
Abstract
Nonsteroidal anti-inflammatory drugs (NSAIDs) are the leading cause of hypersensitivity drug reactions. The different chemical structures, cyclooxygenase 1 (COX-1) and/or COX-2 inhibitors, are taken at all ages and some can be easily obtained over the counter. Vasoactive inflammatory mediators like histamine and leukotriene metabolites can produce local/systemic effects. Responders can be selective (SR), IgE or T-cell mediated, or cross-intolerant (CI). Inhibition of the COX pathway is the common mechanism in CI, with the skin being the most frequent organ involved, followed by the lung and/or the nose. An important number of cases have skin and respiratory involvement, with systemic manifestations ranging from mild to severe anaphylaxis. Among SR, this is the most frequent entity, often being severe. Recent years have seen an increase in reactions involving the skin, with many cases having urticaria and/or angioedema in the absence of chronic urticaria. Aspirin, the classical drug involved, has now been replaced by other NSAIDs, with ibuprofen being the universal culprit. For CI, no in vivo/in vitro diagnostic methods exist and controlled administration is the only option unless the cases evaluated report repetitive and consistent episodes with different NSAIDs. In SR, skin testing (patch and intradermal) with 24–48 reading can be useful, mainly for delayed T-cell responses. Acetyl salicylic acid (ASA) is the test drug to establish the diagnosis and confirm/exclude CI by controlled administration. Desensitization to ASA has been extensively used in respiratory cases though it can also be applied in those cases where it is required.
Introduction
Nonsteroidal anti-inflammatory drugs (NSAIDs) are recognized to be the most common drugs involved in hypersensitivity drug reactions (HDR).Citation1–Citation5 Until recently, antibiotics, particularly betalactams (BLs), were considered the most important inducers,Citation6–Citation10 but after confirmation NSAIDs are now at the front.Citation1,Citation4
Interest in updating information about HDR to NSAIDs (HDR-NSAID), a large family of drugsCitation11,Citation12 derives from the research done by the RIRAAF (Spanish acronym for the network for the study of adverse drug reactions [ADR]),Citation13 reflected in several publications.Citation14–Citation20 Although for many years HDR-NSAID were considered to affect adults, they also occur in children and adolescents.Citation21,Citation22
Although a connection exists between atopy and HDR-NSAID, this differs from IgE allergic reactions to drugs, like HDR to BLs,Citation23 more related with the cross-intolerant (CI) category.Citation2,Citation3,Citation16,Citation24–Citation28 Since 2010 several groups have worked focusing on the skin, the most frequent organ involved.Citation1–Citation5 The European Academy of Allergy and Clinical Immunology (EAACI) provided a new classification that has been progressively adopted by many groups worldwide,Citation29–Citation35 although not by others, probably due to local/national differences in patterns of drug prescription, medical indications and self-intake of these drugs, as well as in some instances the limited number of cases evaluated in clinical practice in some centers.Citation36,Citation37 When subjects complaining of HDR-NSAID develop a reaction they do not consider NSAIDs as the cause because the reaction occurs in the context of different coincidental triggers and the physicians are often not familiar with the procedures to follow. It may take a long time to evaluate these cases, even though several episodes occurred in a patient, sometimes eight or more.Citation2,Citation3
It is surprising that some NSAIDs can be obtained over the counter, and are advertised on TV or in other media. In a study published in the lay press, the two most important chemicals found in depurated water were dioxin and ibuprofen metabolites. The price we are paying for this, as it contributes to the increased exposure, is a rise in the reactions to aryl propionic acids, particularly ibuprofen. This situation resembles that occurring with BL antibiotics, where subjects not only become sensitized or resensitized, but also develop clinical manifestations after hidden exposure.Citation38
Leaders in the field, although attempting to conciliate the European and American positions, still have disagreements.Citation36,Citation39,Citation40 This may be related with the expertise of each author in their daily practice rather than differences among countries/populations because common drugs involved are ibuprofen and paracetamol, followed by diclofenac and more recently selective COX-2 inhibitors.Citation4,Citation5,Citation41 In a collaborative study with a Chinese group, a high degree of homology existed with the Spanish population not only in the drugs involved but also in clinical entities.Citation42 Recent years have seen an increasing number of manuscripts concerning children.Citation43–Citation48 The adolescent population might be less exposed to NSAIDs as compared to children,Citation49,Citation50 although sports people usually require NSAIDs for treating muscle and bone lesions.Citation51–Citation53
Classification of HDR-NSAID and mechanisms
ENDA classificationCitation54,Citation55 has been a reference guide for clinicians and investigators working in this field. This classification is not new but rather represents an extension of previous ones but better adapted to daily demandsCitation2,Citation12,Citation14,Citation36,Citation49 and provides a more precise approach for the diagnosis and management of subjects with HDR-NSAID. However, further improvement of the classification is expected to occur in the coming years, with resulting modifications in the classification.
To the five major groups shown in with the corresponding acronyms and two additional entities added: organ-specific reactions and skin/systemic reactions included in the SR category. Most of the proposed mechanisms have been inferred from the clinical manifestations accompanied by basic knowledge obtained mainly from the cases with NERD, although the subject is in fact more complex.Citation56 A list of NSAIDs is provided in and includes a large number of chemically different organic compounds classified according to the chemical structure.
Figure 1 (Continued)

Figure 1 Groups and chemical structures of the different NSAIDs.
Abbreviation: NSAID, nonsteroidal anti-inflammatory drug.
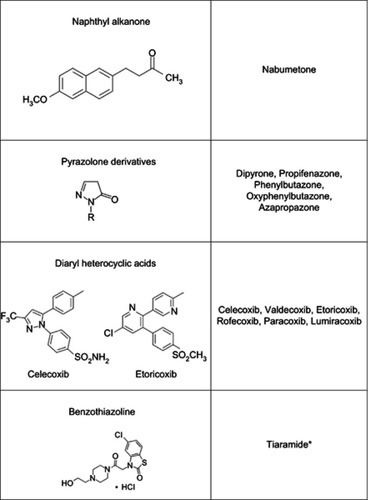
Table 1 Classification of NSAIDs-HDR and mechanisms and example of drugs involved
Considering the entities within the CI category (), the first proposed mechanism was inhibition of PGE2 synthesis and activation of key cells like mast cells, basophils, and eosinophils.Citation57 This created a shunting with released metabolites of the LOX pathway, PGDCitation2, and histamine, as well as several cytokines and other protein mediators, including tryptase.Citation58–Citation60 However, a more complex mechanism emerges if we look at all the by-products released, the enzymes involved, and the receptors through which the mediators signal.Citation61
The most distinctive finding in NERD is not shared by the other entities. It consists of chronic inflammation, mostly with the presence of eosinophils, extending beyond the acute episode. Both COX and LOX mediators contribute to the lesions including an up/downregulation of some by-products,Citation62,Citation63 although a product of the COX pathway, PGD2, is also released by mast cells.Citation58 Other abnormalities extend beyond the classical COX and LOX pathways, including the involvement of lipoxin A4. In this context, an interplay between all these cells plus those of the bronchial and nasal epithelia originate a response that goes beyond the classical TH1/TH2 paradigm.Citation64
Classification in
NERD.Citation55 Although we cannot state exactly since when, this is no longer the most frequent entity among HDR-NSAID. As ASA is not the most common drug involved, the term NERD seems more appropriate. Besides the classical entity reported,Citation65 there are entities with less severe manifestations that do not follow the natural course.Citation27,Citation34,Citation35,Citation66–Citation69 Within ASA-induced asthma several endotypes have been reported that may correspond to different mechanisms or variations of the same mechanism involved in NERD.Citation62 To complicate this, we have reported in a small series of cases selective respiratory responders that do not fall into this classification.Citation70
NECD.Citation55 In subjects with active CSU symptoms aggravate after intake of strong COX-1 inhibitors. This may affect up to 30% of CSU cases, although these have not been widely confirmedCitation1–Citation3,Citation12,Citation33 and other types of urticaria/angioedema like physical urticaria may also be aggravated.Citation71,Citation72 Whether NECD represents a subtype or it may occur in any case of CSU has not been clarified so far.
The evidence supporting the mechanism in NECD is based on limited data.Citation12,Citation15 The basal abnormal state is not present in CSU and the entity itself may change, with a subsequent variation in the response to NSAIDs.Citation73 Less is known about the response in NIUA where the evidence is missing and studies are needed to unveil differences with NERD and NECD.Citation74
NIUA.Citation55 This entity has been neglected or given less attention till recently, when our group provided evidence supporting that it was the most prevalent of all entities, confirmed by other groups.Citation1–Citation5,Citation69,Citation73–Citation76 Published literature and classical textbooks still do not accept it but it is expected that in the coming years this entity should be taken into account.Citation12,Citation77–Citation79 Although anaphylaxis was not included in the first ENDA classification, later reviews have now considered it.Citation80 Claims by some European groups regarding ENDA classification consider it incomplete and have made us to clarify this,Citation56 as shown in . Now in NIUAA, we include the combined forms of respiratory plus skin involvement accompanied in certain cases with systemic symptoms.Citation56
The mechanism proposed for the entities within this group has been directly inferred from that for NERD and assumed to be the same.Citation12,Citation56,Citation81 Although all strong COX-1 inhibitors can induce reactions, clinical observations suggest that there might be differences in the way they interact with the COX enzymes.Citation82 For example, ASA induces an irreversible inactivation of COX-1 and COX-2 but differences with other NSAIDs may explain why some subjects having a response to ASA tolerate ibuprofen, diclofenac, or piroxicam even at high dose.Citation3,Citation12,Citation52,Citation82 Transient competitive inhibition of prostanoid biosynthesis may also contribute to symptoms,Citation83 and specific drugs like piroxicam, although considered a strong COX-1 inhibitor, are better tolerated in cases with skin involvement,Citation80 but our experience questions whether tolerance occurs in NERD. Paracetamol has been shown to suppress PGE2 biosynthesis contributing to the imbalance leading to excess production of LOX pathway products.Citation16,Citation84
The two groups of entities below are considered SR and are induced by specific immunologic mechanisms.
SNIUAA.Citation55 This can be indistinguishable from NIUAA and involves mainly the skin, though when respiratory and/or other organs are involved this is anaphylaxis. Several entities can be included ranging from mild urticaria/angioedema to the more severe forms. Isolated angioedema in the absence of other skin manifestations may occur, and this may be produced by another mechanism still unknown.Citation56 We include single respiratory responders to several drugs that are not chemically related and that have good tolerance to ASA.Citation31,Citation85
SNIDR.Citation55 It includes well-differentiated entities such as NIU, delayed angioedema, exanthematic and bullous reactions, including the most severe like SJS-TEN. T cells are implicated and reactions usually occur at intervals of 24–48 hours after drug intake although it can be longer. The term single may not be appropriate and the term selective would be better because two or more different non-chemically related NSAIDs may induce these reactions, and each one can induce a different clinical entity.Citation86–Citation88
Evidence supporting specific immunologic mechanisms in IgE (SNIUA) or T-cell-dependent reactions (SNIDR) exists.Citation89–Citation92 Positive skin testing with some pirazolones like metamizole or propifenazone,Citation93,Citation94 in vitro basophil activation with metamizole,Citation93,Citation95 or sIgE to ASACitation96 supports an IgE-mediated reaction but other mechanisms nonimmunologically mediated are worth exploring.Citation89 All efforts so far to detect sIgE Abs to diclofenac, arylpropionic, and other drugs like COX-2 inhibitors have been unsuccessful.Citation91,Citation97 Of particular concern are the propionic derivatives where the response is so selective that subjects tolerate ASA, the other strong COX-1 inhibitors as well as other NSAIDS, and also other aryl propionic drugs. For example, subjects developing immediate reactions to naproxen can tolerate ibuprofen.Citation29 Further evidence now being evaluated (data not published) show that some subjects become tolerant over time. With this evidence for the propionic derivatives it is hard to envisage an alternative mechanism to the IgE-specific response but further efforts for the elucidation are warranted.Citation56
Regarding SNIDR, T-cell involvement existsCitation56 with allergic and photoallergic reactions reported with positive delayed skin testing, both intradermal and patch testing, biopsies showing a mononuclear cell infiltrate. NSAIDs are difficult to study in vitro because they interfere with prostaglandin biosynthesis pathways at several steps.Citation56 The development of T-cell clones specific for certain NSAIDs has contributed to elucidate in part the physiopathology, together with genetic studies involving HLA molecules and antigen presentation.Citation56 To our knowledge, drug-specific T-cell clones to NSAIDs have not been produced and this limits understanding the mechanisms involved.Citation56 Regarding drug metabolites of ibuprofen and pyrazolones,Citation98 although some have been identified, studies regarding their antigenicity are still pending. In cases with HDR to pirazolones, T-cell proliferation has been shown.Citation99–Citation101 This suggests the specificity of T-cell responses to different metabolites and that low amounts of such metabolites might be generated during in vitro cell culture, allowing stimulation of specific T cells. A similar situation may occur with other NSAIDs, including weak and selective COX-2 inhibitors and further research would be needed.
The four subgroups of T-cell-dependent reactions within the IV group of Classical Gel and Coombs classification have been reported with NSAIDs.Citation56 Some examples for each one are shown below with the addition of a fith sub-group.
Type IVa. Contact and photo-CD. This is considered a Th1 response with effector T-cell involvement and production of interferon gamma (IFN-γ), IL-12, and other cytokines and chemokines.Citation92,Citation102,Citation103
Type IVb: MPE is the classical entity with activated T cells, CD4, and CD8, which home to the skin and form a perivascular infiltrate that can be accompanied by eosinophils and neutrophils. Activated T cells are present with the expression of several activation markers and production of IL-4 and IL-5.Citation104
Type IVc: SJS-TEN. This is a very severe entity, both in the histopathology and clinical manifestations, with the presence of activated T cells that release perforin and granzyme-B leading to apoptosis and a massive death of keratinocytes and other cells.Citation105 An entity with lesions partly resembling TEN is FDE, though this is usually limited to well-localized areas but sometimes, if more extensive, must be differentiated from SJS-TEN. MPE, which in severe lesions is often named toxicodermia, and CD can often be quite aggressive and involve an important degree of cell death. In fact, MPE can be followed by extensive desquamation in the absence of bullae formation.Citation106,Citation107
Type IVd: AGEP. T cells as well as neutrophils are attracted to the skin inducing a typical lesion consisting of small confluent pustules without infected fluid. Lesions are generalized, usually mild, and can produce problems in the clinical course.Citation108,Citation109
Type IVe. NIU. Although AX, AX-CLAV, and antibiotics are the most common culprits,Citation110–Citation112 NSAIDs are also involved.Citation71 Although, this entity has only been studied in detail recently showing T-cell activation with the presence in peripheral blood-activated T cells (CD4 and CD8) responsible for the lesions. Skin immunohistopathology is in consonance with the pattern observed in peripheral cells.Citation110
DRESS. This reaction starts with mild exanthema that may generalize to an intense erythema, often accompanied by angioedema, joint involvement, fever, malaise, and liver damage. Neutrophilia and eosinophilia can also be present.Citation113,Citation114
Other clinical entities in which the mechanisms have not been so extensively studied are included in .Citation115–Citation117
Focusing on the clinical entities included within the CI groups, a number of claims have been raised, especially with NIUAA, indicating that particularly in children and adolescents both cutaneous and respiratory manifestations may occur.Citation60,Citation118 These reactions also occur in adults although in a lower percentage.Citation3 Further queries can be raised concerning this classification that rather than invalidating it actually contributes to improving the classification, providing more detailed information on the clinical entities outlined above.Citation56
Prevalence
Although different approaches concerning adverse drug effects have been made,Citation119 few data have focused on HDR-NSAID. Published reports on ADR mostly relate to new drugsCitation120,Citation121 and include side effects that go beyond the field of HDR. Once drugs are released on to the market and have lost their novelty as a new drug product or category, interest is gradually lost.Citation119 Because ADR including NSAIDs occur in the context of complex situations with many offenders, links to side effects are often not convincingCitation122 and side effects to HDR-NSAID may be attributed to errors by the physician or other health care givers.Citation119 The term prevalence for HDR in general and even for those groups of drugs like antibiotics is difficult to establish.Citation56 Nevertheless, despite the limitations we shall use this term here referring to HDR to NSAIDs.
Propionic acid derivatives are available worldwide, particularly ibuprofen, although there exist country/regional differences.Citation4,Citation42 In one study, a consecutive series of >4,000 cases with DHR reactions were evaluated in a period of 6 years. The protocol applied for NSAIDs was as described by the EAACI drug expert committee.Citation55 The analysis of the different factors/variables of the study was made by Mann–Whitney tests and chi-square analysis. After confirmation by DPT (drug provocation test) the 47.2 were confirmed as hypersensitivity to multiple NSAIDs followed by antibiotics with an 18%, less than the half and in a minor proportion by other drugs like non-BL antibiotics, contrast media, and other drugs.Citation1
Ibuprofen and paracetamol are the most commonly prescribed drugs in children, with some competition with BLs.Citation49,Citation50 When HDR are considered in children some studies indicate that antibiotics are the most frequent before making the final evaluation, after which the opposite occurs.Citation5,Citation72 From adolescence up to the oldest people the rest of the NSAIDs shown in are progressively prescribed, although ASA has diminished its indication in cardiovascular prophylaxis worldwide.Citation123,Citation124 In a large multicentric study conducted under the GA2LEN program, >60,000 cases were evaluated in 22 centers from 15 countries, and the aim was to estimate the prevalence of NERD assessing upper and lower respiratory disorders. For this purpose, cases were selected in each country by random from general physician registries and a questionnaire was undertaken. Sampling probability weights were used to standardize prevalence by gender and 5-year groups. The association of NSAIDs as potential agents inducing respiratory symptoms was made by logistic regression analysis. Results showed a mean prevalence of 1.9% with a variation rank from 0.9 to 4.9 in the different centers included.Citation67
Table 2 Proposed guidelines for the differential diagnosis of clinical manifestation where skin symptoms are the predominant
In another study, a systematic review identified patients with NERD selected by either challenge or a self-reported history showing a prevalence of 9% (95% confidence interval 6%–12%) in the cases confirmed by oral provocation test and 9.9% (95% confidence interval 9.4%–10.5%) using a self-reported historyCitation68 concluding that the prevalence was similar by both approaches. This is similar to other estimations with sufficient data provided for respiratory diseases.Citation62 For the other entities within the CI group, and also for SR, fewer data are available and we refer the reader to a recent review giving details on this issue.Citation56
Impact
As NSAIDs contribute to the highest percentage above all drugs inducing HDR-NSAID and they are widely used as stated above, the impact in managing cases with these reactions is paramount. For dealing with this, we divide this section in three parts: clinical entities, further impact, and role of atopy.
Clinical entities
The classification in provides a guide to allocating the different entities shown above. Because these are described elsewhere,Citation12,Citation14,Citation49,Citation50,Citation54,Citation55,Citation62 we will focus on just a few points. Time interval is implicit in clinical manifestations,Citation14,Citation29 so to use this variable as discriminative for a new classification is not needed.Citation118 Within each group several entities can be identified although more will emerge or be segregated from these as more research is done.
NERD. The natural course is well established and in many cases it may have an unfavorable clinical evolution that needs special surveillance, close attention, and great efforts for the management. Unlike other entities, NERD patients usually have previous airway involvement and even if no strong symptoms are present, scanning or testing the upper airways and studying pulmonary function, including the lower airways, shows some degree of involvement. Nowadays many physicians recommend avoiding NSAID intake. In our community, although not specifically studied, we no longer see as many chronic severe forms as before. Reactions occur in a short time interval, usually <2 hours after drug intake, although this can be longer.Citation40 A detailed description of the symptoms reported by the patient or observed by the clinician, the time interval after drug intake, and the previous status of the patient must be recorded when taking a clinical history.Citation2,Citation27 The description by the patient is very often quite accurate and matches what we usually observe in the DPT, although fortunately less intense and severe because there is a dose–effect relationship.
Subjects can be exposed without knowing the risks taken and often experience mild symptoms that are not imputed to NSAIDs since it is coincidental with physical factors, other drugs or chemicals, foods, and even psychological triggers that can be confounding factors or cofactors.Citation125 Respiratory symptoms usually appear in the course of the underlying disease with involvement of the upper and lower airways with nasal polyposis in severe cases. Occurrence before the third and fourth decades of life is unusual and the more common natural order of symptom appearance is the upper airways, followed by the lower airways and later by symptoms elicited by NSAIDs. Triggering factors in the absence of NSAID intake include alcohol, and possibly we must consider other histamine-releasing factors that may aggravate or predispose.Citation126 Initially atopy was not present but nowadays it is a fact that may correspond to a general increase in atopy in western populations, although the connection is hard to define.Citation127 Nasal symptoms are quite bothersome and in addition obstruction, rhinorrhea, loss of smell, and anosmia may occur. In cases of polyp recurrence corticoids may be needed for control.Citation62
NECD. Aggravation of CSU after NSAID intake may occur in up to 30% of cases. In spite of the progress made in recent years concerning understanding the pathophysiology of CSU,Citation128 a better phenotyping has now been made. Nevertheless, we still do not know in which type of CSU NSAIDs reactivate or worsen the disease.Citation56 If this does not occur, the mechanism acts in the activation pathway at a level common to the different subphenotypes where the pathophysiology is common for all forms, including the autoimmune and not autoimmune, and possibly other forms of urticaria.Citation56,Citation128 The clinical manifestations consist of a worsening that can often be latent, very attenuated, or controlled by medication in the previous state. If this is the case, it requires a more aggressive treatment with the use of CS.Citation12 Despite this, there are cases in children and adults of development of symptoms involving several organs and thus we are dealing with anaphylaxis.Citation21 Although less known, some reports point out that physical urticaria and possibly othersCitation129 may be worsened by NSAID intake. Although evidence is mostly supported by single cases or small series, more information is needed in this respect but it is not surprising that any type of activation of mast cells, which occurs in all types of urticaria, may cause worsening in certain cases after the pharmacologic interaction after intake of these drugs.Citation56
NIUAA. This is the most common entity and it can be confusing when we depend on just the clinical description.Citation3 However, the patient history provides clues to differentiate it, like the appearance of urticaria with or without angioedema in a well-delineated pattern at any place or all over the body, being most troublesome on the face. The time interval is usually no longer than 2 hours, although episodes may appear up to 6 hours later or longer, and in many instances angioedema can be predominant or be the sole manifestation.Citation27 The natural evolution indicates that this is a well-defined entity that does not convert to NERD over a long period of follow-up, as suggested by some.Citation130
SNIUAA. Following the general classification, the two entities that follow belong to SR. Clinical manifestations also include urticaria accompanied or not by angioedema, isolated angioedema, or anaphylaxis, as occurs in NIUAA.Citation89 However, organ-specific reactions have recently been reported that, although the skin is not involved, we still include in this section because patients have good tolerance to ASA, as far as we know.Citation70 If more evidence is supported by different groups in the coming years, the same term can be used with the extra addition of an “A” for anaphylaxis (NIUAAA). The term acute does not fit well because all the cases of NSAID-DHR are acute with no chronic forms, excluding NECD. The time interval in these reactions is usually <1 hour, but not always, as occurs with the immediate IgE reactions to AX and other BL antibiotics.Citation32
SNIDR. The entities included in this group are shown in , and although NSAIDs are not the main drugs eliciting these reactions, particularly the severe ones, some entities like FDE or MPE can be induced. Much literature has been dedicated to thisCitation121–Citation133 and in this context we recommend several reviews for further reading.Citation54–Citation56,Citation78,Citation103,Citation105
Further phenotyping
It is becoming clearer that within the five major categories, more phenotypes and subphenotypes are now recognized that help understanding the pathologic mechanisms involved. This extends not only to NERDCitation62 but to the other entities.Citation56,Citation89 Further phenotyping is not only of interest in understanding new mechanisms but also of clinical relevance in order to establish a prognosis once a diagnosis is made and adequate alternatives are given.Citation14–Citation16,Citation56
NERD. Within the classical syndrome known as ASA triad there are several endotypes that have been clearly described by several groups. More subphenotypes have been proposed that need external validation by other groups and in other populations.Citation31,Citation134 In one study, significant differences were found in total urinary LTE4 and serum total IgE and also in the eosinophil count in the different subgroups.Citation135 As shown above, single respiratory responders to one or several NSAIDs with good tolerance to ASA exist and must not be considered in this group; further details will be given below.Citation70
NECD. Although not in all instances, subjects with CSU worsen with NSAIDs, though we do not know which cases develop symptoms after NSAID intake.Citation56
NIUAA. In the clinical description of this group, several entities have been included that clearly represent well-differentiated forms.Citation3 These have been described in detail in a previous section of this review and reported elsewhere.Citation14,Citation17,Citation54,Citation55 The combination of both NERD plus NECD has been reported but much more frequent than NERD are those with mixed reactions. We prefer this term to blended reactions, though it is still pending a defined nomenclature that is awaiting further discussion and consensus agreements.Citation14,Citation17 Clinical data in children and adolescents point in this direction.Citation22,Citation134 In this context, further consensus to set up the clinical criteria is being demanded.Citation56
SNIUAA. Within this category, the entities included can be well defined or be unique, with a variation in symptom expression from less to more severe. Thus, urticaria can be the first step in an anaphylaxis episode that after re-exposure within a short time can be more severe, while the opposite can occur; if a long time has elapsed after the first episode symptoms can be minor or even absent. This is well known with the BL model, particularly in those cases with IgE reactions to AX and some cephalosporins,Citation9 and it is extensible to everything, including SNIUAAA.Citation56,Citation89 It is clear that isolated angioedema can be a reproducible and consistent entity, without further progression in repeated episodes, but there are no clues as to the underlying mechanism in these cases.Citation56
NIDHR. This is the group of HDR-NSAID where the phenotypes are best defined and more consistent, induced by the different drug as well as the specific mechanism within an effector T-cell response. In fact in a new updated revision, we have included an additional Type IVe corresponding to NIU, also known as accelerated allergic reactions and also serum sickness-like disease.Citation110
Role of atopy
Atopy as a trait is a complex definition applied to subjects who develop sensitization to inhalant as well as food proteins and glycoproteins by a mechanism mediated by IgE Abs.Citation135 There is a big difference in the prevalence of respiratory compared to oral allergen sensitizations, although both are on the increase. To connect both the GI and the respiratory system is not easy because usually when we are positive to an inhalant, like the case of birch pollen, in most instances we develop symptoms after oral exposure also known as secondary sensitization. When primary sensitization occurs by the oral route although IgE Abs are found, very often subjects are tolerant, and this makes sense because the GI system has been adapted to develop immunologic tolerance to proteins that pass through it.Citation136,Citation137 Whether HDR-NSAID are linked with atopy or not is not sufficiently clear, although different references support thisCitation2,Citation3,Citation56 and further stratification in large numbers of cases and with molecular allergens is needed for a better clarification.Citation56 Some cumulative evidence of HDR-NSAID points to an increase in allergic reactions to NSAIDs but appropriate studies with long enough time follow-up periods to support this are lacking. Unreported data from our group show an increase but these are not complete as we did not know the denominator for referring and therefore these comparisons lack accuracy.
Management
In this section, we include the first step consisting in diagnosis followed by the management of the cases once the diagnosis has been established.
Following the general description shown in the text, after the clinical history has been taken a clear approach of how to proceed must be elucidated.Citation2,Citation3,Citation27 For this purpose, two major categories can be envisaged: CI or SR. If the clinical information is reliable and the number of episodes is provided, the classification can be consistent and definitive. Because NSAIDs are drugs taken very frequently and subjects often take them without medical prescription, they come to the allergist with the diagnosis already made and our intervention consists of making a clear report, including the diagnosis and what recommendations to propose.Citation3,Citation27
If clinical manifestations are limited to the respiratory airways, we are dealing in most instances with CI and NERD is the category we are dealing with and can be rhinitis and/or nasal polyposis and/or asthma,Citation62 although there are exceptions.Citation32 When in addition to respiratory symptoms patients also report cutaneous symptoms (mixed reactions) the approach is different and will be detailed below. The most frequent reactions are those with cutaneous involvement and, in the event a single episode has occurred, the subject can be CI or SR.Citation3,Citation56 In our populations as well as in others, the proportion of CI to SR is 3 to 1.Citation1,Citation3 However, great differences may exist not only from country to country but also when we consider different age strata. Children are much more common to be CI than SR,Citation138 although not all series agree with this.Citation21
NERD. Cases with the symptoms described above are easily diagnosed without need for further confirmation.Citation62 The problems arise when first episode appear and this is the first step in the course of the disease. Rhinoscopy provides information on the status of the mucosa with the presence of obstruction and edema, often signs of infection in the mucus and polyps. All these symptoms must be slight and no polyps present at the onset of the disease.Citation139 In computed tomography of the sinus, the extension of the lesion can be seen, as well as opacification.Citation140 The more recent procedure of magnetic resonance imaging may be needed when intraorbital and other complications are suspected.Citation62 In children, the classical NERD has been rarely reported although cases with upper or lower airway symptoms may occur.Citation39,Citation40,Citation69
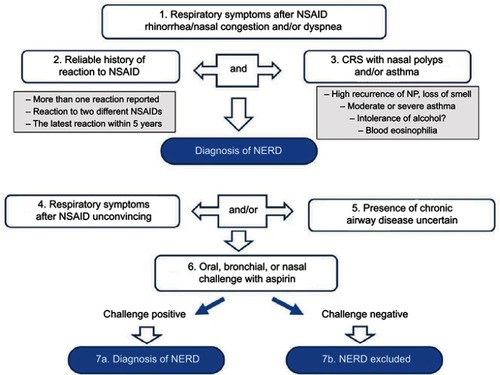
Today several diagnostic algorithms are provided that are useful for the diagnosis of NERD. As reported by the ENDA group,Citation62 the following are indicators of category and groups within which to classify according to : upper and/or lower immediate symptoms after NSAID intake whether or not reported by the patient but clearly described in a clinical report, involvement of two or more strong COX-1 inhibitors but also one strong inhibitor and a weak one like paracetamol, the occurrence of several episodes, the existence of previous symptoms, the existence of nasal polyposis and of persistent nasal complaints indicative of rhinosinusitis.Citation62 Several episodes with all these characteristics are quite indicative and when some are missing or the history is not reliable, further confirmation is needed. Although several algorithms have been provided through the years, the most updated has been published by the ENDA working group.Citation62 provides the steps to follow in the case of NERD evaluation.Citation62
Figure 2 Diagnostic algorithm for NERD.
Abbreviations: CRS, chronic rhinisinusitis; NERD, NSAID-exacerbated respiratory disease; NP, nasal polyposis; NSAID, nonsteroidal anti-inflammatory disease.
NECD. This is not difficult because CSU appears first and can sometimes be with minor symptoms. In these circumstances, avoidance of the drugs leads to improvement although sometimes additional support with corticoids is needed for a quick and better improvement.Citation55,Citation80
NIUAA. In this group, because there are alternatives, another NSAID can be the choice and there are quite a large number of drugs that are strong COX-1 inhibitors that can be safely administered.Citation89 Skin testing has only been validated for pirazolones, mostly with metamizole, although sensitivity does not surpass 50%.Citation93 In this sense, basophil activation can be an alternative, though also with limited sensitivity, but cases exist of skin-test negative and basophil positive and vice versa. Putting both techniques together, sensitivity does not increase >60%.Citation89 Recommendations for escalating and the doses with different NSAIDs have been published.Citation3
SNIDR. The problems diagnosing T-cell-mediated reactions come mainly when any NSAID induces a reaction in the context of the intake of several drugs, all of them being strong candidates.Citation56 When this occurs, according to the probability and risk/benefit balance, we must start with the drug that, having no alternatives, has the lowest probability of being responsible. The acute phase is quite useful for monitoring the reactions and seeking immunologic markers. The general approach, valid also for NSAIDs, is to monitor the reaction in both the acute phase and the resolution period, taking samples from peripheral blood and skin. Results show a perivascular mononuclear cell infiltrate in the skin with the presence of CD4+ and CD8+ T cells that are activated expressing IL-25+, early and late lymphocyte activation markers, the presence of IL-12 and IFN-γ and, depending on the severity of the lesions, perforin and FAS-L. These changes are also observed in parallel in peripheral blood together with the expression of markers on T cells that home to the skin like CLA. Further studies and transcriptomic analysis add additional information to the mechanisms involved in these lesions.Citation141–Citation143
General recommendations for intradermal and patch testing are shown in several reviews.Citation144,Citation145 In this respect, although no large series of T-cell-mediated reactions to NSAIDs are available there are several studies with different drugs from these groups that show the concentration used for intradermal or patch testing.Citation146–Citation148 In general, patch testing is reserved for those NSAIDs that are not soluble, and powder solutions in petrolatum at a concentration of 5%–20% w/w are recommended although a maximum concentration value in a negative control needs to be assessed with new drugs where information is not available in the literature. For investigating photoallergic reactions, the most effective and widely used method is to perform photo-patch testing prepared in petrolatum and applied in duplicate sets to the skin, irradiating one of them with a UV source, as described.Citation149
Because in many instances the information provided by the patients is based on retrospective episodes, and also because sometimes we evaluate reactions that can belong to any of the categories shown above, we provide in the characteristics of any of the clinical entities described as well as the different groups to which they belong in order to help to clarify this.
Because NSAIDs are drugs taken and prescribed for many conditions at all ages they cannot be withdrawn without providing alternatives. Once a subject has been diagnosed as having HDR-NSAID, next step is the management and consists of providing clear measures to follow, which must be written in a intelligible language for patients and also for the physicians who in the future need to know the precise diagnosis in order to make any decision as to which drug to prescribe. The EAACI has considered it useful to provide a consensus document (drug allergy passport) with the recommendations needed for each case written in a clear way and also given, in addition to the native language, in English, thus enabling the document to be consulted in any country.Citation150
One of the major problems in management is when the patients have not been diagnosed, as occurs in all cases of the first episode as well as in many cases that have had several episodes, an allergological workup never has been carried out. In these instances, allergy centers are not available to undertake an appropriate study although in many countries allergy services now have personal facilities to evaluate subjects with drug allergies, including HDR-NSAID.Citation56 Drug allergy is not a permanent condition; in many instances, it is not for ever and in others it may get worse and subjects may need further evaluation.Citation1,Citation14,Citation27 Another reason is that new drugs from the same group are released on the market, and often assessing tolerance to these may be required, as occurs in the case of weak COX-1 or new COX-2 inhibitors.Citation2
With NSAIDs the diagnostic approach not only implies confirming/excluding HDR-NSAID but also providing safe alternatives needed in the cases of CI, as will be detailed below. With SR, once the diagnosis is made, there are easy alternatives unless a very specific drug is particularly useful for the process to be treated.Citation89 This is the case of SNIUAA to propionic derivatives where our evidence now has shown that subjects can be SR to ibuprofen but have good tolerance to other propionic acid derivatives.Citation29 For the other drugs, this must also be considered although cases are rather uncommon. This is the case with selected COX-2 inhibitors where differences in chemical structures and clinical data suggest that an SR to one can develop a reaction to the alternatives. In this sense, this can be extended to oxicams, pyrazolones, and others. Drug allergy management, as is many areas of medicine, is becoming a very personalized approach, and that kind of reasoning may be valuable for physicians on specific occasions.
The other group is SNIDHR and as occurs with BLs,Citation9,Citation10 in addition to group-specific responders selective reactions also occur, like with oxicams and aryl-propionics. If the drug that is provided belongs to the same group but is not the same drug that induced the reaction, and if it was not severe, an approach to assess tolerance can be done. The same measures as for a challenge should apply, although less stringently in order to accommodate the balance of risks/benefits.
For CI, it is now progressively accepted that in a case of a subject with NSAIDs-HDR a search for a safe alternative must be made.Citation50,Citation55 To advise in a case of CI, the safety of paracetamol or even a COX-2 inhibitor must not be taken for granted.Citation151 Nowadays, since the classical division in five major groups with well-defined characteristics, our position is that when we deal with CI and an alternative drug must be given, it is not the same evaluating cases with NERD as those with NIUAA and NIUAA.Citation152 Studies with a sufficient number of cases for providing evidence-based recommendations are lacking, although there are some publications that although not fulfilling the requirements are to some extent valid for following their recommendations.Citation2,Citation14
As an important number of patients suffer from the underlying disease the management must include both pharmacologic and other support measures to treat the whole process. Strong COX-1 inhibitors should be avoided and safe alternatives must be provided. Regarding weak COX-1 inhibitors, preferentially COX-2 with some COX-1 effects or selective COX-2, the general idea is that they are well tolerated although in the case of paracetamol doses higher than 500 mg can lead in some instances to worsening of respiratory symptoms that may even lead to manifest bronchospasm.Citation62,Citation153
Whether these patients are more resistant to classical asthma treatment with CS and B2 inhalers must be considered in severe cases well as inhaled CS, both needed for control.Citation62 The value of panleukast and zileuton was initially emphasized by several manuscripts, although they have not yet attained the generalized use of CS and B2 inhalers.Citation154–Citation157 Regarding biologics, promising avenues are now open with initial evidence from case reports, and a recent study has shown improvement.Citation158–Citation160
NECD. It is assumed in clinical practice that in subjects with CSU, particularly those very active, ASA and other strong COX-1 inhibitors, including piroxicam, may aggravate the clinical course.Citation161,Citation162 Whether this can be extended to weak COX-1 inhibitors or selective COX-2 is not known and the general practice is to administer this with reasonable safety.Citation161,Citation162
NIUA. As occurs with other entities all strong COX-1 inhibitors should be avoided in these patients although some cases tolerate ibuprofen in spite of having a reaction with ASA or other NSAID, though in all instances intolerance to ASA must be proven.Citation3,Citation14,Citation27,Citation30 Cases with any of the clinical entities belonging to this group, if they tolerate ASA, are considered double or triple selective.Citation38 In the case of piroxicam it has been estimated that about 20% of cases may develop symptoms, with 80% having good tolerance,Citation80 but later follow-up of these cases has shown that they can develop mild symptoms after intake (data not published). Other drugs of the group of oxicams are shown to be better tolerated.Citation163 Regarding paracetamol, although generally it is well tolerated, investigators who have studied large series of patients have shown that up to 19% of cases may have symptoms after intake.Citation164 Better tolerance is shown with selective COX-2 inhibitors, although a low percentage of cases (about 10%) may develop symptoms.Citation165 Another alternative drug that has been tested, not available in many countries, is nabumetone that has been shown to be well tolerated.Citation166 More recently, a new drug, tiaramide, has been shown to be well tolerated in a reduced number of cases in a Japanese study.Citation167,Citation168
SNIUA. The choice in this entity is to look for an alternative drugCitation80,Citation89 but if any of these drugs must be administered a desensitization procedure must be considered, as shown below. It is expected that with the progress made in the understanding of drugs involved in the prostaglandin–leukotriene pathways, any of the NSAIDs now in use may have specific beneficial/detrimental effects that will in the future need to be considered independently.
Because of the relevance of NSAIDs and considering that they are drugs of absolute necessity, if no alternatives are available, desensitization is an option that can be considered in special cases.Citation80 Also, dispensation has been used in the management of those cases that within the NERD group have a poor evolution.Citation62,Citation169–Citation171 The rationale is different than that for IgE-mediated reactions but the final outcomes pursued are similar, to induce some type of tachyphylaxis although additional mechanisms have recently been proposed.Citation73
For NSAID, desensitization ASA is given at initial doses of 40.5 mg with increasing doses given over a period of 1–3 days till achieving a final dose of 325 mg. During this period in some cases minor symptoms appear that can be transitory. Then the dose can be maintained from 325 to 650 mg of ASA daily. This treatment is then maintained over a long time during which patients experience decrease in nasal swelling, better breathing by the nose but no change in the presence of asthma. This approach, initially made at the Scrip Clinic by Stevenson et al, has been now generalized to many American centers and also other located all over the world including Europe.Citation172 Several protocols have been used and, although they have apparent differences, they, nevertheless, follow the same rational strategy with the use of omalizumab in some cases that may help in the success of the procedure. For further details, we recommend the recent review published by the ENDA study group on NERD.Citation62 In cases of NECD, desensitization has been less studied and it is not easy to find cases where we can envisage this.Citation173 Because the number of patients treated so far is rather low and adverse effects have been reported, we do not know if cases with NECD are more resistant to ASA desensitization. In any case, in any potential scenario where a certain NSAID is needed, the general approaches made for NERD are also valid here.Citation62 Finally, concerning desensitization in SNIUAA no cases yet exist and as far as we are aware no information is available in the medical literature, as can be seen by introducing appropriate key words in PubMed or other database sources.
Concluding remarks
Increasing worldwide evidence in the last year supported by many groups is showing that NSAIDs are the most important drug involved in HDR. This observation extends to children and the older people although in these ages more evidence is still needed for supporting the observations made in adults and adolescents. Due to the lack of well-validated in vitro and in vivo tests like skin testing for the diagnosis, DPT is the sole approach in most instances to verify tolerance or confirm hypersensitivity. This requires that many centers involved in drug allergy evaluation include in their services special units dedicated to evaluate drug allergy with the required facilities and trained personnel for the diagnosis and management of NSAID-HDR. As the use of these drugs including selective COX-2 inhibitors goes on increasing, this approach must be warranted in allergy services.
Abbreviations
Ab, antibodies; ADR, adverse drug reactions; AGEP, acute generalized exanthematic pustulosis; ASA, acetyl salicylic acid; AX, amoxicillin; AX-CLAV, amoxicillin-clavulanic acid; BLs, betalactams; CD, contact dermatitis; CI, cross-intolerance; COX, cyclooxygenase; COX-1, cyclooxygenase-1; COX-2, cyclooxygenase-2; CS, corticosteroid; CSU, chronic spontaneous urticaria; DRESS, drug rash with eosinophilia and systemic symptoms; DPT, drug provocation test; EAACI, European Academy of Allergy and Clinical Immunology; ENDA, European Network for Drug Allergy; FDE, fixed drug eruption; GI, gastrointestinal; HDR, hypersensitivity drug reactions; HDR-NSAIDs, hypersensitivity drug reactions to NSAIDs; LOX, lipo-oxygenase; MPE, maculopapular exanthema; NECD, NSAIDs-exacerbated cutaneous disease; NERD, NSAIDs exacerbated respiratory disease; NIU, nonimmediate urticaria; NIUA, NSAID-induced urticaria angioedema; NSAIDs, non-steroidal anti-inflammatory drugs; RIRAAF, Spanish National Network for the Study of Adverse Drug Reactions; sIgE, specific IgE; SJS-TEN, Steven Johnson Syndrome – toxic epidermal necrolysis; SNIDR, single NSAID-induced delayed reactions; SNIUAA, single NSAID-induced urticaria, angioedema, and anaphylaxis; SR, selective responders.
Acknowledgments
This work is supported by fundings as well as grants PI15/00726 and RD16/0006/0024, from the NIH, the Carlos III Health Institute (ISCIII), ARADYAL and FEDER to N Blanca-Lopez, V Soriano, E Garcia-Martin, G Canto, and M Blanca.
Disclosure
The authors report no conflicts of interest in this work.
References
- Doña I, Blanca-López N, Torres MJ, et al. Drug hypersensitivity reactions: response patterns, drug involved, and temporal variations in a large series of patients. J Investig Allergol Clin Immunol. 2012;22(5):363–371.
- Blanca-López N, Pérez-Alzate D, Canto G, Blanca M. Practical approach to the treatment of NSAID hypersensitivity. Expert Rev Clin Immunol. 2017;13(11):1017–1027.28893093
- Doña I, Blanca-López N, Cornejo-García JA, et al. Characteristics of subjects experiencing hypersensitivity to non-steroidal anti-inflammatory drugs: patterns of response. Clin Exp Allergy. 2011;41(1):86–95.21155908
- Messaad D, Sahla H, Benahmed S, et al. Drug provocation tests in patients with a history suggesting an immediate drug hypersensitivity reaction. Ann Intern Med. 2004;140(12):1001–1006.15197017
- Jares EJ, Baena-Cagnani CE, Sánchez-Borges M, et al. Drug-induced anaphylaxis in Latin American countries. J Allergy Clin Immunol Pract. 2015;3(5):780–788.26143020
- Çelik G, Pichler WJ, Adkinson NF. Drug allergy. In: Adkinson NF, Brocher BS, Busse WW, Holgate ST, Lemanske RF, Simons FER. Middleton’s Allergy Principles & Practise. Vol 2 7th ed. St. Louis, MO: Mosby Elsevier; 2009; Chapter 68: 1205–1226.
- Zhou L, Dhopeshwarkar N, Blumenthal KG, et al. Drug allergies documented in electronic health records of a large healthcare system. Allergy. 2016;71(9):1305–1313.26970431
- Xing Y, Zhang H, Sun S, et al. Clinical features and treatment of pediatric patients with drug-induced anaphylaxis: a study based on pharmacovigilance data. Eur J Pediatr. 2018;177(1):145–154.29168013
- Blanca M. Allergic reactions to amoxicillin. A changing world? Allergy. 1995;50:772–782.
- Blanca M, Mayorga C, Torres MJ, et al. Side-chain-specific reactions to betalactams: 14 years later. Clin Exp Allergy. 2002;32(2):192–197.11929481
- Brunton LL, Hilal-Dandan R, Knollmann BC. Goodman and Gilman´s: The Pharmacological Basis of Therapeutics. 13th ed. New York: McGrawHill; 2017.
- Szczeklik A, Nizankowska-Mogilnicka E, Sanak M. Hypersensitivity to aspirin and non-steroidal antiinflammatory drugs. In: Adkinson NF, Brocher BS, Busse WW, Holgate ST, Lemanske RF, Simons FER, editors. Middleton´s Allergy Principles & Practise. Vol 2 7th ed. St. Louis, MO: Mosby Elsevier; 2009; Chapter 69: 1227–1243.
- Network for the Study of Adverse Reactions to Drug and Allergens (RIRAAF). ISCiii, Madrid, Spain. Available from: https://chirimoyo.ac.uma.es/riraaf/. Accessed February 2, 2019.
- Blanca-López N, Barrionuevo E, Andreu I, Canto MG. Hypersensitivity reactions to nonsteroidal anti-inflammatory drugs: from phenotyping to genotyping. Curr Opin Allergy Clin Immunol. 2014;14(4):271–277.24915547
- Ayuso P, Cornejo-García JA, Blanca-López N, Doña I. Advanced phenotyping in hypersensitivity drug reactions to NSAIDs. Clin Exp Allergy. 2013;43(10):1097–1109.24074328
- Gómez F, Perkins JR, García-Martín E, Canto G, Cornejo-García JA. Genetic basis of hypersensitivity reactions to nonsteroidal anti-inflammatory drugs. Curr Opin Allergy Clin Immunol. 2015;15(4):285–293.26110677
- Plaza-Serón MDC, García-Martín E, Agúndez JA, Ayuso P. Hypersensitivity reactions to nonsteroidal anti-inflammatory drugs: an update on pharmacogenetics studies. Pharmacogenomics. 2018;19(13):1069–1086.30081739
- Perkins JR, Barrionuevo E, Ranea JA, Blanca M, Cornejo-Garcia JA. Systems biology approaches to enhance our understanding of drug hypersensitivity reactions. Clin Exp Allergy. 2014;44(12):1461–1472.25040150
- Pham DL, Jim JH, Park HS. What we know about non-steroidal drug hypersensitivity. Korean J Intern Med. 2016;3:417–432.
- Kim SH, Sanak M, Park HS. Genetics of hypersensitivity to aspirin and nonsteroidal anti-inflammatory drugs. Immunol Allergy Clin North Am. 2013;33(2):177–194.23639707
- Kidon M, Blanca-Lopez N, Gomes E, et al. EAACI/ENDA position paper: diagnosis and management of hypersensitivity reactions to non-steroidal anti-inflammatory drugs (NSAIDs) in children and adolescents. Pediatr Allergy Immunol. 2018;29(5):469–480.29693290
- Blanca-López N, Pérez-Alzate D, Somoza ML, et al. Pattern of responses of hypersensitivity reactions to NSAIDs in adolescents and young adults. Allergy. 2018;73(S105):1757.
- Guéant JL, Romano A, Cornejo-Garcia JA, et al. HLA-DRA variants predict penicillin allergy in genome-wide fine-mapping genotyping. J Allergy Clin Immunol. 2015;135(1):253–259.25224099
- Rajan JP, Wineinger NE, Stevenson DD, White AA. Prevalence of aspirin-exacerbated respiratory disease among asthmatic patients: a meta-analysis of the literature. J Allergy Clin Immunol. 2015;135(3):676–681.25282015
- Bavbek S, Yılmaz İ, Çelik G, et al. Prevalence of aspirin-exacerbated respiratory disease in patients with asthma in Turkey: a cross-sectional survey. Allergol Immunopathol. 2012;40(4):225–230.
- Hayashi H, Mitsui C, Nakatani E, et al. Omalizumab reduces cysteinyl leukotriene and 9α,11β-prostaglandin F2 overproduction in aspirin-exacerbated respiratory disease. J Allergy Clin Immunol. 2016;137(5):1585–1587.26559322
- Blanca-López N, Torres JM, Doña I, et al. Value of the clinical history in the diagnosis of urticaria/angioedema induced by NSAIDs with cross-intolerance. Clin Exp Allergy. 2013;43(1):85–91.23278883
- Asero R. Single NSAID hypersensitivity is associated with atopic status. Eur Ann Allergy Clin Immunol. 2015;47(2):48–53.25781194
- Blanca-López N, Pérez-Alzate D, Andreu I, et al. Immediate hypersensitivity reactions to ibuprofen and other arylpropionic acid derivatives. Allergy. 2016;71(7):1048–1056.26841325
- Blanca-López N, Bogas G, Doña I, et al. ASA must be given to classify multiple NSAID-hypersensitivity patients as selective or cross-intolerant. Allergy. 2016;71(4):576–578.27003105
- Pérez-Alzate D, Cornejo-García JA, Pérez-Sánchez N, et al. Immediate reactions to more than 1 NSAID must not be considered cross-hypersensitivity unless tolerance to ASA is verified. J Investig Allergol Clin Immunol. 2017;27(1):32–39.
- Pérez-Alzate D, Blanca-López N, Doña I, et al. Asthma and rhinitis induced by selective immediate reactions to paracetamol and non-steroidal anti-inflammatory drugs in aspirin tolerant subjects. Front Pharmacol. 2016;7:215.27489545
- Blanca-López N, Doña I, Perkins JR, et al. Multiple nonsteroidal anti-inflammatory drug-induced cutaneous disease: relevance, natural evolution and relationship with atopy. Int Arch Allergy Immunol. 2014;164(2):147–148.25012690
- Tuttle KL, Schneider TR, Henrickson SE, et al. Aspirin-exacerbated respiratory disease: not always “adult-onset”. J Allergy Clin Immunol Pract. 2016;4(4):756–758.27393784
- Ertoy Karagol HI, Yilmaz O, Topal E, Ceylan A, Bakirtas A. Nonsteroidal anti-inflammatory drugs-exacerbated respiratory disease in adolescents. Int Forum Allergy Rhinol. 2015;5(5):392–398.25755210
- Cavkaytar O, Arik Yilmaz E, Karaatmaca B, et al. Different phenotypes of non-steroidal anti-inflammatory drug hypersensitivity during childhood. Int Arch Allergy Immunol. 2015;167(3):211–221.26315297
- Yilmaz O, Ertoy Karagol IH, Bakirtas A, et al. Challenge-proven nonsteroidal anti-inflammatory drug hypersensitivity in children. Allergy. 2013;68(12):1555–1561.24117618
- Blanca M, Garcia J, Vega JM, et al. Anaphylaxis to penicillins after non-therapeutic exposure: an immunological investigation. Clin Exp Allergy. 1996;26(3):335–340.8729672
- Demir S, Olgac M, Unal D, et al. Evaluation of hypersensitivity reactions to nonsteroidal anti-inflammatory drugs according to the latest classification. Allergy. 2015;70(11):1461–1467.26173603
- Caimmi S, Caimmi D, Bousquet PJ, Demoly P. How can we better classify NSAID hypersensitivity reactions?–validation from a large database. Int Arch Allergy Immunol. 2012;159(3):306–312.22739440
- Kidon MI, Liew WK, Chiang WC, et al. Hypersensitivity to paracetamol in Asian children with early onset of nonsteroidal anti-inflammatory drug allergy. Int Arch Allergy Immunol. 2007;144(1):51–56.17505137
- Cornejo-García JA, Liou LB, Blanca-López N, et al. Genome-wide association study in NSAID-induced acute urticaria/angioedema in Spanish and Han Chinese populations. Pharmacogenomics. 2013;14(15):1857–1869.24236485
- Alves C, Romeira AM, Abreu C, et al. Non-steroidal anti-inflammatory drug hypersensitivity in children. Allergol Immunopathol. 2017;45(1):40–47.
- Hassani A, Ponvert C, Karila C, et al. Hypersensitivity to cyclooxygenase inhibitory drugs in children: a study of 164 cases. Eur J Dermatol. 2008;18(5):561–565.18693161
- Kidon MI, Kang LW, Chin CW, et al. Early presentation with angioedema and urticaria in cross-reactive hypersensitivity to nonsteroidal antiinflammatory drugs among young, Asian, atopic children. Pediatrics. 2005;116(5): e675–e680.
- Cavkaytar O, Arik Yilmaz E, Buyuktiryaki B, et al. Challenge-proven aspirin hypersensitivity in children with chronic spontaneous urticaria. Allergy. 2015;70(2):153–160.25353369
- Calvo Campoverde K, Giner-Muñoz MT, Martínez Valdez L, et al. Hypersensitivity reactions to non-steroidal anti-inflammatory drugs and tolerance to alternative drugs. An Pediatr (Barc). 2016;84:148–153.26195066
- Ameratunga R, Randall N, Dalziel S, Anderson BJ. Samter’s triad in childhood: a warning for those prescribing NSAIDs. Paediatr Anaesth. 2013;23(8):757–759.23782034
- Blanca-López N, Cornejo-García JA, Pérez-Alzate D, et al. Hypersensitivity reactions to nonsteroidal anti-inflammatory drugs in children and adolescents: selective reactions. J Investig Allergol Clin Immunol. 2015;25(6):385–395.
- Blanca-López N, Cornejo-García JA, Plaza-Serón MC, et al. Hypersensitivity to nonsteroidal anti-inflammatory drugs in children and adolescents: cross-intolerance reactions. J Investig Allergol Clin Immunol. 2015;25(4):259–269.
- Lovell DJ, Dare JA, Francis-Sedlak M, et al. A 6-month, multicenter, open-label study of fixed dose naproxen/esomeprazole in adolescent patients with juvenile idiopathic arthritis. Pediatr Rheumatol Online J. 2018;16(1):41.29941047
- Predel HG, Giannetti B, Connolly MP, Lewis F, Bhatt A. Efficacy and tolerability of a new ibuprofen 200 mg plaster in patients with acute sports-related traumatic blunt soft tissue injury/contusion. Postgrad Med. 2018;130(1):24–31.29110567
- Predel HG, Connolly MP, Bhatt A, et al. Efficacy and safety assessment of acute sports-related traumatic soft tissue injuries using a new ibuprofen medicated plaster: results from a randomized controlled clinical trial. Phys Sportsmed. 2017;45(4):418–425.28926295
- Kowalski ML, Makowska JS, Blanca M, et al. Hypersensitivity to nonsteroidal anti-inflammatory drugs (NSAIDs) - classification, diagnosis and management: review of the EAACI/ENDA(#) and GA2LEN/HANNA*. Allergy. 2011;66(7):818–829.21631520
- Kowalski ML, Asero R, Bavbek S, et al. Classification and practical approach to the diagnosis and management of hypersensitivity to nonsteroidal anti-inflammatory drugs. Allergy. 2013;68(10):1219–1232.24117484
- Blanca-López N, Somoza-Alvarez ML, Bellon T, et al. NSAIDs hypersensitivity: questions not resolved. Curr Opin Allergy Clin Immunol. 2018;18(4):291–301.29878898
- Cahill KN, Boyce JA. Aspirin-exacerbated respiratory disease: mediators and mechanisms of a clinical disease. J Allergy Clin Immunol. 2017;139(3):764–766.27771324
- Buchheit KM, Cahill KN, Katz HR, et al. Thymic stromal lymphopoietin controls prostaglandin D2 generation in patients with aspirin-exacerbated respiratory disease. J Allergy Clin Immunol. 2016;137(5):1566–1576.26691435
- Pérez-Novo CA, Watelet JB, Claeys C, van Cauwenberge P, Bachert C. Prostaglandin, leukotriene, and lipoxin balance in chronic rhinosinusitis with and without nasal polyposis. J Allergy Clin Immunol. 2005;115(6):1189–1196.15940133
- Steinke JW, Negri J, Liu L, Payne SC, Borish L. Aspirin activation of eosinophils and mast cells: implications in the pathogenesis of aspirin-exacerbated respiratory disease. J Immunol. 2014;193(1):41–47.24890720
- Fajmut A, Emeršič T, Dobovišek A, et al. Dynamic model of eicosanoid production with special reference to non-steroidal anti-inflammatory drug-triggered hypersensitivity. IET Syst Biol. 2015;9(5):204–215.26405144
- Kowalski ML, Agache I, Bavbek S, et al. Diagnosis and management of NSAID-exacerbated respiratory disease (N-ERD)-a EAACI position paper. Allergy. 2019;74(1):28–39.30216468
- Liu T, Laidlaw TM, Katz HR, Boyce JA. Prostaglandin E2 deficiency causes a phenotype of aspirin sensitivity that depends on platelets and cysteinyl leukotrienes. Proc Natl Acad Sci U S A. 2013;110(42):16987–16992.24085850
- Aktas A, Kurt E, Gulbas Z. Cytokine expression before and after aspirin desensitization therapy in aspirin-exacerbated respiratory disease. Inflammation. 2013;36(6):1553–1559.23912646
- Samter M, Beers RF Jr. Intolerance to aspirin. Clinical studies and consideration of its pathogenesis. Ann Intern Med. 1968;68(5):975–983.5646829
- Bavbek S, Celik G, Demirel YS, Misirligil Z. Risk factors associated with hospitalizations for asthma attacks in turkey. Allergy Asthma Proc. 2003;24(6):437–442.14763246
- Makowska JS, Burney P, Jarvis D, et al. Respiratory hypersensitivity reactions to NSAIDs in Europe: the global allergy and asthma network (GA(2)LEN) survey. Allergy. 2016;71:1603–1611.27230252
- Morales DR, Guthrie B, Lipworth BJ, et al. NSAID-exacerbated respiratory disease: a meta-analysis evaluating prevalence, mean provocative dose of aspirin and increased asthma morbidity. Allergy. 2015;70(7):828–835.25855099
- Cavkaytar O, Arik Yilmaz E, Karaatmaca B, et al. Different phenotypes of non-steroidal anti-inflammatory drug hypersensitivity during childhood. Int Arch Allergy Immunol. 2015;167(3):211–221.26315297
- Pérez-Alzate D, Blanca-López N, Doña I, et al. Asthma and rhinitis induced by selective immediate reactions to paracetamol and non-steroidal anti-inflammatory drugs in aspirin tolerant subjects. Front Pharmacol. 2016;7:215.27489545
- Palikhe S, Palikhe NS, Kim SH, et al. Elevated platelet activation in patients with chronic urticaria: a comparison between aspirin-intolerant and aspirin-tolerant groups. Ann Allergy Asthma Immunol. 2014;113(3):276–281.25037610
- Aun MV, Blanca M, Garro LS, et al. Nonsteroidal anti-inflammatory drugs are major causes of drug-induced anaphylaxis. J Allergy Clin Immunol Pract. 2014;2(4):414–420.25017529
- Mastalerz L, Setkowicz M, Sanak M, Szczeklik A. Hypersensitivity to aspirin: common eicosanoid alterations in urticaria and asthma. J Allergy Clin Immunol. 2004;113(4):771–775.15100686
- Lee HY, Ye YM, Kim SH, et al. Identification of phenotypic clusters of nonsteroidal anti-inflammatory drugs exacerbated respiratory disease. Allergy. 2017;72(4):616–626.27805264
- Campo P, Ayuso P, Salas M, et al. Mediator release after nasal aspirin provocation supports different phenotypes in subjects with hypersensitivity reactions to NSAIDs. Allergy. 2013;68(8):1001–1007.23889565
- Zambonino MA, Torres MJ, Muñoz C, et al. Drug provocation tests in the diagnosis of hypersensitivity reactions to non-steroidal anti-inflammatory drugs in children. Pediatr Allergy Immunol. 2013;24(2):151–159.23506290
- Kowalski ML, Stevenson DD. Classification of reactions to nonsteroidal antiinflammatory drugs. Immunol Allergy Clin North Am. 2013;33(2):135–145.23639704
- Ortega Rodriguez NR, Doña Díaz I, Blanca-López N, et al. Hipersensibilidad a los antiinflamatorios no esteroideos. In: Dávila González IJ, Jáuregui Presa I, Olaguibel Rivera JM, Zubeldia Ortuño JM, editors. Tratado de Alergología. 2nd edition. Madrid: Ergon; 2016; Vol 4, Chapter 19: 1551–1570.
- Giner MT. Alergia a Fármacos. In: Martín Mateos MA, editor. Tratado de Alergología Pediátrica. 2nd ed. Madrid: Ergon; 2011 Chapter 20: 247–263.
- Blanca-López N, Pérez-Alzate D, Canto G, Blanca M. Practical approach to the treatment of NSAID hypersensitivity. Expert Rev Clin Immunol. 2017;13(11):1017–1027.28893093
- Szczeklik A, Nizankowska E, Duplaga M. Natural history of aspirin-induced asthma. AIANE Investigators. European Network on aspirin-induced asthma. Eur Respir J. 2000;16(3):432–436.11028656
- Carmona MJ, Blanca M, Garcia A, et al. Intolerance to piroxicam in patients with adverse reactions to nonsteroidal antiinflammatory drugs. J Allergy Clin Immunol. 1992; 90(6 Pt 1):873–879.1460195
- Setkowicz M, Mastalerz L, Podolec-Rubis M, et al. Clinical course and urinary eicosanoids in patients with aspirin-induced urticaria followed up for 4 years. J Allergy Clin Immunol. 2009;123:174–178.18842291
- Capone ML, Tacconelli S, Di Francesco L, Sacchetti A, Sciulli MG, Patrignani P. Pharmacodynamic of cyclooxygenase inhibitors in humans. Prostaglandins Other Lipid Mediat. 2007;82(1–4):85–94.17164136
- Pérez-Sánchez N, Bogas G, Cornejo-García JA, et al. Multiple nonsteroidal anti-inflammatory drug hypersensitivity without hypersensitivity to aspirin. J Allergy Clin Immunol Pract. 2016;4(3):524–525.26781480
- Macías E, Ruiz A, Moreno E, et al. Usefulness of intradermal test and patch test in the diagnosis of nonimmediate reactions to metamizol. Allergy. 2007;62(12):1462–1464.17983381
- Loh TY, Cohen PR. Ketoprofen-induced photoallergic dermatitis. Indian J Med Res. 2016;144(6):803–806.28474616
- Monteiro AF, Rato M, Martins C. Drug-induced photosensitivity: photoallergic and phototoxic reactions. Clin Dermatol. 2016;34(5):571–581.27638435
- Canto MG, Andreu I, Fernandez J, Blanca M. Selective immediate hypersensitivity reactions to NSAIDs. Curr Opin Allergy Clin Immunol. 2009;9(4):293–297.19561490
- Borja JM, Galindo PA, Gomez E, Feo F. Delayed skin reactions to metamizol. Allergy. 2003;58(1):84–85.12580814
- Angadi SS, Karn A. Ibuprofen induced Stevens-Johnson syndrome – toxic epidermal necrolysis in Nepal. Asia Pac Allergy. 2016;6(1):70–73.26844223
- Gulin SJ, Chiriac A. Diclofenac-Induced allergic contact dermatitis: a series of four patients. Drug Saf Case Rep. 2016;3(1):15.27882527
- Gómez E, Blanca-López N, Torres MJ, et al. Immunoglobulin E-mediated immediate allergic reactions to dipyrone: value of basophil activation test in the identification of patients. Clin Exp Allergy. 2009;39(8):1217–1224.19400910
- Himly M, Jahn-Schmid B, Pittertschatscher K, et al. IgE-mediated immediate-type hypersensitivity to the pyrazolone drug propyphenazone. J Allergy Clin Immunol. 2003;111(4):882–888.12704373
- Ariza A, García-Martín E, Salas M, et al. Pyrazolones metabolites are relevant for identifying selective anaphylaxis to metamizole. Sci Rep. 2016;6:23845.27030298
- Blanca M, Perez E, Garcia JJ, et al. Angioedema and IgE antibodies to aspirin: a case report. Ann Allergy. 1989;62(4):295–298.2468301
- Harrer A, Lang R, Grims R, et al. Diclofenac hypersensitivity: antibody responses to the parent drug and relevant metabolites. PLoS One. 2010;5(10):e13707.21060839
- Levy M, Zylber-Katz E, Rosenkranz B. Clinical pharmacokinetics of dipyrone and its metabolites. Clin Pharmacokinet. 1995;28(3):216–234.7758252
- Herdeg C, Hilt F, Büchtemann A, Bianchi L, Klein R. Allergic cholestatic hepatitis and exanthema induced by metamizole: verification by lymphocyte transformation test. Liver. 2002;22(6):507–513.12445177
- Federmann G, Becker EW, Tautorat H, Penschuck C, Berg PA. [Demonstration by lymphocyte transformation test of the allergic genesis in a case of acute hepatitis]. Dtsch Med Wochenschr. 1988;113(43):1676–1679. German.2903041
- Mockenhaupt M. Epidemiology of cutaneous adverse drug reactions. Chem Immunol Allergy. 2012;97:1–17.22613850
- Drucker AM, Rosen CF. Drug-induced photosensitivity: culprit drugs, management and prevention. Drug Saf. 2011;34(10):821–837.21879777
- Marchand MS, Autret-Leca E, Bourdais E, Jonville-Béra AP. [Photoallergy to piroxicam: what should be contraindicates?]. Therapie. 2013;68(1):57–58. French.23484664
- Chen CB, Abe R, Pan RY, et al. An updated review of the molecular mechanisms in drug hypersensitivity. J Immunol Res. 2018;2018(3):1–22.
- Lerch M, Mainetti C, Terziroli Beretta-Piccoli B, Harr T. Current perspectives on Stevens-Johnson syndrome and toxic epidermal necrolysis. Clin Rev Allergy Immunol. 2018;54(1):147–176.29188475
- Balta I, Simsek H, Simsek GG. Flurbiprofen-induced generalized bullous fixed drug eruption. Hum Exp Toxicol. 2014;33(1):106–108.23703815
- Rho YK, Yoo KH, Kim BJ, Kim MN, Song KY. A case of generalized fixed drug eruption due to a piroxicam plaster. Clin Exp Dermatol. 2010;35(2):204–205.20447085
- Arochena L, Zafra MP, Fariña MC, del Pozo V, Fernández-Nieto M. Acute generalized exanthematic pustulosis due to ibuprofen. Ann Allergy Asthma Immunol. 2013;110(5):386–387.23622012
- di Meo N, Stinco G, Patrone P, Trevisini S, Trevisan G. Acute localized exanthematous pustulosis caused by flurbiprofen. Cutis. 2016;98(5):E9–E11.28040819
- Gómez E, Blanca-Lopez N, Salas M, et al. Induction of accelerated reactions to amoxicillin by T-cell effector mechanisms. Ann Allergy Asthma Immunol. 2013;110(4):267–273.23535091
- Parra FM, Pérez Elias MJ, Cuevas M, Ferreira A. Serum sickness-like illness associated with rifampicin. Ann Allergy. 1994;73(2):123–125.8067595
- Kraleti S, Khatri N, Jarrett D. Serum sickness-like reaction after the treatment of cellulitis with amoxicillin/clavulanate. J Ark Med Soc. 2016;112:278–280.27434982
- Watanabe T, Abe M, Tada F, et al. Drug-induced liver injury with serious multiform exudative erythema following the use of an over-the-counter medication containing ibuprofen. Intern Med. 2015;54(4):395–399.25748955
- Schmutz JL, Barbauda A, Trechot P. [Phenylbutazone and dress syndrome]. Ann Dermatol Venereol. 2010;137:857.21134594
- Karmacharya P, Mainali NR, Aryal MR, et al. Recurrent case of ibuprofen-induced aseptic meningitis in mixed connective tissue disease. Case Rep. 2013; 2013: bcr2013009571.
- Baxter KA, Pucher PH, Berry DP, et al. The effect of non-steroidal anti-inflammatory drugs on severity of acute pancreatitis and pancreatic necrosis. Ann R Coll Surg Engl. 2018;100(3):199–202.29181999
- Aynioglu A, Elicora A, Kaya S. Nicolau syndrome due to diclofenac injection. G Ital Dermatol Venereol. 2016;151(4):452–453.27348328
- Arikoglu T, Aslan G, Yildirim DD, et al. Discrepancies in the diagnosis and classification of non-sdteroidal anti-inflammatory drugs hypersensitivity reactions in chlidren. Alergolo Int. 2017;66:418–24.
- Avorn J. The role of Pharmacoepidemiology in the Health-Care System and Academia. In: Strom BL, Kimmel SE, Hennessy S, editors. Pharmacoepidemiology 5th ed. Hoboken, NJ: Wiley-Blackwell; 2012; Chapter 6: 73–83.
- Oosterhuis I, Zweers P, Rümke H, Muller-Hansma A, van Puijenbroek EP. A tailor-made approach for causality assessment for ADR reports on drugs and vaccines. Pharmacoepidemiol Drug Saf. 2018;17(6).
- Nguyen KD, Tran TN, Nguyen MT, et al. Drug-induced Stevens-Johnson syndrome and toxic epidermal necrolysis in Vietnamese spontaneous adverse drug reaction database: a subgroup approach to disproportionality analysis. J Clin Pharm Ther. 2019;44(1):69–77.30129156
- Kesselheim A. pharmacoepidemiology and the law In: Strom BL, Kimmel SE, Hennessy S, editors. Pharmacoepidemiology. 5th ed. Hoboken: Wiley-Blackwell; 2012; Chapter 9: 117–134.
- Cortellini G, Romano A, Santucci A, et al. Clinical approach on challenge and desensitization procedures with aspirin in patients with ischemic heart disease and nonsteroidal anti-inflammatory drug hypersensitivity. Allergy. 2017;72(3):498–506.27732743
- Al-Ahmad M, Rodriguez-Bouza T, Nurkic M. Establishing a safe administration of ASA in cardiovascular patients with nonsteroidal anti-inflammatory drug hypersensitivity with skin and/or respiratory involvement. Int Arch Allergy Immunol. 2018;175(4):237–245.29393216
- Jenkins C, Costello J, Hodge L. Systematic review of prevalence of aspirin induced asthma and its implications for clinical practice. BMJ. 2004;328(7437):434.14976098
- Cardet JC, White AA, Barrett NA, et al. Alcohol-induced respiratory symptoms are common in patients with aspirin exacerbated respiratory disease. J Allergy Clin Immunol Pract. 2014;2(2):208–213.24607050
- Cornejo-Garcia J, Oussalah A, Blanca M, et al. Genetic predictors of drug hypersensitivity. Curr Pharm Des. 2017;22(45):6725–6733.
- Cherrez-Ojeda I, Robles-Velasco K, Bedoya-Riofrío P, et al. Checklist for a complete chronic urticaria medical history: an easy tool. World Allergy Organ J. 2017;10(1):34.29043012
- Doeglas HM. Reactions to aspirin and food additives in patients with chronic urticaria, including the physical urticarias. Br J Dermatol. 1975;93(2):135–144.1100092
- Doña I, Blanca-López N, Torres MJ, et al. NSAID-induced urticaria/angioedema does not evolve into chronic urticaria: a 12-year follow-up study. Allergy. 2014;69(4):438–444.24372026
- Goeschke B, Braathen LR. Acute generalized exanthematic pustulosis: a case and an overview of side effects affecting the skin caused by celecoxib and other COX-2 inhibitors reported so far. Dermatology. 2004;209(1):53–56.15237269
- Hanafusa T, Azukizawa H, Matsumura S, et al. Non-pigmenting fixed drug eruption caused by an over-the-counter non-steroidal anti-inflammatory drug: drug-specific CD8+ T lymphocytes identified in peripheral blood. Eur J Dermatol. 2012;22(5):680–682.22854000
- Roujeau J-C, Albengres E, Moritz S, et al. Lymphocyte transformation test in drug-induced toxic epidermal necrolysis. Int Arch Allergy Immunol. 1985;78(1):22–24.
- Stevens WW, Schleimer RP. Aspirin-exacerbated respiratory disease as an endotype of chronic rhinosinusitis. Immunol Allergy Clin North Am. 2016;36(4):669–680.27712762
- Lee HY, Ye YM, Kim SH, et al. Identification of phenotypic clusters of nonsteroidal anti-inflammatory drugs exacerbated respiratory disease. Allergy. 2017;72(4):616–626.27805264
- Pali-Schöll I, Untersmayr E, Klems M, Jensen-Jarolim E, et al. The effect of digestion and digestibility on allergenicity of food. Nutrients. 2018;10(9):1129.
- Fisher HR, du Toit G, Bahnson HT, et al. The challenges of preventing food allergy: lessons learned from leap and eat. Ann Allergy Asthma Immunol. 2018;121:313–319.29909054
- Blanca-López N, Haroun-Diaz E, Ruano FJ, et al. Acetyl salicylic acid challenge in children with hypersensitivity reactions to nonsteroidal anti-inflammatory drugs differentiates between cross-intolerant and selective responders. J Allergy Clin Immunol Pract. 2018;6(4):1226–1235.28986120
- Fokkens WJ, Lund VJ, Mullol J, et al. EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists. Rhin. 2012;50(1):1–12.
- Bavbek S, Yılmaz İ, Çelik G, et al. Prevalence of aspirin-exacerbated respiratory disease in patients with asthma in Turkey: a cross-sectional survey. Allergol Immunopathol. 2012;40(4):225–230.
- Posadas SJ, Leyva L, Torres MJ, et al. Subjects with allergic reactions to drugs show in vivo polarized patterns of cytokine expression depending on the chronology of the clinical reaction. J Allergy Clin Immunol. 2000;106(4):769–776.11031349
- Blanca M, Posadas S, Torres MJ, et al. Expression of the skin-homing receptor in peripheral blood lymphocytes from subjects with nonimmediate cutaneous allergic drug reactions. Allergy. 2000;55(11):998–1004.11097307
- Bellón T, Alvarez L, Mayorga C, et al. Differential gene expression in drug hypersensitivity reactions: induction of alarmins in severe bullous diseases. Br J Dermatol. 2010;162(5):1014–1022.20030638
- Romano A, Blanca M, Torres MJ, et al. Diagnosis of nonimmediate reactions to beta-lactam antibiotics. Allergy. 2004;59(11):1153–1160.15461594
- Dalmau J, Serra-Baldrich E, Roé E, Peramiquel L, Alomar A. Use of patch test in fixed drug eruption due to metamizole (Nolotil). Contact Derm. 2006;54(2):127–128.
- Macías E, Ruiz A, Moreno E, et al. Usefulness of intradermal test and patch test in the diagnosis of nonimmediate reactions to metamizol. Allergy. 2007;62(12):1462–1464.17983381
- Romano A, Pietrantonio F, Di Fonso M, et al. Positivity of patch tests in cutaneous reaction to diclofenac. Two case reports. Allergy. 1994;49(1):57–59.8198241
- Marques LP, Villarinho ALCF, Melo MDGM, Torre MGS. Fixed drug eruption to nimesulide: an exuberant presentation confirmed by patch testing. An Bras Dermatol. 2018;93(3):470–472.29924254
- Kerr A, Ferguson J. Photoallergic contact dermatitis. Photodermatol Photoimmunol Photomed. 2010;26(2):56–65.20415735
- Brockow K, Aberer W, Atanaskovic-Markovic M, et al. Drug allergy passport and other documentation for patients with drug hypersensitivity – an ENDA/EAACI Drug Allergy Interest Group Position Paper. Allergy. 2016;71(11):1533–1539.27145347
- Doña I, Blanca-López N, Jagemann LR, et al. Response to a selective COX-2 inhibitor in patients with urticaria/angioedema induced by nonsteroidal anti-inflammatory drugs. Allergy. 2011;66(11):1428–1433.21834936
- Torres MJ, Barrionuevo E, Kowalski M, Blanca M. Hypersensitivity reactions to nonsteroidal anti-inflammatory drugs. Immunol Allergy Clin North Am. 2014;34(3):507–524.25017675
- Kowalski ML, Makowska J. Use of nonsteroidal anti-inflammatory drugs in patients with aspirin hypersensitivity: safety of cyclo-oxygenase-2 inhibitors. Treat Respir Med. 2006;5(6):399–406.17154669
- Obase Y, Shimoda T, Tomari SY, et al. Effects of pranlukast on chemical mediators in induced sputum on provocation tests in atopic and aspirin-intolerant asthmatic patients. Chest. 2002;121(1):143–150.11796443
- Dahlén SE, Malmström K, Nizankowska E, et al. Improvement of aspirin-intolerant asthma by montelukast, a leukotriene antagonist: a randomized, double-blind, placebo-controlled trial. Am J Respir Crit Care Med. 2002;165(1):9–14.11779723
- Dahlén B, Nizankowska E, Szczeklik A, et al. Benefits from adding the 5-lipoxygenase inhibitor zileuton to conventional therapy in aspirin-intolerant asthmatics. Am J Respir Crit Care Med. 1998; 157 (4 Pt 1): 1187–1194.9563738
- Ta V, White AA. Survey-defined patient experiences with aspirin-exacerbated respiratory disease. J Allergy Clin Immunol Pract. 2015;3(5):711–718.25858054
- Porcaro F, di Marco A, Cutrera R. Omalizumab in patient with aspirin exacerbated respiratory disease and chronic idiopathic urticaria. Pediatr Pulmonol. 2017;52(5):E26–E28.27685608
- Gevaert P, van Bruaene N, Cattaert T, et al. Mepolizumab, a humanized anti-IL-5 mAb, as a treatment option for severe nasal polyposis. J Allergy Clin Immunol. 2011;128(5):989–995.21958585
- Bachert C, Mannent L, Naclerio RM, et al. Effect of subcutaneous dupilumab on nasal polyp burden in patients with chronic sinusitis and nasal polyposis: a randomized clinical trial. JAMA. 2016;315(5):469–479.26836729
- El Miedany Y, Youssef S, Ahmed I, et al. Safety of etoricoxib, a specific cyclooxygenase-2 inhibitor, in asthmatic patients with aspirin-exacerbated respiratory disease. Ann Allergy Asthma Immunol. 2006;97(1):105–109.16892790
- Koschel D, Weber CN, Höffken G. Tolerability to etoricoxib in patients with aspirin-exacerbated respiratory disease. J Investig Allergol Clin Immunol. 2013;23(4):275–280.
- Prieto A, de Barrio M, Martín E, et al. Tolerability to nabumetone and meloxicam in patients with nonsteroidal anti-inflammatory drug intolerance. J Allergy Clin Immunol. 2007;119(4):960–964.17292954
- Asero R. Detection of aspirin reactivity in patients with pyrazolones-induced skin disorders. Allergy. 1998;53(2):214–215.9534925
- Kim YJ, Lim KH, Kim MY, et al. Cross-reactivity to acetaminophen and celecoxib according to the type of nonsteroidal anti-inflammatory drug hypersensitivity. Allergy Asthma Immunol Res. 2014;6(2):156–162.24587953
- Confino-Cohen R, Goldberg A. Safe full-dose one-step nabumetone challenge in patients with nonsteroidal anti-inflammatory drug hypersensitivity. Allergy Asthma Proc. 2003;24(4):281–284.12974196
- Nabe T, Hashii H, Matsubara S, et al. A tiaramide derivative, 5-chloro-3-(4-hydroxypiperadinocarbonylmethyl)benzothiazoline-2-one (HPR-611), a potent inhibitor of anaphylactic chemical mediator release–a distinctive feature from disodium cromoglycate. J Pharmacobiodyn. 1992;15(12):673–679.1284281
- Inomata N, Osuna H, Yamaguchi J, et al. Safety of selective cyclooxygenase-2 inhibitors and a basic non-steroidal anti-inflammatory drug (NSAID) in Japanese patients with NSAID-induced urticaria and/or angioedema: comparison of meloxicam, etodolac and tiaramide. J Dermatol. 2007;34(3):172–177.17291297
- Alenazy L, Alenazy L, Garcia-Neuer M, Castells M, et al. Drug hypersensitivity and desensitizations: mechanisms and new approaches. Int J Mol Sci. 2017;18(6):1316.
- Bergmann KC, Zuberbier T, Church MK. Omalizumab in the treatment of aspirin-exacerbated respiratory disease. J Allergy Clin Immunol Pract. 2015;3(3):459–460.25648572
- Ta V, White AA. Survey-defined patient experiences with aspirin-exacerbated respiratory disease. J Allergy Clin Immunol Pract. 2015;3(5):711–718.25858054
- White AA, Stevenson DD. Aspirin-exacerbated respiratory disease. N Engl J Med. 2018;379(11):1060–1070.30207919
- Grzelewska-Rzymowska I, Roznlecki J, Szmidt M. Aspirin desensitization in patients with aspirin-induced urticaria and angioedema. Allergol Immunopathol. 1988;16:305–308.