
Abstract
Purpose
Asthma is a highly prevalent noncommunicable lung disease. The aim of this study was to evaluate the longitudinal association of obesity/adiposity with wheezing and atopy.
Methods
The population of the study was composed of participants from the 1993 Pelotas (Brazil) Birth Cohort. The following outcome variables were measured at 22 years: wheezing in the last 12 months, wheezing with atopy, wheezing without atopy, only atopy, and persistent wheezing at 18 and 22 years. Exposure variables were obesity body mass index, percent fat mass (FM), and fat mass index, which were obtained by precise methods (BOD POD and dual-energy X-ray absorptiometry [DXA]). Crude and adjusted logistic and multinomial logistic regressions were used in the analyses.
Results
The prevalence of wheezing (with and without atopy), wheezing without atopy, only atopy, and persistent wheezing were 10.6%, 3.9%, 30.9%, and 4.0%, respectively. To be obese or to belong to the highest tertile of obesity/adiposity at two follow-ups showed a cumulative and positive association with wheezing in the adjusted analysis; for atopy there was no significant association. The odds ratio (OR) for wheezing according to the percentage of total FM measured by DXA in the highest tertile at both follow-ups was 1.58 (95% CI: 1.14–2.20) against an OR of 1.16 (95% CI: 0.92–1.47) for atopy. Persistent wheezing was also associated with adiposity, but without statistical significance.
Conclusions
We found a positive longitudinal association between several measures of adiposity and wheezing at 22 years old. The effect was higher for cumulative adiposity; the results for atopy were not consistent.
Keywords:
Background
Most of the literature shows a direct association between asthma or wheezing and obesity.Citation1–Citation4 Two systematic reviews among childrenCitation5,Citation6 showed that overweight and obesity are associated with an increased risk of childhood asthma. Besides the systematic reviews among children, a systematic analysis among adults showed that asthma incidence increases by 50% in overweight/obese subjects with a dose–response relationship without effect of gender.Citation7
Although there is almost a consensus about the association of asthma/wheezing and obesity, few studies have explored the atopic and nonatopic phenotypes of asthma, and the results are not so consistent as the previous ones. In a systematic review for risk factors for nonatopic asthma/wheeze in children and adolescents, obesity was found to be a risk factor.Citation8 However, the majority of the studies have used body mass index (BMI) or skinfolds as the main measure of obesity and these indicators are not the best methods for measuring fat mass (FM) or lean mass; it has been recognized that BMI does not reflect adiposity and the gold standard for adiposity is measured by dual-energy X-ray absorptiometry (DXA) or by BOD POD.Citation9,Citation10
Most longitudinal studies on this subject have been carried out outside Latin America (LA), and it is plausible to think that findings in LA can be different from developed countries because the prevalence of atopy is very high in LA.Citation11
Based on this, the aim of this paper was to measure the longitudinal association of obesity and adiposity measured by BMI, DXA, and BOD POD with three phenotypes of asthma: wheezing, atopy, and persistent wheezing, in a birth cohort from Southern Brazil, at the beginning of adulthood.
Methods
In 1993, all hospitals in the city of Pelotas were visited daily from 1 January to 31 December 1993. All mothers who had given birth at these institutions were invited to take part in the study and soon after delivery they were interviewed.Citation12 From the 5,265 live births in the city, 5,249 were enrolled in our birth cohort study. Subsamples of the cohort were followed up during childhood,Citation12 and all cohort members were sought when they had reached the mean age of 11, 15, 18, and 22 years.Citation13
The outcomes were defined according to the questionnaire of the “International Study of Asthma and Allergies in Childhood Steering Committee”, which has already been validated in BrazilCitation14,Citation15: a) presence of wheezing in the last year collected at 22 years, b) wheezing without atopy at 22 years, c) wheezing with atopy, and d) only atopy symptoms. The outcome “persistent wheezing” (presence of wheezing at 18 and at 22 years) was also analyzed and it has been shown as . Wheezing was treated as a binary variable and considered present after a positive answer to the following question: “Have you had wheezing or whistling in the chest in the past 12 months?”. Atopy symptoms were assessed based on binary questions about rhinitis and eczema: 1) “In the last 12 months, have you had any problems with sneezing, runny nose, or stuffy nose without having a flu or a cold?”; 2) “Have you ever had itchy rash, which have appeared and disappeared for at least 6 months? 3) In the last 12 months, have you had these itchy rashes on your skin?”; If the participant answered yes for any of the three questions, we considered that he had atopy symptoms in the last year.
The main exposure variables, collected at 18- and 22-year follow-ups, were BMI (kg/m2), percentage of total FM measured by the BOD POD (air displacement plethysmography – BOD POD® Composition System; COSMED, Albano Laziale, Italy),Citation16 percentage of segmented (trunk) FM measured by DXA – model Lunar Prodigy Advance®; GE Healthcare Europe GmbH, Freiburg, Germany), and fat mass index (FMI; fat kg [BOD POD]/height m2). BMI was categorized as obese (≥30 kg/m2),Citation17 and percentage of FM (according to BOD POD), percentage of total and trunk FM (according to DXA) and FMI as tertiles. Also, four variables were generated classifying individuals according to BMI, total FM, trunk FM, and FMI as follows: none – reference category – (no obese or not in the highest tertile either at 18 or at 22 years), obese or belong to the highest tertile only at 18 years, obese or belong to the highest tertile only at 22 years, and obese or belong to the highest tertile at both ages (18 and 22 years).
Categorical variables were described as absolute and relative frequencies, whereas continuous variables were described by mean and SDs. Crude and adjusted logistic regression and multinomial logistic regression were used to test associations between the outcomes and exposures.
Logistic regression was used for wheezing in the last year and for persistent wheezing, while multinomial regression was used for wheezing and atopy combined (only wheezing, wheezing without atopy, wheezing with atopy, and only atopy); the reference category was those who did not report wheezing and/or atopy. For adjustment, the following covariates were taken into account: sex (male/female), self-reported skin color (white/black/brown/other), asset index (quintiles), years of study (complete years), maternal smoking during pregnancy collected at birth (yes/no), variables that had been gathered at the 11-year follow-up (parents smoking during childhood, parents history of asthma, wheezing or bronchitis, hospitalization during the first 10 years), household crowding (number of house residents) collected at 18 years follow-up; smoking and physical activity at leisure and/or commuting at 18 and 22 years (categorized as none, present only at 18, present only at 22, and present at both follow-ups). Physical activity was measured through a standardized and previously tested questionnaire (IPAQ)Citation18 (categorized as active for ≥300 and 150 minutes a week, according to cutoff points for adolescent and adults, respectively). Confounders were chosen a priori according to previous knowledge and according to the available information on the cohort. Interaction between body composition exposures and sex was tested but it was not significant; therefore, we opted to show results adjusted to sex but nonstratified. Significance level was set as 5% and all analyses performed using Stata 13.1 software (Stata Corp LP, College Station, TX, USA).
Interviewers underwent standardization testing before beginning of field work and every 2 months afterward to determine repeatability and validity of weight, height, and skinfold measurements. All cohort follow-up projects were approved by the Federal University of Pelotas Ethics Committee. The protocols for the 18- and 22-year visits were 05/11 and 1.250.366, respectively. The cohort participants, or their caregivers, signed the term of free and informed consent prior to participation and the study was conducted in accordance with the Declaration of Helsinki.
Results
The response rate of the 1993 Birth Cohort at 11, 15, 18, and 22 years was 87.5%, 85.7%, 81.4%, and 76.3%, respectively.Citation13 The characteristics of the 3,810 members of the 1993 Pelotas Birth cohort followed up when they were 22 years old (). Most of them had white skin color and around 70% of them had nine or more years of schooling. Smoking during pregnancy was present in nearly one-third of the mothers and around 40% among fathers. Hospitalization during childhood was referred by 37% and family history of asthma, wheezing, or bronchitis by nearly 35%. The number of house residents was six or more people for 17% of the cohort participants at the 18-year follow-up. At 18 and 22 years, 44% of them were active and 9.9% were smokers. Obesity at both ages was 7.8% and the percentage in the highest tertile of all FM measures and of FMI at 18 and 22 years was similar (around 24.0%).
Table 1 Characteristics of the 22-year follow-up sample
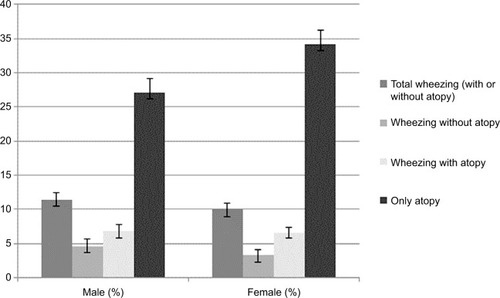
shows a prevalence of wheezing in the last 12 months of 10.6% (95% CI: 9.6–11.6), without significant difference according to sex (P=0.130) at the age of 22 years, while wheezing without atopy was more prevalent among males (4.6%; 95% CI: 3.6–5.6) than females (3.3%; 95% CI: 2.5–4.1) (P=0.04). The highest prevalence was for the outcome “atopy symptoms” reaching 30.9% (95% CI: 29.5–32.4) and more frequent among females (34.3%; 95% CI: 32.2–36.3) than males (27.1%; 95% CI: 25.1–29.2). Persistent wheezing, that is, those who have answered yes for wheezing at 18 and at 22 years old, did not differ according to sex (4.0%; 95% CI: 3.3–4.6) (data shown as ).
Figure 1 Prevalence of self-reported wheezing and atopy symptoms in the last 12 months at 22 years by sex.
Mean BMI was slightly higher at 22 than at 18 years and similar according to sex. The percentage of FM measured by BOD POD and DXA was higher at 22 compared to 18 years and higher among women than men at both follow-ups; the same pattern was observed for FMI ().
Table 2 Mean BMI and body composition variables at 18- and 22-year follow-up by sex
Obesity and most measures of adiposity were positively associated with wheezing at 22 years (). In the adjusted analysis, for those who were obese at 18 and 22 years or did belong to the highest tertile of FM and FMI also at both follow-ups, the odds ratio (OR) for “wheezing” was higher than for those who were not obese or did not belong to the highest tertile of adiposity. Also, the ORs for wheezing in the last 12 months varied from 2.0 (95% CI: 1.32–3.03), for those who were obese at both follow-ups, to 1.58 (95% CI: 1.14–2.20) for those belonging to the third tertile of percentage of total FM at both ages.
Table 3 Association between body composition at 18 and 22 years and wheezing and atopy
Very similar results were observed between obesity and measures of adiposity for the outcome “only wheezing without atopy”, with the highest ORs for those who had been obese or who belonged to the highest tertile of adiposity at 18 and at 22 years, in the adjusted analysis. Although the OR was 1.59 for wheezing without atopy according to FMI in the adjusted analysis at both follow-ups, the confidence interval included the unit (). For wheezing plus atopy (outcome shown in the third column of ), there was an association between the highest tertile of total FM measured by DXA and trunk FM (OR of 1.60; 95% CI: 1.06–2.42; OR of 1.65; 95% CI: 1.08–2.51) with P-values of 0.021 and 0.014, respectively. For the outcome “only symptoms of atopy”, in the adjusted analysis there was a positive and significant association only for the exposure “percentage trunk FM” at both follow-ups (OR=1.26; 95% CI: 1.0–1.59) (). Persistent wheezing followed the same pattern as wheezing, with higher OR for those who were obese or in the third tertile of adiposity at both ages (18 and 22 years), although probably due to the sample size the results did not reach statistical significance ()
Discussion
This paper describes a positive association between cumulative obesity/adiposity at 18 and 22 years and the phenotype wheezing at 22 years, even after adjustment for confounders; this association seems to be more due to wheezing than to atopy, because the results for the atopic phenotype (alone) were not so consistent. Persistence of wheezing at both ages also showed the same pattern as for the phenotype wheezing, although there was absence of statistical significance due to lack of power.
Most of the literature has shown an association between wheezing and obesity; however, few articles have been tried to disentangle the different phenotypes (wheezing and atopy). Classification of phenotypes is important to predict the prognosis and response to treatment and understand its underlying mechanisms.Citation19 Epidemiologic studies have considered instability of asthma phenotypes over timeCitation20,Citation21 and identified associated risk factors for each asthma phenotype.Citation19 Therefore, the aim of the present study was to evaluate the association of obesity/adiposity considering different phenotypes, such as atopic, nonatopic, and persistent.
It is plausible to think that symptoms of wheezing and atopy are a good proxy for asthma diagnosis, even without methacholine tests, because wheezing is the main symptom of asthma.Citation22,Citation23 One can argue this as a limitation of the paper, but at the young age of 18 and 22 years, asthma is the most prevalent chronic noncommunicable disease with wheezing as its main symptom; COPD is an important differential diagnosis from asthma, but COPD usually shows symptoms after the age of 40 years and not at young adulthood and its mains symptoms are cough, sputum, and dyspnea. The wheezing information may suffer from recall bias; however, we applied a well-known validated instrument to measure asthma symptoms, which eases such bias.Citation14,Citation15 Atopy in the present paper was based only on symptoms of rhinitis or symptoms of eczema, without skin prick tests or IgE measurement; this is indeed a limitation in the interpretation of the results, although it has been used in several studies.Citation24,Citation25
On the other hand, several strengths should be emphasized in this study. The prospective design allowed us to evaluate temporality and the cumulative role of the exposures for the studied outcomes. According to our results, it seems that current exposure (22 years) and cumulative exposure of obesity and adiposity (18 and 22 years) are the main risk factors for the wheezing phenotype at early adulthood, since the highest OR was observed for those subjects obese or with adiposity at two points in time (18 and 22 years) or for those with the exposure at 22 years. The very high attrition rates at all phases of this cohort reassure us of the robustness of the findings. Due to the low refusal rates and to the several follow-ups of this cohort, we were able to adjust for important potential confounders, which could be misleading the findings. Socioeconomic (SE) status is one of the most important confounders in the association between obesity/adiposity and wheezing and atopy; in this cohort it has been found that wheezing is more prevalent among poor people (12.7% in the poor tertile of income) than among rich people (9.3%), at 22 years (data not shown); and the prevalence of atopy shows the opposite pattern, prevalence of 5.6% among poor and 18.5% among rich, at the same age. Similar finding was observed in a historical cohort from Glasgow at adolescence and young adulthood age (16–30 years)Citation26; they evaluated the effect of SE position based on several indicators and wheezing and atopy and it has been found that a low SE position was associated with wheezing and a high SE position was associated with atopy. Other study with the Avon Longitudinal Study of Parents and Children (ALSPAC) cohort at childhood (7–8 years) found an association between wheezing with low SE status and atopy with high SE status.Citation27
Most studies have evaluated obesity only by BMI; however, BMI alone may not adequately characterize the relation between overweight or obesity and complex diseases such as asthma.Citation3 For instance, its usefulness and predictive value have been questioned in studies of cardiovascular disease and diabetes.Citation28,Citation29 Adiposity measured by highly precise methods (BOD POD and DXA) – as it was performed in the present cohort – enabled us to analyze the % of FM and the FMI, which are better measures of adiposity than BMI.Citation9,Citation10
A very interesting study from a developed country (England) investigated whether the magnitude of the obesity/adiposity effect varied when asthma was classified as atopic and nonatopic; the study was based on the ALSPAC cohort at the age of 7–9 years, with measures of FM obtained by DXA.Citation4 Using a Mendelian randomization approach, the authors observed a stronger effect of obesity/adiposity for nonatopic children (relative ratio [RR]: 1.90, 95% CI: 1.19–3.03) than for atopic according to BMI (RR: 1.37, 95% CI: 0.89–2.11) and according to FM an RR of 1.73 (95% CI: 1.17–2.55) and 1.25 (95% CI: 0.86–1.80), respectively.
Noal et al using data from the 1993 Birth Cohort from Pelotas found a positive association between wheezing and obesity measured by BMI and skinfolds during adolescence.Citation1 The highest RR was found for prevalence of wheezing among those who had been obese at two follow-ups (11 and 15 years) with an adjusted RR of 1.44 (95% CI: 1.01–2.07); for those ever in the highest tertile of skinfolds trajectory from 11 to 15 years the adjusted RR was 1.34 (95% CI: 0.94–1.92); they also found an association between the same exposure categories and persistent wheezing (present at 11 and 15 years). The results of the analysis at 18 and 22 years in the Pelotas cohort reveal the same pattern of results as it had been observed at the beginning of adolescence; besides that, we have shown this association classifying the sample on the nonatopic (wheezing) and atopic phenotypes, and using a more accurate measure of adiposity such as BOD POD and DXA.
Similar results to our findings were also observed in the NHANES population (2–19 years), although they have measured obesity only by BMI; among nonatopic children and adolescents the OR for wheezing was 2.20 (95% CI: 1.15–4.22) and for atopic population there was not greater risk for those obese compared to nonobese.Citation2
In a population-based study in Puerto Rican children (6–14 years), the authors found that adiposity indicators were associated with asthma, severity of asthma, and atopy, and they concluded that atopy was a mediator in this association through the mediation analysisCitation3; the main limitation of this study was the cross-sectional design and the possibility of reverse causation since temporality could not be ascertained.
Some studies have shown an association between persistence or severity of asthma (atopic and nonatopic) and obesity; Noal et al found a positive association in the same cohort as the present one, at 11 and 15 years; the outcome was “wheezing in the last 12 months” (not specifically atopic and nonatopic); an RR of 1.79 (95% CI: 1.20–2.68) and 1.82 (95% CI: 1.10–3.02) for those adolescents obese and for those in the highest tertile of skinfolds at 11 and 15 years, respectively.Citation1 In the NHANES study they found an OR of 2.14, although without statistical significance, from those who have had more medical visits due to wheezing among nonatopic than the atopic asthmatics (OR=1.10; 95% CI: 0.60–2.00).Citation3 We subclassified the persistent wheezing phenotype in those only with “persistent wheezing” (without atopy) and those with “persistent wheezing and atopy” and we did not observe differences among these two phenotypes and obesity/adiposity (data not shown).
Several plausible mechanisms have been proposed to explain the relationship between obesity/adiposity and asthma, including enhanced systemic inflammation.Citation30,Citation31 Results from the NHANES study evaluating CRP suggest that overweight may indeed lead to systemic inflammation that in turn leads to an increased risk of asthma in nonatopic individuals. There was no evidence of this relationship between systemic inflammation and asthma among atopic youth according to NHANES data. These findings suggest that allergic and systemic inflammation may operate independently on the pathway to asthma.Citation2
Another possible link would be through promotion of allergic inflammation by adipokine effects on the immune system,Citation32 but our results and also those from other studies showing stronger associations of obesity with nonatopic,Citation4 and no evidence that obesity is associated with atopy, lead us to conclude that the role of inflammation in the different phenotypes is currently unclear. We performed some analysis to see whether IL-6 and PCR were associated with atopic or nonatopic asthma in our cohort and we found a higher OR for a mean IL-6 in the third tertile at 18 and at 22 years for the phenotype wheezing and not for atopy, although most of the results were not statically significant; the OR for IL-6 and for CRP with atopy was protective (data not shown).
Given conflicting findings from studies of overweight or obesity (largely assessed by BMI) and atopy or nonatopic diseases, the role of inflammation in the different phenotypes is currently unclear.Citation2,Citation33–Citation35
As the prevalence of obesity and asthma has been increasing over the last years in LA, and to the conflicting results of the association between the different phenotypes (atopic and nonatopic asthma) and obesity/adiposity, we suggest more studies to be carried out with a prospective design and using precise methods for measuring atopy and adiposity.
Conclusion
There is a positive longitudinal association between cumulative obesity and adiposity at 18 and 22 years and wheezing at 22 years, even after adjustment for confounders; this association seems to be more due to wheezing than atopy, because the results for atopy were not so consistent.
Acknowledgments
The 1993 Birth Cohort study is currently supported by the Wellcome Trust through the programme entitled Major Awards for Latin America on Health Consequences of Population Change. The European Union, National Support Program for Centers of Excellence (PRONEX), the Brazil-ian National Research Council (CNPq), the Foundation for Research Support of the State of Rio Grande do Sul (FAPERGS), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES -Finance Code 001), and the Brazilian Ministry of Health supported phases of the study.
Supplementary material
Table S1 Association between persistent wheezing and body composition at 18 and 22 years
Disclosure
The authors report no conflicts of interest in this work.
References
- NoalRBMenezesAMMacedoSEIs obesity a risk factor for wheezing among adolescents? A prospective study in southern BrazilJ Adolesc Health2012516 SupplS38S4523283159
- VisnessCMLondonSJDanielsJLAssociation of childhood obesity with atopic and nonatopic asthma: results from the National Health and Nutrition Examination Survey 1999-2006J Asthma201047782282920707763
- FornoEAcosta-PérezEBrehmJMObesity and adiposity indicators, asthma, and atopy in Puerto Rican childrenJ Allergy Clin Immunol20141335130813141314.e1524290290
- GranellRHendersonAJEvansDMEffects of BMI, fat mass, and lean mass on asthma in childhood: a Mendelian randomization studyPLoS Med2014117e100166924983943
- NoalRBMenezesAMMacedoSEDumithSCChildhood body mass index and risk of asthma in adolescence: a systematic reviewObes Rev20111229310420406414
- MebrahtuTFFeltbowerRGGreenwoodDCParslowRCChildhood body mass index and wheezing disorders: a systematic review and meta-analysisPediatr Allergy Immunol2015261627225474092
- BeutherDASutherlandEROverweight, obesity, and incident asthma: a meta-analysis of prospective epidemiologic studiesAm J Respir Crit Care Med2007175766166617234901
- StrinaABarretoMLCooperPJRodriguesLCRisk factors for non-atopic asthma/wheeze in children and adolescents: a systematic reviewEmerg Themes Epidemiol201411524963333
- GonzalezMCCorreiaMHeymsfieldSBA requiem for BMI in the clinical settingCurr Opin Clin Nutr Metab Care201720531432128768291
- MüllerMJBraunWEnderleJBosy-WestphalABeyond BMI: conceptual issues related to overweight and obese patientsObes Facts20169319320527286962
- de Magalhães SimõesSda CunhaSSCruzÁAA community study of factors related to poorly controlled asthma among Brazilian urban childrenPLoS One201275e3705022693565
- VictoraCGBarrosFCHalpernREstudo longitudinal da população materno-infantil da região urbana do Sul do Brasil, 1993: aspectos metodológicos e resultados preliminares. [Longitudinal study of the mother and child population in an urban region of southern Brazil, 1993: methodological aspects and preliminary results]Rev Saude Publica19963013445 Portuguese9008920
- GonçalvesHWehrmeisterFCAssunçãoMCFCohort profile update: the 1993 Pelotas (Brazil) Birth Cohort follow-up at 22 yearsInt J Epidemiol201847513891390e29240909
- SoléDVannaATYamadaERizzoMCNaspitzCKInternational Study of Asthma and Allergies in Childhood (ISAAC) written questionnaire: validation of the asthma component among Brazilian childrenJ Investig Allergol Clin Immunol199886376382
- AsherMIWeilandSKThe International Study of Asthma and Allergies in Childhood (ISAAC). ISAAC Steering CommitteeClin Exp Allergy J Br Soc Allergy Clin Immunol199828Suppl 55266 ; discussion 90–91
- FieldsDAGoranMIMcCroryMABody-composition assessment via air-displacement plethysmography in adults and children: a reviewAm J Clin Nutr200275345346711864850
- de OnisMOnyangoAWBorghiESiyamANishidaCSiekmannJDevelopment of a WHO growth reference for school-aged children and adolescentsBull World Health Organ200785966066718026621
- BastosJPAraujoCLHallalPCPrevalence of insufficient physical activity and associated factors in Brazilian adolescentsJ Phys Act Health20085677779419164815
- LeeELeeSHKwonJWPersistent asthma phenotype related with late-onset, high atopy, and low socioeconomic status in school-aged Korean childrenBMC Pulm Med20171714528231776
- GreenRHPavordIStability of inflammatory phenotypes in asthmaThorax201267866566722544895
- SorknessRLZorattiEMKattanMObstruction phenotype as a predictor of asthma severity and instability in childrenJ Allergy Clin Immunol2018142410901099 e429146272
- KurukulaaratchyRJFennMMatthewsSArshadSHCharacterisation of atopic and non-atopic wheeze in 10 year old childrenThorax200459756356815223861
- CourtCSCookDGStrachanDPComparative epidemiology of atopic and non-atopic wheeze and diagnosed asthma in a national sample of English adultsThorax2002571195195712403877
- WuCCChenRFKuoHCDifferent implications of paternal and maternal atopy for perinatal IgE production and asthma developmentClin Dev Immunol2012201213214222272211
- Platts-MillsTAThe role of immunoglobulin E in allergy and asthmaAm J Respir Crit Care Med20011648 Pt 2S1S511704610
- PatelSHendersonJJeffreysMDavey SmithGGalobardesBAssociations between socioeconomic position and asthma: findings from a historical cohortEur J Epidemiol201227862363122696048
- GalobardesBGranellRSterneJChildhood wheezing, asthma, allergy, atopy, and lung function: different socioeconomic patterns for different phenotypesAm J Epidemiol2015182976377426443417
- KodamaSHorikawaCFujiharaKComparisons of the strength of associations with future type 2 diabetes risk among anthropometric obesity indicators, including waist-to-height ratio: a meta-analysisAm J Epidemiol20121761195996923144362
- ChrysantSGChrysantGSNew insights into the true nature of the obesity paradox and the lower cardiovascular riskJ Am Soc Hypertens201371859423321407
- FordESGaluskaDAGillespieCWillJCGilesWHDietzWHC-reactive protein and body mass index in children: findings from the Third National Health and Nutrition Examination Survey, 1988-1994J Pediatr2001138448649211295710
- RetnakaranRHanleyAJConnellyPWHarrisSBZinmanBElevated C-reactive protein in Native Canadian children: an ominous early complication of childhood obesityDiabetes Obes Metab20068548349116918582
- FengerRVGonzalez-QuintelaAVidalCExploring the obesity-asthma link: do all types of adiposity increase the risk of asthma?Clin Exp Allergy20124281237124522805471
- CibellaFCuttittaGLa GruttaSMelisMRBucchieriSViegiGA cross-sectional study assessing the relationship between BMI, asthma, atopy, and eNO among schoolchildrenAnn Allergy Asthma Immunol2011107433033621962093
- HancoxRJMilneBJPoultonRSex differences in the relation between body mass index and asthma and atopy in a birth cohortAm J Respir Crit Care Med2005171544044515557135
- van GyselDGovaereEVerhammeKDoliEde BaetsFBody mass index in Belgian schoolchildren and its relationship with sensitization and allergic symptomsPediatr Allergy Immunol200920324625318798801