
Abstract
This review by pediatric gastroenterology and allergy-immunology experts aimed to address the biological roles of human milk oligosaccharides (HMOs) and the potential utility of HMOs in prevention of allergy with particular emphasis on cow’s milk protein allergy (CMPA). The participating experts consider HMOs amongst the most critical bioactive components of human milk, which act as antimicrobials and antivirals by preventing pathogen adhesion to epithelial cells, as intestinal epithelial cell modulators by enhancing maturation of intestinal mucosa and intestinal epithelial barrier function, as prebiotics by promoting healthy microbiota composition and as immunomodulators by modulating immune cells indirectly and directly. Accordingly, the participating experts consider the proposed link between HMOs and prevention of allergy to be primarily based on the impact of HMO on gut microbiota, intestinal mucosal barrier, immunomodulation and immune maturation. Along with the lower risk of respiratory and gastrointestinal infections, HMO-supplemented formulas seem to be promising alternatives in the management of CMPA. Nonetheless, the effects of individual as well as complex mixtures of HMO in terms of clear clinical and immunological effects and tolerance development need to be further explored to fully realize the immunomodulatory mechanisms and the potential for HMOs in prevention of allergic diseases and CMPA.
Introduction
The nutritional composition and the non-nutritive bioactive content of human milk are unique for survival and healthy development of the human infant.Citation1 Accordingly, infant feeding is recommended to include exclusive breastfeeding during the first six months of life along with continued breastfeeding for 1 to 2 years of life with complementary feeding.Citation1
Although infant formula milk is an alternative for infant nutrition when human milk is not available, the formula-fed versus exclusively breastfed infants are considered to be more vulnerable to infectious and immune diseases.Citation2
Human milk oligosaccharides (HMOs) are the third-most abundant solid component in maternal milk following the lipids and lactose.Citation3–Citation5 HMOs are associated with certain physiological functions and clinical benefits such as the modulation of microbiota composition, modulation of gut epithelial cell responses and immunomodulatory and anti-inflammatory effects.Citation3–Citation5 In this regard, HMOs have become the focus of current scientific research, given that they offer further optimization of infant nutrition by reducing the compositional difference between human milk and infant formula, as a key support to immune development in early life.Citation6–Citation10
Nonetheless, while the technological advances enabled the addition of up to 5 oligosaccharides structurally identical to HMOs in infant formula, the oligosaccharides composition from infant formula remains very different from human milk, both in diversity and concentration.Citation7,Citation11
There is an emerging evidence in humans in favor of the role of infant gut microbiome in food sensitization/allergy.Citation12,Citation13 Given the benefits of HMOs in terms of early intestinal microbiome development and gastrointestinal and systemic immune modulatory functions,Citation5,Citation6,Citation14–Citation16 supplementation of infant formula with HMOs has been considered a promising strategy in non-exclusively breastfed infants including those with cow’s milk protein allergy (CMPA).Citation9,Citation17
Although based on scarce amount of literature data in infants, HMO-supplemented infant formula was reported to be a safe and tolerable supplementation with several positive effects.Citation7,Citation9,Citation17 Amongst these are the increased amount of bifidobacteria and short chain fatty acids (SCFAs) production, likelihood of reduction in respiratory tract infections and provision of an accepted hypoallergenicity criteria, when added to existing extensively hydrolyzed (eHF) or amino acid-based (AAF) formula in CMPA.Citation7,Citation9,Citation17
Therefore, this review by a panel of pediatric gastroenterology and allergy-immunology experts aimed to address the biological roles of HMOs in terms of early gut microbiota development and gastrointestinal and systemic immunomodulatory properties and the potential utility of HMOs in prevention of allergy with particular emphasis on infants and children with CMPA.
Methods
The present expert panel consisting of pediatric gastroenterology and pediatric allergy-immunology specialists who are members of the Turkish Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the Turkish National Society of Allergy and Clinical Immunology Society met to develop consensus opinion on the biological roles and potential utility of HMOs in infants and children with CMPA. The participating experts (professors, also international speakers and national influencers), who had at least 15 years of experience in pediatric gastroenterology and pediatric allergy-immunology were invited after being recommended by the presidents of the Turkish Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the Turkish National Society of Allergy and Clinical Immunology Society. The panel performed a broad non-structured literature search to reveal the potential studies and agreed on the studies to be included in the review. The panel critically analyzed the evidence-based published literature regarding biological roles and efficacy of HMOs in breastfed infants according to HMO composition as well as the clinical trials with use of HMO-supplemented infant formula in prevention of allergy and CMPA in particular. Based on the available scientific evidence and the experts’ clinical opinion, this consensus document comprehensively addresses HMOs in terms of a) overview of human milk bioactive components, b) structure and biological roles of HMOs, c) advantages of HMO-supplemented infant formula, and d) rationale and potential benefits of using HMO-supplemented infant formula in prevention of allergy with special emphasis on infants and children with CMPA.
HMOs: one of the most important bioactive components of human milk
The functional or bioactive components of human milk, the elements affecting the biological processes or substrates and ultimately the health, have increasingly been recognized as factors responsible for the short- and long-term benefits of human milk feeding.Citation18,Citation19 These functional components involve a large group of several compounds such as protein (lactoferrin), carbohydrates (especially HMOs), fats (polyunsaturated fatty acids), immunoglobulins, hormones, vitamins, nucleotides, minerals, prebiotics, probiotics, transporters, antioxidants and antimicrobial factors.Citation18
T-helper (Th) cell population is still biased towards the Th2 phenotype (humoral immunity) rather than Th1/Th17 phenotype (cellular immunity) at birth.Citation20–Citation22 Human milk provides protection during this vulnerable period via bioactive components that stimulate healthy intestinal microbial diversity (Bifidobacteria and Lactobacillus species), prevent pathogenic infection, promote intestinal development and mucosal barrier function, facilitate immune tolerance and directly support the further development of the immune system ().Citation5,Citation8,Citation10,Citation15,Citation23–Citation25
Figure 1 Human milk bioactive components in relation to provision of healthy neonatal microbial colonization, fine-tuning of inflammatory processes and immune defense and maturation in early life.
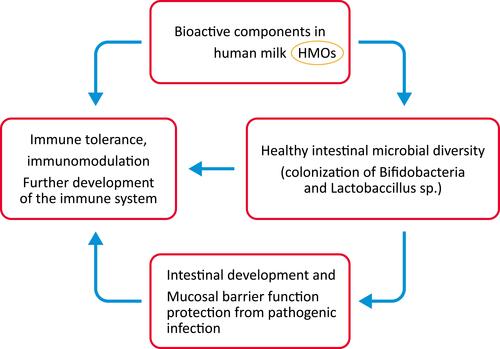
The physical barriers and the crosstalk between mucosal epithelial cells and underlying immune cells are considered to play a crucial role in the first-line defense in early life.Citation8,Citation22,Citation26,Citation27 Hence, the gastrointestinal tract, as a functional barrier preventing pathogenic invasion and an immune-modulator providing active elements of the lymphoid cell line, is considered to be of utmost importance to the neonatal immunity.Citation21,Citation22
The breastfeeding as a nutrient source in early life and particularly the non-digestible HMOs amongst the diverse bioactive components in human milk are considered critical for healthy neonatal microbial colonization, fine-tuning of inflammatory processes and immune defense and maturation in the first years of life ().Citation8,Citation10,Citation22
The incidence as well as severity of several infectious diseases (ie, bacteremia, diarrhea, otitis media, respiratory and urinary tract infections, necrotizing enterocolitis) and immune system disorders (ie, inflammatory bowel disease [IBD], allergy, asthma, type 1 diabetes) is considered to be lower in breastfed infants vs formula-fed infants.Citation2,Citation7,Citation10,Citation18,Citation28–Citation30
Human milk, during the time of complementary food introduction, is considered likely to prevent celiac disease or allergy through interactions between dietary antigens, human milk components and gut associated lymphoid tissue (GALT).Citation31–Citation34
Structure and biological roles of HMOs
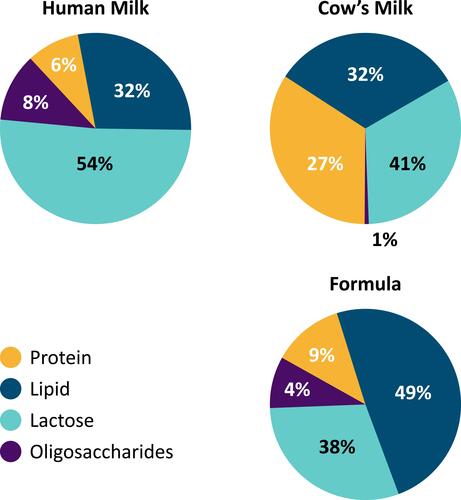
Human milk is a complex matrix and a living tissue consisting of 87% water, 3.8% lipid, 1.0% protein and 7% lactose, while HMOs (1–1.5%) represent the third largest component of human milk, after lactose and lipids.Citation5,Citation7,Citation11,Citation35,Citation36
HMOs are a unique mixture of structurally diverse indigestible carbohydrates present in the human milk.Citation7,Citation10,Citation19,Citation37 The concentration and composition of HMOs is subjected to inter-individual variation, depending on the genetic predisposition and geographical origin of mothers as well as on the gestational age at delivery (higher concentrations but lower levels of fucosylated HMOs in preterm vs term milk), stage of lactation (colostrum: 20–25 g/L; mature milk: 5–20 g/L) and maternal nutrition.Citation7,Citation8,Citation10,Citation11,Citation22,Citation38,Citation39
The changes in HMOs from secretor mothers during the course of lactation was reported to include a decrease in total, fucosylated, sialylated, non-fucosylated neutral HMO concentrations over time, an increase in the percentage of fucosylation and a decrease in the percentage of sialylation, while non-fucosylated neutrals are considered to remain stable over time.Citation40 Hence, HMOs do not decrease in concentration uniformly across lactation, with change in individual HMO concentrations during lactation and predominance of different HMOs in each stage.Citation40,Citation41
2′-fucosyllactose (2ʹ-FL) is the most abundant HMO, accounting for about 20–40% of total HMO concentration in colostrum, whereas 6ʹ-sialyllactose (6ʹ-SL) is the dominant form of sialylated HMO at the early stages of lactation, followed by 3ʹ-sialyllactose (3ʹ-SL) in late lactation.Citation40 HMOs are considered to be stable over one-week during early lactation, while most HMOs decline as lactation progresses, except for 3ʹ-FL and 3’-SL which are consistently higher at 6 months and 12 months of lactation.Citation40–Citation43
Indeed, the efforts to enhance the quality of infant formulas aim not only to mimic the composition of human milk in every respect (ie, adapting the composition of bioactive compounds besides the concentration of macronutrients and micronutrients) to make it as similar as possible to human milk but also to achieve physiological effects as in breastfed infants.Citation18 Hence, whether the HMO supplementation ultimately improves infant formula milk in a way that mimics the documented benefits of human milk remain to be further investigated.Citation42,Citation44
Structure of HMOs
Of at least 200 unique HMOs identified in human milk, more than 100 were structurally defined.Citation38,Citation45,Citation46 HMOs consist of monosaccharides and monosaccharide derivatives with a lactose, polylactosamine or lacto-N-biose core, while a further modification through differently linked fucose or sialic acids to the molecule enables structural diversity and resistance against enzymatic digestion.Citation22
The basic HMO structure is fucosylated or nonfucosylated and/or sialylated, resulting in neutral, neutral N-containing and acidic HMO subtypes ().Citation5,Citation7,Citation47,Citation48
Figure 2 Human milk oligosaccharide structural subtypes.
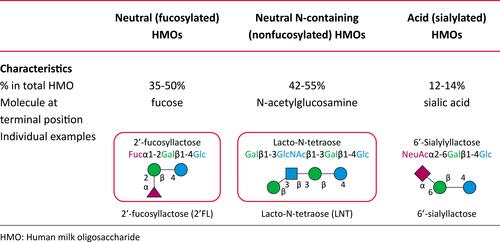
The neutral HMOs comprise > 75% of the total HMOs in the human milk, while the most abundant HMO is the 2′-FL (2.7 g/L, range, 1.88–4.9 g/L).Citation7,Citation39 2′-FL, a glucose, galactose, and fucose based trisaccharide, constitutes almost 30% of the total HMOs in secretor mothers ().Citation7,Citation39
HMO profile of human milk is dependent largely on the individual maternal genetic disposition.Citation8 Hence, the complex HMO composition is genetically determined by the activity of the secretor (Se) fucosyltransferase 2 gene encoding α1-2-fucosyltransferase (FUT2) and the Lewis (Le) gene encoding α1-3/4-fucosyltransferase (FUT3), and is regulated by glycosyl-transferases within the mammary gland.Citation5,Citation31,Citation34,Citation49
Based on Se locus, women are categorized into secretors (those with functional FUT2 enzyme and with 2′-FL, LNFP I and other α1-2-fucosylated HMOs in milk) and non-secretors (those lack a functional FUT2 enzyme and with no α1-2-fucosylated HMOs in milk).Citation7,Citation47,Citation50,Citation51
Based on Le locus, women are categorized into Le-positive women (express FUT3, milk contain specific α1-4-fucosylated HMOs such as LNFP II) and Le-negative women (lacks FUT3 activity and specific α1-4-fucosylated HMOs in milk).Citation7,Citation47,Citation50,Citation51
Hence, based on the expression of FUT2 and FUT3, the human milk is classified as: Le-positive secretors (Le+Se+), Le-negative secretors (Le-Se+), Le-positive nonsecretors (Le+Se-), and Le-negative nonsecretors (Le-Se–) ().Citation7,Citation47,Citation50,Citation51
Figure 3 Human milk oligosaccharide profile according to genetic background.
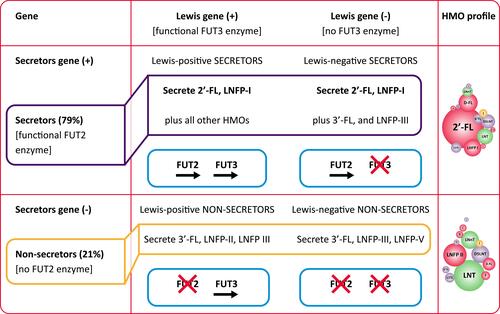
Overall, 79% of mothers in European and North American populations have the active gene for FUT2 (secretors), while 21% of mothers lack the functional FUT2 enzyme (non-secretors) and produce milk without 2′FL and LNFP I.Citation7,Citation37–Citation39,Citation47 Notably, the delayed bifidobacteria colonization and altered microbiota-related metabolic activity and increased risk for diarrheal diseases have been reported in infants fed by non-secretor mothers.Citation10,Citation13,Citation52,Citation53 Nonetheless, it should be noted that HMOs differ in terms of individual structures and related effects, emphasizing the importance of balanced complex mixture.Citation31
Biological roles of HMOs
HMOs have several functions, including selectively enriching gut bacteria and thereby promoting healthy microbiota composition, preventing pathogen adhesion to epithelial cells, enhancing maturation of intestinal mucosa and intestinal epithelial barrier function, modulating immune cells, pathogen recognition receptors as well as signaling pathways related to maturation of lymphoid tissue, influencing cytokine and chemokine networks that regulate Th1/Th2 lymphocyte balance and preventing infection and supporting immunity ().Citation6,Citation8,Citation10,Citation15,Citation22
Figure 4 Biological roles of human milk oligosaccharide (HMOs).
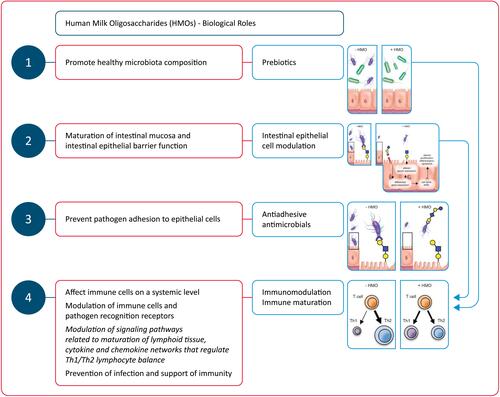
Immunomodulation is one of the most outstanding functions of HMOs, including the indirect modulation of immune responses via changes in infant gut microbiota composition, and the direct effect on immune cells at a systemic level, after reaching the blood circulation ().Citation22,Citation46,Citation47,Citation54,Citation55
Following gastrointestinal absorption, up to 1% of HMOS become available in systemic circulation at a level (ranging 10 to 100 mg/mL) being sufficient for interaction with cell receptors.Citation46,Citation47,Citation54
Therefore, HMOs are considered to have multiple beneficial effects in a breast-fed infant:Citation11
As prebiotics they are metabolic substrates for beneficial bacteria enabling a growth advantage for them over potential pathogens;
As antiadhesive antimicrobials they act as soluble glycan receptor decoys preventing the pathogen-intestinal mucosa contact;
By directly affecting intestinal epithelial cells and modulate their gene expression, resulting in modifications in the cell surface glycans and other cellular responses;
By modulating lymphocyte cytokine production, increasing the likelihood of a a more balanced Th1/Th2 response;
By reducing selectin-mediated interactions between immune cells and decreasing the leukocyte rolling on activated endothelial cells, decreasing the likelihood of mucosal leukocyte infiltration and activation.
HMOs as antimicrobials and antivirals
HMOs mimic the glycans on the gut epithelia that acts as surface pathogen receptors (virus, bacteria, toxins and/or eukaryotes) and they prevent gut epithelial adhesion and biofilm formation through competitive interaction with pathogens.Citation8,Citation31,Citation47,Citation56 In addition to acting as soluble decoy receptors and blocking the attachment of viral pathogens to the epithelial cells, HMOs can also indirectly prevent viral adhesion through binding to the epithelial surface causing a structural change in the receptor.Citation57 Accordingly, antimicrobial and antiviral effects of HMOs depend on blockade of pathogen access via pathogen or epithelial surface receptor binding to prevent their replication and subsequent infection.Citation8 In addition, they are more advantageous than pathogens in terms of being fermented by commensal bacteria (ie, Bifidobacteria) which promote their growth while pathogens experience growth suppression.Citation8,Citation31
Notably, in addition to serving as prebiotics, HMOs possess bacteriostatic and antimicrobial properties against Streptococcus agalactiae and Gram-negative aerobe Acinetobacter baumannii as well as antibiofilm properties against methicillin-resistant Staphylococcus aureus (MRSA).Citation57,Citation58 HMOs were reported to inhibit Campylobacter colonization and to reveal protection against pneumococcal pneumonia in animal studies.Citation59,Citation60 The studies in infants revealed that they offer protection against infectious diarrhea, necrotizing enterocolitis, and can directly inhibit the growth of group B streptococcus (GBS), a leading cause of invasive bacterial infection in newborns.Citation61–Citation64 Moreover, HMOs are suggested to potentiate the actions of aminoglycosides, anti-folates, macrolides, lincosamides, and tetracyclines against GBS, S. aureus and A. baumannii.Citation57,Citation65 Hence, prophylactic and therapeutic use of HMOs is also possible in immune compromised infants as well as in those at high risk of infection.Citation10
HMOs as intestinal epithelial cell modulators
HMOs, through interaction with glycans on the epithelial or dendritic cell surface, promote gut maturation and contribute to the barrier integrity via increased growth of Bifidobacterium.Citation8,Citation66 HMOs can also directly affect the intestinal cell response by suppressing the cell growth and by stimulating the differentiation and apoptosis, required for a proper intestinal barrier function.Citation7,Citation67
In fact, besides their impact on microbes and their roles as decoy receptor for pathogens, HMOs can also directly alter epithelial cell gene expression and thus alter the binding ability of certain pathogens to the cell surfaces via changing the expression of cell surface glycocalyx.Citation3,Citation6,Citation68 In addition, HMOs induce production of SCFAs important for gut health such as butyric acid and propionate which can stimulate mucin release, mucosal blood flow and intestinal epithelial cell maturation through their interaction with the host epithelium.Citation8,Citation69–Citation71 These functions are considerably important in early neonatal life given that intestinal health and barrier function are the first line of defense in innate immunity.Citation72
HMOs as prebiotics and effectors of the microbiota composition
Since infants lack glycoside hydrolases and intestinal membrane transporters, the majority of HMOs reach the colon undigested and are utilized by certain microbes influencing the gut microbiota.Citation6,Citation73 Hence, HMOs are “prebiotics” that selectively induce the growth of beneficial (probiotic) organisms such as Bifidobacterium, a dominant species in the intestine of breast-fed infants.Citation6,Citation19,Citation73 Bifidobacteria have the ability to utilize HMOs through specifically expressed glycoside hydrolases and therefore considered to be co-evolved with HMOs.Citation6
Accordingly, for breast-fed infants, bifidobacteria can preferentially colonize the infant GI tract by the third month of life.Citation74 HMOs also play a role in improved epithelial barrier function by inducing the B. infantis growth in the infant gut, which is responsible for production of peptides that normalize intestinal permeability.Citation10,Citation74,Citation75 Indeed, a highly selective, prebiotic effect of HMOs has been reported in shaping the gut microbiota in the first weeks of life with a decrease in fecal HMOs via a shift in fecal bacterial population from the non-HMO-consuming microbes (Enterobacteriaceae and Staphylococcaceae) to HMO-consuming bacteria (Bacteroidaceae and Bifidobacteriaceae).Citation74
In this regard, HMOs are considered to play a key role in healthy development of gut-microbiota, and thus the intestinal wall barrier and immune functions.Citation6,Citation76 Given the impact of maternal secretor status on the infant gut bifidobacterial community, the combination of HMOs with specific bacteria has been suggested likely to modulate gut immunity and gut integrity.Citation31,Citation52
HMOs as immunomodulators and potential inducers of immune maturation
The gut barrier involves a mucus layer, epithelium, the resident microbiota, and resident or recruited immune cells, whereas the immune responses are immature in newborns as based primarily on a Th2 type response rather than a Th1 type immune response along with a relative lack of immunological memory.Citation6,Citation77
HMOs are considered to affect expression of several cytokines including IL-8, IL-1β, colony-stimulating factor 2 (CSF2), platelet factor 4 (PF4) and IL-17C. They also influence the expression of certain chemokines including CXCL1,2,3,6, CX3CL1, CCL5 and CCL20 as well as that of cell surface receptors including intercellular adhesion molecule-1 (ICAM-1), intercellular adhesion molecule-2 (ICAM-2), interferon γ receptor 1 (IFNGR1), and IL-10 receptor a (IL10RA).Citation5 In this way, HMOs can modulate the intrinsic expression of cell trafficking-related inflammatory markers, the lymphoid tissue-related signaling pathways and the cytokine and chemokine networks responsible for Th1/Th2 lymphocyte balance ().Citation8,Citation10,Citation15,Citation78
HMOs are considered to target expression of receptors involved in pathogen recognition, such as toll-like receptors (TLRs), to interact with dendritic cells (DCs) in close proximity to the intestinal epithelial barrier that leads to T cell differentiation and/or T cell/B cell interaction and to show systemic effects by interaction of neutrophils, lymphocytes and monocytes with endothelial cells that affects immune cell populations and secretion of cytokines.Citation8,Citation10,Citation78
In fact, DCs are considered to play a cardinal role in the regulation and development of innate and adaptive immune responses during infections and inflammatory diseases and one sub-population, so-called tolerogenic DC (tDC), results in a reduced inflammatory cytokine production (ie, IL-4, IL-12, IL-6, and TNF-α) but an elevated regulatory cytokine production (ie, TGF-β IL-10 and IL-27).Citation78
Overall, interactions with these chemokines, cytokines, and cell surface receptors are considered to enable subsequent immunomodulation and immune maturation through development of a balanced and efficient immune response and thus a lesser risk of infections and allergic diseases.Citation5,Citation8,Citation10,Citation78
Accordingly, HMOs play a role in the maturation of the infant immune system both at the gut barrier level through effects on microbiota, gene expression and intestinal epithelial cell maturation as well as by exerting direct immune modulating effects after being absorbed intact into the systemic circulation.Citation10,Citation22,Citation46,Citation79 Notably, nearly 70% of gastrointestinal immune cells may associate directly with HMOs consumed by infants, while the first few weeks of life represent a key window of immune development with a circulatory peak of innate immune cells during this period.Citation80
HMO-supplemented infant formula
Milk oligosaccharides in human milk present at a higher concentration and a greater structural diversity and degree of fucosylation than those in cow’s milk and infant formulae.Citation10 HMOs are unique for human milk and not found in the same composition and diversity in animal milk ().Citation11,Citation81
Figure 5 Composition of human milk, formula (Similac® infant formula, Abbott nutrition) and cow’s milk. Data from Bode L.Citation11
Despite the well-known benefits of HMOs, it has only recently become technically feasible to produce HMOs identical to human milk HMOs.Citation9 Accordingly, cow-milk derived infant formulas have been supplemented with affordable non-digestible carbohydrates (non-HMOs) such as fructo-oligosaccharides (FOS) and galacto-oligosaccharides (GOS) to enable some of the HMO functions.Citation82
The recent availability of synthesized 2′-FL, structurally identical to the 2′-FL in human milk, is important in this regard, enabling the availability of HMOs in some commercial infant formulas.Citation66 Currently, two types of HMOs are used as add-on to the infant formula including a fucosylated HMO, 2′FL, and a neutral, non-fucosylated HMO, LNnT.Citation9,Citation47,Citation83 HMO-supplemented infant formulae are considered to be safe and beneficial for human infants along with increased availability of commercially produced HMOs.Citation17,Citation79,Citation84
2′-FL is the most abundant HMO in the milk of most lactating women with extensive data on the potential systemic effects.Citation80 Preclinical data indicate 2′-FL to have multiple functions via prebiotic, anti-infective, anti-inflammatory and immunomodulatory properties and to reduce the risk of necrotizing enterocolitis.Citation80 Observational studies revealed the association of 2′-FL HMOs with bifidobacteria dominated early gut microbiota in breastfed infants.Citation52,Citation85,Citation86
Albeit the amount of data available on HMO supplementation in infant formula from clinical trials in infants is still limited,Citation4 clinical data showed the supplementation of infant formula with 2′-FL to be safe and well-tolerated.Citation17,Citation79,Citation84,Citation87,Citation88 Moreover, 2′-FL is considered to show similar absorption and excretion characteristics with 2′-FL in human milkCitation84 and is associated with similar immune benefits with the breastfed reference group, and fewer respiratory infections.Citation79
In a past study with 420 healthy term infants by Marriage et al,Citation84 authors reported no significant differences between groups of infant formulas added with GOS/L (2.4 g), 2′-FL (0.2 g) + GOS/L (2.2 g) or 1 g 2′-FL (1 g) + GOS/L (1.4 g) and the breast-fed reference group in terms of data on weight, length, and head circumference. All formulas were well tolerated along with similar 2′-FL relative absorption and excretion between infants fed with 2′-FL containing formulas and the breast-fed infants.Citation84
Further analysis of 201 healthy term infants from the cohort from Marriage et al,Citation84 by Goehring et al,Citation79 revealed the circulating cytokines concentrations in infants fed with the 2′-FL containing formulas to differ from the concentrations in infants fed with GOS containing formulas but not from the concentrations in breast-fed infants.Citation79
In a study by Puccio et alCitation17 in healthy infants randomized to a cow’s milk-based infant formula (control, n = 87) or the same formula with 1.0 g/L 2ʹfucosyllactose (2ʹFL) and 0.5 g/L lacto-N-neotetraose (LNnT) (test, n = 88), the authors reported that weight gain through 4 months, digestive symptoms and behavioral patterns were similar in both groups, except for softer stool and fewer nighttime wake-ups in the test group at 2 months. Infants receiving test (vs control) had significantly fewer parental reports of bronchitis through 4 (2.3% vs 12.6%), 6 (6.8% vs 21.8%), and 12 months (10.2% vs 27.6%), lower respiratory tract infection (adverse event cluster) through 12 months (19.3% vs 34.5%), lower rate of antipyretics use through 4 months (15.9% vs 29.9%) and antibiotics use through 6 (34.1% vs 49.4%) and 12 months (42.0% vs 60.9%).Citation17
In a real-world study by Roman et alCitation87 on growth and tolerance in three groups of infants (n=159) including a healthy, exclusively breastfed infants, an exclusively formula-fed group who received a milk-based formula with 2ʹ FL (1g/L) and LNnT (0.5g/L), and a group mixed fed with both formula and human milk for 8 weeks, the authors reported that mean z-scores for growth and gastrointestinal tolerance were similar between all groups and incidence of AEs was low overall, and comparable across groups.Citation87 Hence, the authors concluded that the growth and tolerance outcomes of a HMO-supplemented infant formula were similar to data from randomized clinical trials, supporting the effectiveness of this early feeding option.Citation87
In a prospective, randomized, multi-center, double-blinded, controlled tolerance study by Kajzer et alCitation88 in 131 healthy term infants assigned to control formula without oligosaccharides (n=30), formula with 0.2 g 2‘-FL/L + 2 g scFOS/L (n=35) and breast-fed reference group (n=36), the authors noted that 2′-FL and scFOS containing formula was safe and well tolerated with no significant differences among the three groups at 35 days of age in terms of stool consistency, formula intake, anthropometric measures, and percent feedings with spit-up/vomit associated with feeding.Citation88
Overall, 2′-FL supplementation of infant formula has been considered to be safe and tolerable approach along with absorption and excretion efficiency similar to 2′-FL in human milk.Citation80 The 2′-FL supplementation has also been considered to offer additional advantages such as immune benefits, improved tolerance and lower risk of respiratory infections.Citation80 Addition of 0.2 g 2′-FL/L to the infant formula supports immune and gut health and brings it closer to human milk not only compositionally but also functionally.Citation80
Utility of HMO-supplemented infant formula in prevention of allergy
Rationale behind the proposed link between HMOs and prevention of allergy
Exclusive breastfeeding has a potential to reduce the development of several diseases such as asthma, allergies, IBD, and type 1 diabetes,Citation15 while the “secretor type” related complex mixtures of HMOs are also considered likely to have a critical role in lowering the risk of allergic disease experienced by breast-fed infants later in life.Citation31,Citation89
HMOs are suggested to improve gut epithelial integrity, apoptosis, and intestinal permeability and to have indirect and direct immunomodulatory properties.Citation6,Citation15 The immune modulating properties of HMOs, including interaction with dendritic cells and reduced antigen–antibody complex-induced chemokine release, are considered of critical importance for CMPA in terms of attenuation of allergic symptoms as well as promotion of tolerance development.Citation9,Citation78,Citation90,Citation91
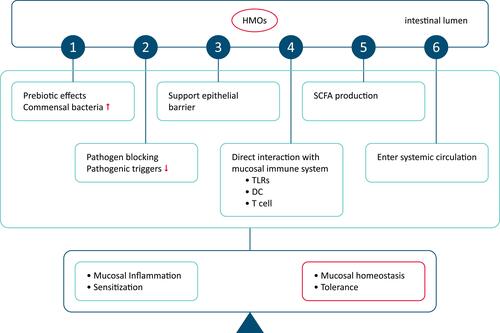
The proposed link between HMOs, tolerance induction and prevention of allergy is primarily based on the certain effects of HMOs on gut microbiota, intestinal mucosal barrier and immunomodulation.Citation8,Citation92 These include the prebiotic effects, effects related to pathogen binding, enhanced epithelial barrier integrity and local and systemic modification of immune responses via SCFAs produced during HMOs fermentation, stimulation of mucus production and epithelial tight junction integrity to support the physical barrier between the intestinal epithelium and the gut content, the direct interaction with mucosal immune system (ie, modulation of the response of DCs, protective mucosal immune development) and finally the immunomodulatory role beyond the gastrointestinal tract via entering systemic circulation through transportation over the intestinal epithelium ().Citation92
Figure 6 Potential roles of human milk oligosaccharide in enhanced tolerance induction and prevention of allergic diseases.
Gut microbiota, barrier integrity and prevention of allergy
The composition and function of gut microbiota early in life is considered important in the development of food allergy.Citation93,Citation94 Reduced gut microbial diversity and dysbiosis during early life is considered a risk factor for immune-mediated diseases, such as allergy and asthma, through modulation of balance between effector or tolerant responses (activities of Th1 and Th2 cells) that leads to induction of a Th2-skewed immune response, with enhanced IgE responses to food antigens, and/or a defect in mounting proper regulatory T-cell responses.Citation95
Hence, the manipulation of the microbiota of the infant during pregnancy or after birth, when there is significant immune-plasticity has been suggested to have an impact on allergy prevention.Citation95 HMO-dependent increase in the growth of Bifidobacterium induces healthy gut microbiota development and contributes to the barrier integrity, while the direct effects of HMOs on the intestinal cell response (ie, reducing the cell growth, inducing differentiation and apoptosis, stimulating SCFA production) are also important for intestinal epithelial cell maturation and a proper intestinal barrier function.Citation7,Citation8,Citation66,Citation67,Citation69–Citation71
Notably, the infants who are exclusively breastfed by secretor mothers vs those breastfed by non-secretor mothers were reported to have a more rapid establishment of a bifidobacteria-predominant microbiota as well as lesser likelihood of diarrhea development.Citation7,Citation61 The stool bacterial profile in infants fed by a formula supplemented with 2′-FL and LNnT was reported to be more similar to that of the breastfed infants rather than those fed by a formula not supplemented with prebiotics.Citation7,Citation17 The amount of 2-FL in human milk was reported to inversely correlate with the incidence of Campylobacter diarrhea and the severity of infection with E. coli in infants,Citation53,Citation96 while besides their effects on gut bacteria, HMOs have also been reported to affect viral pathogens (ie, norovirus, rotavirus and HIV).Citation97
HMOs are suggested to decrease the risk of preterm mortality and morbidity via their modulatory effects on the gut microbiome to protect against infections (ie, necrotizing enterocolitis, candidiasis) and several immune-related diseases,Citation6,Citation7,Citation98 while recent studies have also suggested a possible association between HMOs and atopic dermatitis, milk allergy or allergic sensitization in the infant.Citation13,Citation89,Citation99,Citation100
Although the exact mechanism behind the association of microbiota composition with allergy development remains unknown, a protective role for SCFA has been suggested in asthma, arthritis, and colitis models as well as in allergic airway inflammation.Citation93
Immunomodulation, immune maturation and allergy prevention
Although many studies regarding the composition of HMOs have been published, there are few publications on the immune-modulatory effects of individual HMOs.Citation5,Citation84,Citation101 Although anti-inflammatory and immune regulatory potential of HMOs has been suggested, the exact mechanism underlying the effect of the specific HMOs on the risk for allergy development remains unknown.Citation5,Citation84,Citation101 Nonetheless, proposed mechanisms underlying immunomodulatory properties of HMOs include the pathogen decoy capacity, the prebiotic effect, the modulatory effect on the SCFA production and thus improved barrier integrity and the direct immune modulatory functions.Citation31
The use of HMOs has been considered to reduce the levels of cytokine proteins including monocyte chemoattractant protein 1/2, IL-8, IL-6 and IL-1β, whereas to increase the level of cytokines associated with tissue repair and homeostasis.Citation15 The HMO-mediated induction of tDCs with ability to modulate T‐cell responses is considered likely to be a potential target for prevention and treatment of autoimmune diabetes and allergic diseases early in life.Citation78,Citation102
Accordingly, superiority of HMOs over non-human prebiotic oligosaccharides was indicated in systemic and gastrointestinal immunomodulation.Citation7,Citation103 The plasma concentration of inflammatory cytokines was reported to be significantly lower in the breastfed infants and infants fed with 2′-FL-supplemented formula when compared to those fed with GOS-supplemented formula.Citation79
The impact of 2′-FL on reduction of food allergy related symptoms was suggested to occur via induction of interleukin-10+ T-regulatory cells and indirect stabilization of mast cells in a mouse model.Citation91 Moreover, cord blood T-cells exposed to sialylated HMOs were reported to increase the number of interferon-γ-producing CD3+CD4+ and CD3+CD8+ lymphocytes and interleukin-13 (IL-13)-producing CD3+CD8+ lymphocytes.Citation104 Sialylated HMOs were also reported to reduce IL-4 production in a subset of lymphocytes from adult patients with peanut allergy, indicating that certain sialylated HMOs may contribute to allergy prevention.Citation55 Acidic HMOs were also reported to induce IFN-gamma and IL-10 in human cord blood T cells, and to decrease IL-4 production in allergen-specific T cells.Citation55 Supplementation of 2′-FL alone was reported to lower levels of TNFa, IL-1a, IL-1b, and IL-6, resembling those identified in breast fed infants.Citation79
Hence, HMOs are considered to promote a shift in T-cell response toward a more balanced Th1/Th2-cytokine production and low-level immunity,Citation11 while inflammatory cytokine expression patterns of infants fed with HMO-supplemented formula and exclusively breastfed infants are considered to be similar.Citation5
In a study of 266 infants followed for 5 years, infants born to secretor mothers were reported to have lower incidence of IgE-mediated eczema at 2 years, while authors also noted that 2′-FL was significantly associated with a lower incidence of any (acute or delayed) allergic disease in infants born with C-section.Citation89 In addition, 2-year-old children who were born through C-section and fed on an infant formula supplemented with 2′-FL were reported to have a lower risk of developing IgE-associated allergies compared to those fed unsupplemented formula.Citation105
In a past study in the LIFE Child cohort, authors suggested possible indirect influences of allergic sensitization in the mother (based on IgE level) on HMO in human milk (indirectly via TGF beta2 and IgA) along with a dependency between human milk IgA and specific HMOs (6’SL in particular).Citation100
Nonetheless, it remains unclear whether specific HMO are more protective against allergy than other components,Citation100 while in a recent study overall HMO profiles were reported to differ significantly between sensitized vs non-sensitized infants, whereas no positive or negative association was noted between sensitization and individual or total HMO.Citation99
The exact role of the diverse HMO structures in inducing microbiome and immune development and providing protection against infections also remains unclarified.Citation8 Indeed, the onset of IgE-associated allergic manifestations has recently been suggested to be linked to FUT2-dependent oligosaccharide composition in human milk among infants with a high hereditary risk for allergies and those born by C-section.Citation31,Citation89
Owing to growing evidence on the composition and effects of HMOs and the progress in biotechnology in the last years, there is increased availability of infant formulas comprising HMOs added to the complex mixture of prebiotic oligosaccharides.Citation31 However, available studies regarding the impact of HMOs on infection and immune function are limitedCitation93 and most have focused on safety rather than on anti-infective or immunomodulatory profile.Citation84,Citation106 Hence, further clinical studies are needed to determine the full potential of HMOs within the early life immune development in order to clarify which HMO to be added to infant formula and the optimal strategies for concentration, composition and combination to prevent and treat allergy development in early and later life.Citation8,Citation31,Citation78,Citation93
Potential utility of HMO-supplemented formula in infants and children with CMPA
The IgE-mediated acute allergic reactions (wheezing, urticaria, vomiting, and anaphylaxis), non-IgE-mediated reactions, or mixed immune reactions can induce food allergy, while cow’s milk and eggs are the most common food allergens in childhood food allergy.Citation107–Citation112
Overall, the management of CMPA is based on three intervention strategies including primary prevention of initial IgE sensitization, secondary prevention of the triggering of allergic reactions in IgE-sensitized children and tertiary prevention to reduce the expression of end-organ allergic disease in case of known food allergy via avoidance of allergic food and induction of tolerance.Citation110,Citation113–Citation116
Although the benefits of human milk has consistently been reported in several areas (ie decreased risk of infections, overweightness and diabetes and increased cognitive functions), there is conflicting evidence regarding its role in the prevention of allergy.Citation95,Citation117
Past studies, mainly focused on IgE mediated CMPA, indicated that the incidence of CMPA in the first year of life is significantly lower in exclusively breastfed infants than in those fed by cow’s milk based infant formula with intact protein (<0.5 vs 2–7.5%).Citation95 Hence, it has been suggested that modifying human milk composition by selected interventions may enable more suitable human milk with the capacity to combat allergy epidemics in addition to infectious disease in offspring.Citation95,Citation118
HMOs are considered likely to modulate the susceptibility to both IgE and non-IgE mediated allergy in this regard, by affecting the immune development, gut inflammation and microbiota of the offspring, through indirect (prebiotics for gut microbiota) and direct systemic immunomodulatory effects (reduced antigen-antibody complex-induced chemokine release, improved Th1/Th2 balance).Citation90,Citation119,Citation120
The likelihood of HMO to attenuate allergic symptoms has been reported in a mouse CMPA model study,Citation91 while preclinical experiments indicated that HMOs are likely to induce tolerance development via interaction with human dendritic cells.Citation78
In a past study in breastfed infants with and without CMPA, the authors reported that all mothers with an infant with delayed-onset CMPA were reported to be secretors (active FUT2, milk containing 2ʹFL and LNFP I), whereas those with an infant with immediate-type (IgE-mediated) CMPA were non-secretor (FUT2 negative) mothers.Citation13
Data from the first hypoallergenicity study by Nowak-Wegrzyn et al related to use of an HMO-supplemented eHF in CMPA have confirmed the hypoallergenicity of the HMO-supplemented eHF and indicated the presence of the comparable levels of 2′FL and LNnT in the eHF and in the human milk.Citation9
Authors also noted that while HMO are manufactured by bio-fermentation from lactose, there is no risk of residual milk allergen contamination due to removal of potential residual proteins via several purification steps.Citation9 In fact, given that highly purified lactose is another microbiome-modifying substrate, authors also have hypothesized that the concomitant presence of lactose and HMO in the eHF may offer beneficial synergistic effects to the infants with CMPA in terms of developing gut microbiome and immune system.Citation9,Citation121,Citation122 Hence, authors suggested the supplementation of eHF with 2′FL to be a safe strategy in the management CMPA, not increasing the risk of clinical reactions compared to the non-HMO control formula.Citation9
Nonetheless, the potential utility of HMO-supplemented formula in the management of CMPA still needs further exploration, particularly in terms of their potential to accelerate tolerance development or to reduce the frequency of infections in infants and children with CMPA.Citation15,Citation123
Conclusions
This review by pediatric gastroenterology and allergy-immunology experts emphasize the marked contribution of HMOs to the beneficial effects of human milk in early life in terms of provision of healthy neonatal microbial colonization, fine-tuning of inflammatory processes and immune defense and maturation. The participating experts consider HMOs amongst the most critical bioactive components of human milk, given that they act as antimicrobials and antivirals by preventing pathogen adhesion to epithelial cells, as intestinal epithelial cell modulators by enhancing maturation of intestinal mucosa and intestinal epithelial barrier function, as prebiotics and effectors of the gut microbiota by selectively enriching gut bacteria and thereby promoting healthy microbiota composition and as immunomodulators by modulating immune cells indirectly via changing the infant gut microbiota composition, and directly via affecting immune cells on a systemic level. The potential advantages of HMO-supplemented formula over GOS and FOS supplemented formulas are considered to be ability of HMOs to form the preferred substrate for bifidobacteria and suppress potential gut pathogens, to positively influence gut epithelial integrity, apoptosis, and intestinal permeability and to have indirect and direct immunomodulatory properties.
The participating experts emphasize that reduced gut microbial diversity and dysbiosis during early life as well as induction of a Th2-skewed immune response are considered a risk factor for immune-mediated diseases, such as allergy and asthma in early life. Accordingly, given the marked impact of HMOs on development of healthy gut microbiota and indirect (pathogen decoy capacity, the prebiotic effect, the stimulatory effects on SCFA production and tDCs) and direct anti-inflammatory and immune modulatory functions that promote a shift in T-cell response toward a more balanced Th1/Th2-cytokine production, the participating experts consider the proposed link between HMOs and prevention of allergy to be primarily based on the effects of HMO on gut microbiota, intestinal mucosal barrier and immunomodulation.
The increased availability of HMO from commercial sources as well as accumulating evidence on safety and tolerability of HMO-supplemented formulas seem important given that they seem to be promising alternatives in the management of infants and children with CMPA due to beneficial effects on gut microbiota, intestinal mucosal barrier and immunomodulation as well as anti-inflammatory and anti-infective properties. Accordingly, representing the most critical bioactive component of human milk, responsible for gastrointestinal and immune benefits, HMO-supplemented formulas seem to have potential for provision of infants with CMPA with a formula that brings the similar health benefits with the human milk. Nonetheless, the effects of individual as well as complex mixtures of HMO in relation to well-defined clinical and immune outcomes and tolerance development needs to be further explored to fully realize the immunomodulatory mechanisms and the potential for HMO in prevention of allergic disease development and in the management of CMPA. This review is an expert panel summary report addressing the biological roles of HMOs and their beneficial effects in early life with special emphasis on CMPA to increase awareness about CMPA and to achieve a consensus amongst the different specialties in the CMPA patient care via panel discussions regarding the unmet needs and controversial topics. Hence, focusing on not only the overall beneficial effects of HMOs in early life but also specifically addressing the utility of HMO-supplemented formula in the management of CMPA and in the development of tolerance in the early life with potential long-term positive impacts, this paper provides the opinion and perspectives of the medical community and may help to inform the design of future HMO studies. The expert panel suggests the long-term effects of different HMOs on development of tolerance in early life, their effects on gut microbiota, intestinal mucosal barrier, immunomodulation and immune maturation are the relevant clinical aspects to address when investigating the role of HMOs in prevention of allergy and in reducing the severity of allergy.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Acknowledgments
The authors would like to thank Cagla Ayhan, MD and Prof. Sule Oktay, MD, PhD from KAPPA Consultancy Training Research Ltd, Istanbul who provided editorial support funded by Abbott Nutrition Turkey.
Disclosure
Bulent Enis Sekerel reports speaker fees from Abbott, Abdi Ibrahim, and Sandoz, outside the submitted work. Aydan Kansu reports speaker fees from Abbott, outside the submitted work. The authors declare that they have no other conflicts of interest in this work.
Additional information
Funding
References
- World Health Organization. Maternal, Newborn, Child and Adolescent Health. Geneva: World Health Organization; 2017. Available from: http://www.who.int/maternal_child_adolescent/topics/child/nutrition/breastfeeding/en/. Accessed January 4, 2021..
- Agostoni C, Braegger C, Decsi T, et al; ESPGHAN Committee on Nutrition. Breast-feeding: a commentary by the ESPGHAN Committee on Nutrition. J Pediatr Gastroenterol Nutr. 2009;49(1):112–125. doi:10.1097/MPG.0b013e31819f1e05
- Bode L. Recent advances on structure, metabolism, and function of human milk oligosaccharides. J Nutr. 2006;136(8):2127–2130. doi:10.1093/jn/136.8.2127
- Vandenplas Y, Berger B, Carnielli VP, et al. Human milk oligosaccharides: 2ʹ-Fucosyllactose (2ʹ-FL) and Lacto-N-Neotetraose (LNnT) in infant formula. Nutrients. 2018;10(9):1161. doi:10.3390/nu10091161
- Plaza-Díaz J, Fontana L, Gil A. Human milk oligosaccharides and immune system development. Nutrients. 2018;10(8):1038. doi:10.3390/nu10081038
- Akkerman R, Faas MM, de Vos P. Non-digestible carbohydrates in infant formula as substitution for human milk oligosaccharide functions: effects on microbiota and gut maturation. Crit Rev Food Sci Nutr. 2019;59(9):1486–1497. doi:10.1080/10408398.2017.1414030
- Hegar B, Wibowo Y, Basrowi RW, et al. The role of two human milk oligosaccharides, 2ʹ-fucosyllactose and Lacto-N-Neotetraose, in infant nutrition. Pediatr Gastroenterol Hepatol Nutr. 2019;22(4):330–340. doi:10.5223/pghn.2019.22.4.330
- Ayechu-Muruzabal V, van Stigt AH, Mank M, et al. Diversity of human milk oligosaccharides and effects on early life immune development. Front Pediatr. 2018;6:239. doi:10.3389/fped.2018.00239
- Nowak-Wegrzyn A, Czerkies L, Reyes K, Collins B, Heine RG. Confirmed hypoallergenicity of a novel whey-based extensively hydrolyzed infant formula containing two human milk oligosaccharides. Nutrients. 2019;11(7):1447. doi:10.3390/nu11071447
- Donovan SM, Comstock SS. Human milk oligosaccharides influence neonatal mucosal and systemic immunity. Ann Nutr Metab. 2016;69 Suppl 2(Suppl2):42–51.
- Bode L. Human milk oligosaccharides: every baby needs a sugar mama. Glycobiology. 2012;22(9):1147–1162. doi:10.1093/glycob/cws074
- Azad MB, Konya T, Guttman DS, et al. Infant gut microbiota and food sensitization: associations in the first year of life. Clin Exp Allergy. 2015;45(3):632–643. doi:10.1111/cea.12487
- Seppo AE, Autran CA, Bode L, Järvinen KM. Human milk oligosaccharides and development of cow’s milk allergy in infants. J Allergy Clin Immunol. 2017;139(2):708–711. doi:10.1016/j.jaci.2016.08.031
- Gibson GR, Wang X. Regulatory effects of bifidobacteria on the growth of other colonic bacteria. J Appl Bacteriol. 1994;77(4):412–420. doi:10.1111/j.1365-2672.1994.tb03443.x
- Wiciński M, Sawicka E, Gębalski J, Kubiak K, Malinowski B. Human milk oligosaccharides: health benefits, potential applications in infant formulas, and pharmacology. Nutrients. 2020;12(1):266. doi:10.3390/nu12010266
- Harmsen HJ, Wildeboer-Veloo AC, Raangs GC, et al. Analysis of intestinal flora development in breast-fed and formula-fed infants by using molecular identification and detection methods. J Pediatr Gastroenterol Nutr. 2000;30(1):61–67. doi:10.1097/00005176-200001000-00019
- Puccio G, Alliet P, Cajozzo C, et al. Effects of infant formula with human milk oligosaccharides on growth and morbidity: a randomized multicenter trial. J Pediatr Gastroenterol Nutr. 2017;64(4):624–631. doi:10.1097/MPG.0000000000001520
- Aly E, Darwish AA, Lopez-Nicolas R, Frontela-Saseta C, Ros-Berruezo G. Bioactive components of human milk: similarities and differences between human milk and infant formula, selected topics in breastfeeding, R. Mauricio Barría P. IntechOpen. 2018. Available from: https://www.intechopen.com/chapters/58668. Accessed August 27, 2021.
- Ballard O, Morrow AL. Human milk composition: nutrients and bioactive factors. Pediatr Clin North Am. 2013;60(1):49–74. doi:10.1016/j.pcl.2012.10.002
- Levy O. Innate immunity of the newborn: basic mechanisms and clinical correlates. Nat Rev Immunol. 2007;7(5):379–390. doi:10.1038/nri2075
- Newburg DS, He Y. Neonatal gut microbiota and human milk glycans cooperate to attenuate infection and inflammation. Clin Obstet Gynecol. 2015;58(4):814–826. doi:10.1097/GRF.0000000000000156
- Kulinich A, Liu L. Human milk oligosaccharides: the role in the fine-tuning of innate immune responses. Carbohydr Res. 2016;432:62–70. doi:10.1016/j.carres.2016.07.009
- Lloyd-Price J, Abu-Ali G, Huttenhower C. The healthy human microbiome. Genome Med. 2016;8(1):51. doi:10.1186/s13073-016-0307-y
- Turfkruyer M, Verhasselt V. Breast milk and its impact on maturation of the neonatal immune system. Curr Opin Infect Dis. 2015;28(3):199–206. doi:10.1097/QCO.0000000000000165
- Cacho NT, Lawrence RM. Innate immunity and breast milk. Front Immunol. 2017;8:584. doi:10.3389/fimmu.2017.00584
- Futata EA, Fusaro AE, de Brito CA, Sato MN. The neonatal immune system: immunomodulation of infections in early life. Expert Rev Anti Infect Ther. 2012;10(3):289–298. doi:10.1586/eri.12.9
- Renz H, Holt PG, Inouye M, Logan AC, Prescott SL, Sly PD. An exposome perspective: early-life events and immune development in a changing world. J Allergy Clin Immunol. 2017;140(1):24–40. doi:10.1016/j.jaci.2017.05.015
- Eidelman AI. Breastfeeding and the use of human milk: an analysis of the American Academy of Pediatrics 2012 breastfeeding policy statement. Breastfeed Med. 2012;7(5):323–324. doi:10.1089/bfm.2012.0067
- Oddy WH. Breastfeeding, childhood asthma, and allergic disease. Ann Nutr Metab. 2017;70(Suppl 2):26–36. doi:10.1159/000457920
- Vieira Borba V, Sharif K, Shoenfeld Y. Breastfeeding and autoimmunity: programing health from the beginning. Am J Reprod Immunol. 2018;79:1. doi:10.1111/aji.12778
- Munblit D, Peroni DG, Boix-Amorós A, et al. Human milk and allergic diseases: an unsolved puzzle. Nutrients. 2017;9(8):894. doi:10.3390/nu9080894
- Akobeng AK, Ramanan AV, Buchan I, Heller RF. Effect of breast feeding on risk of coeliac disease: a systematic review and meta-analysis of observational studies. Arch Dis Child. 2006;91(1):39–43. doi:10.1136/adc.2005.082016
- Perkin MR, Logan K, Tseng A, et al. Randomized trial of introduction of allergenic foods in breast-fed infants. N Engl J Med. 2016;374(18):1733–1743. doi:10.1056/NEJMoa1514210
- WHO. Global Strategy for Infant and Young Child Feeding, the Optimal Duration of Exclusive Breastfeeding. Geneva, Switzerland: World Health Organization; 2001.
- Lönnerdal B, Hernell O. An opinion on “staging” of infant formula- a developmental perspective on infant feeding. J Pediatr Gastroenterol Nutr. 2016;62(1):9–21. doi:10.1097/MPG.0000000000000806
- Martin CR, Ling PR, Blackburn GL. Review of infant feeding: key features of breast milk and infant formula. Nutrients. 2016;8(5):279. doi:10.3390/nu8050279
- Boehm G, Stahl B. Oligosaccharides from milk. J Nutr. 2007;137(3Suppl 2):847S–849S. doi:10.1093/jn/137.3.847S
- Thurl S, Munzert M, Henker J, et al. Variation of human milk oligosaccharides in relation to milk groups and lactational periods. Br J Nutr. 2010;104(9):1261–1271. doi:10.1017/S0007114510002072
- McGuire MK, Meehan CL, McGuire MA, et al. What’s normal? Oligosaccharide concentrations and profiles in milk produced by healthy women vary geographically. Am J Clin Nutr. 2017;105(5):1086–1100. doi:10.3945/ajcn.116.139980
- Thum C, Wall CR, Weiss GA, Wang W, Szeto IM, Day L. Changes in HMO concentrations throughout lactation: influencing factors, health effects and opportunities. Nutrients. 2021;13(7):2272. doi:10.3390/nu13072272
- Plows JF, Berger PK, Jones RB, et al. Longitudinal changes in Human Milk Oligosaccharides (HMOs) over the course of 24 months of lactation. J Nutr. 2021;151(4):876–882. doi:10.1093/jn/nxaa427
- Siziba LP, Mank M, Stahl B, et al. Human milk oligosaccharide profiles over 12 months of lactation: the Ulm SPATZ Health Study. Nutrients. 2021;13(6):1973. doi:10.3390/nu13061973
- Berger P, Plows J, Jones R, et al. Human milk oligosaccharides are stable over one-week of lactation and over six-hours following a standardized meal current developments in nutrition. Curr Dev Nutr. 2021;5(Supplement_2):719. doi:10.1093/cdn/nzab046_016
- Chouraqui J-P. Does the contribution of human milk oligosaccharides to the beneficial effects of breast milk allow us to hope for an improvement in infant formulas? Crit Rev Food Sci Nutr. 2021;61:1503–1514. doi:10.1080/10408398.2020.1761772
- Yu Y, Mishra S, Song X, et al. Functional glycomic analysis of human milk glycans reveals the presence of virus receptors and embryonic stem cell biomarkers. J Biol Chem. 2012;287(53):44784–44799. doi:10.1074/jbc.M112.425819
- Goehring KC, Kennedy AD, Prieto PA, Buck RH. Direct evidence for the presence of human milk oligosaccharides in the circulation of breastfed infants. PLoS One. 2014;9(7):e101692. doi:10.1371/journal.pone.0101692
- Bode L. The functional biology of human milk oligosaccharides. Early Hum Dev. 2015;91(11):619–622. doi:10.1016/j.earlhumdev.2015.09.001
- Smilowitz JT, O’Sullivan A, Barile D, German JB, Lönnerdal B, Slupsky CM. The human milk metabolome reveals diverse oligosaccharide profiles. J Nutr. 2013;143(11):1709–1718. doi:10.3945/jn.113.178772
- Xu G, Davis JC, Goonatilleke E, Smilowitz JT, German JB, Lebrilla CB. Absolute quantitation of human milk oligosaccharides reveals phenotypic variations during lactation. J Nutr. 2017;147(1):117–124. doi:10.3945/jn.116.238279
- Smilowitz JT, Lebrilla CB, Mills DA, German JB, Freeman SL. Breast milk oligosaccharides: structure-function relationships in the neonate. Annu Rev Nutr. 2014;34:143–169. doi:10.1146/annurev-nutr-071813-105721
- Bode L, Jantscher-Krenn E. Structure-function relationships of human milk oligosaccharides. Adv Nutr. 2012;3(3):383S–391S. doi:10.3945/an.111.001404
- Lewis ZT, Totten SM, Smilowitz JT, et al. Maternal fucosyltransferase 2 status affects the gut bifidobacterial communities of breastfed infants. Microbiome. 2015;3:13. doi:10.1186/s40168-015-0071-z
- Newburg DS, Ruiz-Palacios GM, Altaye M, et al. Innate protection conferred by fucosylated oligosaccharides of human milk against diarrhea in breastfed infants. Glycobiology. 2004;14(3):253–263. doi:10.1093/glycob/cwh020
- Rudloff S, Pohlentz G, Borsch C, Lentze MJ, Kunz C. Urinary excretion of in vivo 13C-labelled milk oligosaccharides in breastfed infants. Br J Nutr. 2012;107(7):957–963. doi:10.1017/S0007114511004016
- Eiwegger T, Stahl B, Haidl P, et al. Prebiotic oligosaccharides: in vitro evidence for gastrointestinal epithelial transfer and immunomodulatory properties. Pediatr Allergy Immunol. 2010;21(8):1179–1188. doi:10.1111/j.1399-3038.2010.01062.x
- Ackerman DL, Doster RS, Weitkamp JH, Aronoff DM, Gaddy JA, Townsend SD. Human milk oligosaccharides exhibit antimicrobial and antibiofilm properties against Group B Streptococcus. ACS Infect Dis. 2017;3(8):595–605. doi:10.1021/acsinfecdis.7b00064
- Moore RE, Xu LL, Townsend SD. Prospecting human milk oligosaccharides as a defense against viral infections. ACS Infect Dis. 2021;7(2):254–263. doi:10.1021/acsinfecdis.0c00807
- Craft KM, Townsend SD. Mother knows best: deciphering the antibacterial properties of human milk oligosaccharides. Acc Chem Res. 2019;52(3):760–768. doi:10.1021/acs.accounts.8b00630
- Ruiz-Palacios GM, Cervantes LE, Ramos P, Chavez-Munguia B, Newburg DS. Campylobacter jejuni binds intestinal H(O) antigen (Fuc alpha 1, 2Gal beta 1, 4GlcNAc), and fucosyloligosaccharides of human milk inhibit its binding and infection. J Biol Chem. 2003;278:14112–14120. doi:10.1074/jbc.M207744200
- Ida¨npa¨a¨n-Heikkila¨ I, Simon PM, Zopf D, et al. Oligosaccharides interfere with the establishment and progression of experimental pneumococcal pneumonia. J Infect Dis. 1997;176:704–712. doi:10.1086/514094
- Morrow AL, Ruiz-Palacios GM, Altaye M, et al. Human milk oligosaccharides are associated with protection against diarrhea in breast-fed infants. J Pediatr. 2004;145(3):297–303. doi:10.1016/j.jpeds.2004.04.054
- Lin AE, Autran CA, Szyszka A, et al. Human milk oligosaccharides inhibit growth of group B Streptococcus. J Biol Chem. 2017;292(27):11243e9. doi:10.1074/jbc.M117.789974
- Cheng Y-J, Yeung C-Y. Recent advance in infant nutrition: human milk oligosaccharides. Pediatr Neonatol. 2021;62(4):347–353. doi:10.1016/j.pedneo.2020.12.013
- Nolan LS, Rimer JM, Good M. The role of human milk oligosaccharides and probiotics on the neonatal microbiome and risk of necrotizing enterocolitis: a narrative review. Nutrients. 2020;12(10):3052. doi:10.3390/nu12103052
- Craft KM, Gaddy JA, Townsend SD. Human Milk Oligosaccharides (HMOs) sensitize group B Streptococcus to clindamycin, erythromycin, gentamicin, and minocycline on a strain specific basis. ACS Chem Biol. 2018;13(8):2020–2026. doi:10.1021/acschembio.8b00661
- Chen X. Human Milk Oligosaccharides (HMOS): structure, function, and enzyme-catalyzed synthesis. Adv Carbohydr Chem Biochem. 2015;72:113–190.
- Kuntz S, Kunz C, Rudloff S. Oligosaccharides from human milk induce growth arrest via G2/M by influencing growth-related cell cycle genes in intestinal epithelial cells. Br J Nutr. 2009;101(9):1306–1315. doi:10.1017/S0007114508079622
- Angeloni S, Ridet JL, Kusy N, et al. Glycoprofiling with micro-arrays of glycoconjugates and lectins. Glycobiology. 2005;15(1):31–41. doi:10.1093/glycob/cwh143
- Asakuma S, Hatakeyama E, Urashima T, et al. Physiology of consumption of human milk oligosaccharides by infant gut-associated bifidobacteria. J Biol Chem. 2011;286(40):34583–34592. doi:10.1074/jbc.M111.248138
- Plöger S, Stumpff F, Penner GB, et al. Microbial butyrate and its role for barrier function in the gastrointestinal tract. Ann N Y Acad Sci. 2012;1258:52–59. doi:10.1111/j.1749-6632.2012.06553.x
- Reichardt N, Duncan SH, Young P, et al. Phylogenetic distribution of three pathways for propionate production within the human gut microbiota. ISME J. 2014;8(6):1323–1335. doi:10.1038/ismej.2014.14
- Holscher HD, Davis SR, Tappenden KA. Human milk oligosaccharides influence maturation of human intestinal Caco-2Bbe and HT-29 cell lines. J Nutr. 2014;144(5):586–591. doi:10.3945/jn.113.189704
- Garrido D, Kim JH, German JB, Raybould HE, Mills DA. Oligosaccharide binding proteins from bifidobacterium longum subsp. infantis reveal a preference for host glycans. PLoS One. 2011;6(3):e17315. doi:10.1371/journal.pone.0017315
- De Leoz ML, Kalanetra KM, Bokulich NA, et al. Human milk glycomics and gut microbial genomics in infant feces show a correlation between human milk oligosaccharides and gut microbiota: a proof-of-concept study. J Proteome Res. 2015;14(1):491–502. doi:10.1021/pr500759e
- Marcobal A, Sonnenburg JL. Human milk oligosaccharide consumption by intestinal microbiota. Clin Microbiol Infect. 2012;18(suppl 4):12–15. doi:10.1111/j.1469-0691.2012.03863.x
- Rautava S, Luoto R, Salminen S, Isolauri E. Microbial contact during pregnancy, intestinal colonization and human disease. Nat Rev Gastroenterol Hepatol. 2012;9(10):565–576. doi:10.1038/nrgastro.2012.144
- Simon AK, Hollander GA, McMichael A. Evolution of the immune system in humans from infancy to old age. Proc Biol Sci. 2015;282(1821):20143085.
- Xiao L, van De Worp WR, Stassen R, et al. Human milk oligosaccharides promote immune tolerance via direct interactions with human dendritic cells. Eur J Immunol. 2019;49(7):1001–1014. doi:10.1002/eji.201847971
- Goehring KC, Marriage BJ, Oliver JS, Wilder JA, Barrett EG, Buck RH. Similar to those who are breastfed, infants fed a formula containing 2ʹ-fucosyllactose have lower inflammatory cytokines in a randomized controlled trial. J Nutr. 2016;146(12):2559–2566. doi:10.3945/jn.116.236919
- Reverri EJ, Devitt AA, Kajzer JA, Baggs GE, Borschel MW. Review of the clinical experiences of feeding infants formula containing the human milk oligosaccharide 2ʹ-fucosyllactose. Nutrients. 2018;10(10):1346. doi:10.3390/nu10101346
- Kunz C, Rudloff S, Baier W, Klein N, Strobel S. Oligosaccharides in human milk: structural, functional, and metabolic aspects. Annu Rev Nutr. 2000;20:699–722. doi:10.1146/annurev.nutr.20.1.699
- Vandenplas Y, Zakharova I, Dmitrieva Y. Oligosaccharides in infant formula: more evidence to validate the role of prebiotics. Br J Nutr. 2015;113(9):1339–1344. doi:10.1017/S0007114515000823
- Petschacher B, Nidetzky B. Biotechnological production of fucosylated human milk oligosaccharides: prokaryotic fucosyltransferases and their use in biocatalytic cascades or whole cell conversion systems. J Biotechnol. 2016;235:61–83. doi:10.1016/j.jbiotec.2016.03.052
- Marriage BJ, Buck RH, Goehring KC, Oliver JS, Williams JA. Infants fed a lower calorie formula with 2ʹFL show growth and 2ʹFL uptake like breast-fed infants. J Pediatr Gastroenterol Nutr. 2015;61(6):649–658. doi:10.1097/MPG.0000000000000889
- Matsuki T, Yahagi K, Mori H, et al. A key genetic factor for fucosyllactose utilization affects infant gut microbiota development. Nat Commun. 2016;24(7):11939. doi:10.1038/ncomms11939
- Smith-Brown P, Morrison M, Krause L, Davies PSW, Weir TL. Mothers secretor status affects development of childrens microbiota composition and function: a Pilot Study. PLoS One. 2016;11(9):e0161211. doi:10.1371/journal.pone.0161211
- Román E, Moreno Villares JM, Domínguez Ortega F, et al. Real-world study in infants fed with an infant formula with two human milk oligosaccharides. Nutr Hosp. 2020;37(4):698–706.
- Kajzer J, Oliver J, Marriage B. Gastrointestinal tolerance of formula supplemented with oligosaccharides. FASEB J. 2016;30:671.
- Sprenger N, Odenwald H, Kukkonen AK, Kuitunen M, Savilahti E, Kunz C. FUT2-dependent breast milk oligosaccharides and allergy at 2 and 5 years of age in infants with high hereditary allergy risk. Eur J Nutr. 2017;56(3):1293–1301. doi:10.1007/s00394-016-1180-6
- Zehra S, Khambati I, Vierhout M, Mian MF, Buck R, Forsythe P. Human milk oligosaccharides attenuate antigen-antibody complex induced chemokine release from human intestinal epithelial cell lines. J Food Sci. 2018;83(2):499–508. doi:10.1111/1750-3841.14039
- Castillo-Courtade L, Han S, Lee S, Mian FM, Buck R, Forsythe P. Attenuation of food allergy symptoms following treatment with human milk oligosaccharides in a mouse model. Allergy. 2015;70(9):1091–1102. doi:10.1111/all.12650
- Zuurveld M, van Witzenburg NP, Garssen J, et al. Immunomodulation by human milk oligosaccharides: the potential role in prevention of allergic diseases. Front Immunol. 2020;11:801. doi:10.3389/fimmu.2020.00801
- Triantis V, Bode L, van Neerven RJJ. Immunological effects of human milk oligosaccharides. Front Pediatr. 2018;6:190. doi:10.3389/fped.2018.00190
- Aitoro R, Paparo L, Amoroso A, et al. Gut microbiota as a target for preventive and therapeutic intervention against food allergy. Nutrients. 2017;9(7):672. doi:10.3390/nu9070672
- Vandenplas Y, Meyer R, Chouraqui JP, et al. The role of milk feeds and other dietary supplementary interventions in preventing allergic disease in infants: fact or fiction? Clin Nutr. 2021;40(2):358–371. doi:10.1016/j.clnu.2020.10.025
- Morrow AL, Ruiz-Palacios GM, Altaye M, et al. Human milk oligosaccharide blood group epitopes and innate immune protection against campylobacter and calicivirus diarrhea in breastfed infants. Adv Exp Med Biol. 2004;554:443–446.
- Etzold S, Bode L. Glycan-dependent viral infection in infants and the role of human milk oligosaccharides. Curr Opin Virol. 2014;7:101–107. doi:10.1016/j.coviro.2014.06.005
- Moukarzel S, Bode L. Human milk oligosaccharides and the preterm infant: a journey in sickness and in health. Clin Perinatol. 2017;44(1):193–207. doi:10.1016/j.clp.2016.11.014
- Miliku K, Robertson B, Sharma AK, et al. Human milk oligosaccharide profiles and food sensitization among infants in the CHILD Study. Allergy. 2018;73(10):2070–2073. doi:10.1111/all.13476
- Michel L, Shevlyakova M, Ní Cléirigh E, et al. Novel approach to visualize the inter-dependencies between maternal sensitization, breast milk immune components and human milk oligosaccharides in the LIFE child cohort. PLoS One. 2020;15(4):e0230472. doi:10.1371/journal.pone.0230472
- Doherty AM, Lodge CJ, Dharmage SC, Dai X, Bode L, Lowe AJ. Human milk oligosaccharides and associations with immune-mediated disease and infection in childhood: a systematic review. Front Pediatr. 2018;6:91. doi:10.3389/fped.2018.00091
- Xiao L, Van’t Land B, van de Worp WRPH, Stahl B, Folkerts G, Garssen J. Early-life nutritional factors and mucosal immunity in the development of autoimmune diabetes. Front Immunol. 2017;8:1219. doi:10.3389/fimmu.2017.01219
- Comstock SS, Li M, Wang M, et al. Dietary human milk oligosaccharides but not prebiotic oligosaccharides increase circulating natural killer cell and mesenteric lymph node memory T cell populations in noninfected and rotavirus-infected neonatal piglets. J Nutr. 2017;147(6):1041–1047. doi:10.3945/jn.116.243774
- Eiwegger T, Stahl B, Schmitt J, et al. Human milk–derived oligosaccharides and plant-derived oligosaccharides stimulate cytokine production of cord blood T-cells in vitro. Pediatr Res. 2004;56(4):536–540. doi:10.1203/01.PDR.0000139411.35619.B4
- Sprenger N, Lee LY, De Castro CA, Steenhout P, Thakkar SK, Wiley AS. Longitudinal change of selected human milk oligosaccharides and association to infants’ growth, an observatory, single center, longitudinal cohort study. PLoS One. 2017;12(2):e0171814. doi:10.1371/journal.pone.0171814
- Meli F, Puccio G, Cajozzo C, et al. Growth and safety evaluation of infant formulae containing oligosaccharides derived from bovine milk: a randomized, double-blind, noninferiority trial. BMC Pediatr. 2014;14(1):306. doi:10.1186/s12887-014-0306-3
- Lee S. IgE-mediated food allergies in children: prevalence, triggers, and management. Korean J Pediatr. 2017;60(4):99–105. doi:10.3345/kjp.2017.60.4.99
- Sicherer SH, Sampson HA. Food allergy: epidemiology, pathogenesis, diagnosis, and treatment. J Allergy Clin Immunol. 2014;133(2):291–307. doi:10.1016/j.jaci.2013.11.020
- Rona RJ, Keil T, Summers C, et al. The prevalence of food allergy: a meta-analysis. J Allergy Clin Immunol. 2007;120(3):638–646. doi:10.1016/j.jaci.2007.05.026
- Fiocchi A, Brozek J, Schünemann H, et al. World Allergy Organization (WAO) Diagnosis and Rationale for Action against Cow’s Milk Allergy (DRACMA) guidelines. World Allergy Organ J. 2010;3(4):57–161.
- Kansu A, Yüce A, Dalgıç B, Şekerel BE, Çullu-çokuğraş F, Çokuğraş H. Consensus statement on diagnosis, treatment and follow-up of cow’s milk protein allergy among infants and children in Turkey. Turk J Pediatr. 2016;58(1):1–11. doi:10.24953/turkjped.2016.01.001
- Kahveci M, Koken G, Şahiner ÜM, Soyer Ö, Şekerel BE. Immunoglobulin E-mediated food allergies differ in east Mediterranean children aged 0–2 years. Int Arch Allergy Immunol. 2020;181(5):365–374. doi:10.1159/000505996
- Sackesen C, Altintas DU, Bingol A, et al. Current trends in tolerance induction in cow’s milk allergy: from passive to proactive strategies. Front Pediatr. 2019;7:372. doi:10.3389/fped.2019.00372
- Du Toit G, Tsakok T, Lack S, Lack G. Prevention of food allergy. J Allergy Clin Immunol. 2016;137(4):998–1010. doi:10.1016/j.jaci.2016.02.005
- Crittenden RG, Bennett LE. Cow’s milk allergy: a complex disorder. J Am Coll Nutr. 2005;24(6 Suppl):582S–591S. doi:10.1080/07315724.2005.10719507
- Yüce A, Dalgıç B, Çullu-çokuğraş F, et al. Cow`s milk protein allergy awareness and practice among Turkish pediatricians: a questionnaire-survey. Turk J Pediatr. 2017;59(3):233–243. doi:10.24953/turkjped.2017.03.002
- Victora CG, Bahl R, Barros AJ, França GV, Horton S, Krasevec J. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. 2016;387(10017):475–490. doi:10.1016/S0140-6736(15)01024-7
- Munblit D, Verhasselt V. Allergy prevention by breastfeeding: possible mechanisms and evidence from human cohorts. Curr Opin Allergy Clin Immunol. 2016;16(5):427–433. doi:10.1097/ACI.0000000000000303
- D’Auria E, Salvatore S, Pozzi E, et al. Cow’s milk allergy: immunomodulation by dietary intervention. Nutrients. 2019;11(6):1399. doi:10.3390/nu11061399
- Dzidic M, Mira A, Artacho A, Abrahamsson TR, Jenmalm MC, Collado MC. Allergy development is associated with consumption of breastmilk with a reduced microbial richness in the first month of life. Pediatr Allergy Immunol. 2020;31(3):250–257. doi:10.1111/pai.13176
- Thompson-Chagoyan OC, Fallani M, Maldonado J, et al. Faecal microbiota and short-chain fatty acid levels in faeces from infants with cow’s milk protein allergy. Int Arch Allergy Immunol. 2011;156(3):325–332. doi:10.1159/000323893
- Berni Canani R, De Filippis F, Nocerino R, et al. Gut microbiota composition and butyrate production in children affected by non-IgE-mediated cow’s milk allergy. Sci Rep. 2018;8(1):12500. doi:10.1038/s41598-018-30428-3
- O’Mahony L, Renz H, Forbes-Blom E, Nowak-Wegrzyn A. Human milk oligosaccharides: new ways to shape the gut microbiome in cow’s milk protein allergy. EMJ Allergy Immunol. 2019;4(1):48–54.