time the study was conducted. The authors report no other conflicts of interest in this work.
References
- Global Strategy for Asthma Management and Prevention, Global Initiative for Asthma (GINA) [homepage on the Internet]2015 Available from: http://www.ginasthma.org/Accessed January 19, 2017
- JuniperEFO’ByrnePMGuyattGHFerriePJKingDRDevelopment and validation of a questionnaire to measure asthma controlEur Respir J199914490290710573240
- JuniperEFBousquetJAbetzLBateman ED; CommitteeGOALIdentifying ‘well-controlled’ and ‘not well-controlled’ asthma using the Asthma Control QuestionnaireRespir Med2006100461662116226443
- JuniperEFSvenssonKMörkA-CStåhlEMeasurement properties and interpretation of three shortened versions of the asthma control questionnaireRespir Med200599555355815823451
- BatemanEDBousheyHABousquetJCan guideline-defined asthma control be achieved? The Gaining Optimal Asthma ControL studyAm J Respir Crit Care Med2004170883684415256389
- O’ByrnePMNayaIPKallenAPostmaDSBarnesPJIncreasing doses of inhaled corticosteroids compared to adding long-acting inhaled beta2-agonists in achieving asthma controlChest200813461192119918689590
- AdamsNPJonesPWThe dose-response characteristics of inhaled corticosteroids when used to treat asthma: an overview of Cochrane systematic reviewsRespir Med200610081297130616806876
- BatemanEDCheungDLapa e SilvaJGohringUMSchaferMEngelstatterRRandomized comparison of ciclesonide 160 and 640 microg/day in severe asthmaPulm Pharmacol Ther200821348949818178494
- O’ConnorBJKilfeatherSCheungDEfficacy and safety of ciclesonide in patients with severe asthma: a 12-week, double-blind, randomized, parallel-group study with long-term (1-year) follow-upExpert Opin Pharmacother201011172791280320958119
- O’ByrnePMPedersenSMeasuring efficacy and safety of different inhaled corticosteroid preparationsJ Allergy Clin Immunol19981026 pt 18798869847425
- PauwelsRALofdahlCGPostmaDSEffect of inhaled formoterol and budesonide on exacerbations of asthma. Formoterol and Corticosteroids Establishing Therapy (FACET) International Study GroupN Engl J Med199733720140514119358137
- BatemanEDEfficacy and safety of high-dose ciclesonide for the treatment of severe asthmaExpert Rev Respir Med20137433934823964625
- TomlinsonJEMcMahonADChaudhuriRThompsonJMWoodSFThomsonNCEfficacy of low and high dose inhaled corticosteroid in smokers versus non-smokers with mild asthmaThorax200560428228715790982
- LeeDKFardonTCBatesCEHaggartKMcFarlaneLCLipworthBJAirway and systemic effects of hydrofluoroalkane formulations of high-dose ciclesonide and fluticasone in moderate persistent asthmaChest2005127385186015764767
- MarczakJCiebiadaMGorskiPSwitching from systemic steroids to ciclesonide restores the hypothalamic pituitary-adrenal axisPostepy Dermatol Alergol2014312596425097469
- SzeflerSRohatagiSWilliamsJLloydMKunduSBanerjiDCiclesonide, a novel inhaled steroid, does not affect hypothalamic-pituitary-adrenal axis function in patients with moderate-to-severe persistent asthmaChest200512831104111416162694
- NaveRMuellerHFrom inhaler to lung: clinical implications of the formulations of ciclesonide and other inhaled corticosteroidsInt J Gen Med201369910723516175