
Abstract
Background
Allergy can start at early ages, with genetic and environmental factors contributing to its development.
Aim
The study aimed to describe the pattern of sensitisation and allergy in children and adolescents of Spanish versus Moroccan ancestry but born in the same rural area of Spain.
Methods
Participants were children and adolescents (3–19 years) of Spanish or Moroccan descent, born in Blanca, Murcia (Spain). A detailed questionnaire was completed, and skin prick tests were performed to assess reactions to the most prevalent pollen allergens (O. europaea, P. pratense, S. kali, C. arizonica, P. acerifolia, A. vulgaris and P. judaica) plus molecular components Ole e 1 and Ole e 7. The association with ancestry was verified by studying participants’ parents.
Results
The study included 693 participants: 48% were aged 3–9 years and 52%, 10–19 years; 80% were of Spanish descent and 20% of Moroccan descent. Sensitisation to Olea europaea, Phleum pratense, Salsola kali and Cupressus arizonica were slightly higher in the Spanish group. The only significant differences were observed in sensitisation to Ole e 1 (p=0.02). Rhinitis, conjunctivitis, and rhinitis plus asthma were significantly higher in the Spanish group (p=0.03, p=0.02, p=0.007, respectively). The sensitisation pattern differed between Spanish and Moroccan parents, and between Moroccan parents and their children, but not between Spanish parents and their children.
Conclusion
Both environment and ancestry may influence sensitisation and symptoms. Although the environment seems to have a stronger influence, other factors may contribute to the differences in prevalence and in the clinical entities in people of Spanish versus Moroccan descent.
Plain Language Summary
Sensitisation and allergy to inhalants—especially pollen—are increasing worldwide. We did a large study set in a well-defined ecosystem to understand how the environment and individual characteristics contribute to allergy.
We included children and adolescents as well as their parents, analysing them according to their ancestry: Spanish versus Moroccan. Our results indicate that although parents differ in the sensitisation pattern and frequency, in children and adolescents it is similar. Moreover, our data suggest that environment has a stronger influence than ancestry in the induction of sensitisation.
Second generation immigrants do not have a different risk for sensitisation and allergy than native children and adolescents of any age.
Introduction
Over 20% of the population in high-income countries suffers from common allergies, incurring a high burden on healthcare systems.Citation1,Citation2 Allergy involves a complex interaction between the environment and the genetic response.Citation3–7 The immunological response includes antigen-specific and non-antigen-specific mechanisms. Among the former, there is an association between the IgE response to major pollen and other allergens and specific DR and DQ alleles.Citation8,Citation9 Gheerbrant et al reported a significant association between HLA-class II alleles and the allergens Ole e 1, Phl p 2, Phl p 5, and Pla l 1.Citation10 The non-antigen immunological response depends on the gene polymorphisms involved in innate receptors and signalling pathways.Citation11 Dendritic cells are directly activated by allergens or by epithelial cells that secrete alarmins, leading to Th2 polarization.Citation12 Pollens contain proteolytic enzymes and other components that may interact with epithelial cells, favouring the transportation of allergens.Citation11,Citation13 Other factors also contribute to the allergic response: diesel particles, environmental pollutants, viral infections, and nutrition, among others.Citation11 All these may participate as early as the prenatal period and continue throughout childhood and adolescence.Citation13–16
Epigenetic research has uncovered a link between environmental triggers and genetic response. Acevedo et al reported that DNA methylation from the mother and child are associated with IgE sensitisation to allergens, including pollens, in early life.Citation17 In the prenatal period, these factors may be implicated in the development of allergic diseases and asthma through epigenetic modifications affecting the immunological system, which in turn drive a Th2 response.Citation13,Citation14,Citation18 One study has shown that such modifications are more pronounced in the nasal epithelia than in peripheral blood.Citation19
Allergic rhinitis affects 10% to 30% of the population and is often associated with asthma.Citation20–23 In Spain, the prevalence of asthma is 8.2% in children and 18.8% in adolescents, with pollens standing out as the most common cause.Citation24,Citation25 A survey undertaken in the area where this study took place among the general population, classified according to 10-year age bands, showed that sensitisation increases until age 30–40 years and then gradually declines until age 80.Citation26
The large migration flows, mostly from low- and middle-income to high-income countries, enable the study of both environmental and ancestry-related contributions to the development of allergic diseases.Citation27,Citation28 Migrants may come from countries with very different ecological characteristics. In the case of children and adolescents born and living in the destination country, the influence of environment and ancestry on the development of allergy can be disentangled. This study aimed to describe the pattern of sensitisation and allergy in children and adolescents of different ancestry but born in the same rural area of southeast Spain in order to clarify the contribution of these conditions.
Methods
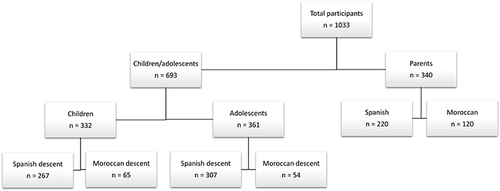
The study took place in Blanca (Murcia, southeast Spain) and included children and adolescents aged 3 to 19 years who were born and lived in the study setting, described in detail elsewhere.Citation29 Participants were classified by age (children: 3–9 years, and adolescents: 10–19 years) and origin (Spanish or Moroccan ancestry). The population was divided into four subgroups: children of Spanish versus Moroccan descent and adolescents of Spanish versus Moroccan descent. Children were considered of Moroccan descent if their parents were born in Morocco and moved to Spain at the age of 20 years or older ().
Figure 1 Participant flow chart.
Participants were recruited at local schools, as described previously.Citation24,Citation25 Each person had a personal interview and completed a questionnaire based on previously validated instruments.Citation30–32 Data collected included demographic, environmental and clinical variables, birth place, date of birth, nationality, type of delivery, school, pets, tobacco exposure, exercise, visits to farmland, work experience on farmland (in the case of adolescents), annual income and family history of atopy. Children’s parents also underwent the interviews, questionnaires, and skin tests.
Skin prick tests (SPT) to the most prevalent pollens, (Olea europaea, Phleum pratense, Salsola kali, Cupressus arizonica, Platanus acerifolia, Artemisia vulgaris and Parietaria judaica) plus Ole e 1 and Ole e 7 (provided by Dr M Villalba, Biochemistry and Molecular Biology, UCM, Spain), were performed as described elsewhereCitation33 (Inmunotek, Madrid, Spain). Participants with a positive SPT (SPT+) to at least one allergen were considered atopic. Clinical entities were labelled as rhinitis, conjunctivitis, and/or asthma.Citation34
Quantitative variables were described using means, medians, standard deviations (SD), and confidence intervals (CI). Qualitative variables, expressed as absolute and relative frequencies, were analysed using the chi-squared test or Fisher’s exact tests when frequencies numbered five or less.
Bivariate analysis was performed to assess the association between sensitisation to each pollen and the risk of having the clinical entity. We also compared the risk of sensitisation to Olea europaea, Ole e 1 and Ole e 7; pollen sensitisation; rhinitis; conjunctivitis; asthma; rhinitis and asthma according to ancestry.
Analyses were done with the Software Package for Social Sciences (SPSS), version 20.0 (SPSS Inc., IBM, Chicago, IL, USA), and SAS v 9.4 Software (SAS Institute, Cary, NC, USA). The level of significance was 0.05.
All participants or their parents/guardians signed informed consent, in compliance with the Declaration of Helsinki.
The study was approved by our Institutional Ethics Committee of Hospital General Universitario Gregorio Marañón (approval number: 41/18) and Research Ethics Committee of the Hospital Universitario Infanta Leonor and Hospital Virgen de la Torre (approval number: 100/20).
Results
We included 693 participants, 48% aged 3–9 years and 52% aged 10–19; 80% were Spanish and 20% of Moroccan descent. Atopy was present in half the participants, with an interquartile range of sensitisation to 1 to 3 pollens. Results of the SPT were positive to Olea europaea in 30% of participants; Phleum pratense, 18%; Salsola kali, 14%; Cupressus arizonica, 12%; and Platanus acerifolia, Artemisia vulgaris and Parietaria judaica, less than 10%.
Compared to children, adolescents were more likely to be female (p<0.05) and to present atopy (p<0.0001) and pollen sensitisation (p=0.03) (). No significant differences were observed between Spanish and Moroccan participants for atopy and pollen sensitisation, though female gender predominated in the Spanish group (p=0.003) ().
Table 1 Participants’ Demographic and Allergy-Related Characteristics, by Age (Children vs Adolescents) and Ancestry (Spanish vs Moroccan Descent)
Adolescents were significantly more likely to show sensitisation to pollens including Olea europaea, Phleum pratense, Salsola kali, and Cupressus arizonica ().
Figure 2 Pollen sensitisation in children vs adolescents.

Children of Spanish descent were more likely to be female (p<0.05), while atopy was slightly but non-significantly more prevalent in children of Moroccan descent (). The opposite was true in adolescents: there were more females among the Moroccan group and more atopy in the Spanish group, though differences were not significant. The number of pollens to which they were sensitised was also similar ().
Spanish children were most commonly sensitised to Olea europaea, followed by Salsola kali, Phleum pratense, Cupressus arizonica, Platanus acerifolia, Artemisia vulgaris, and Parietaria judaica. In Moroccan children, Olea europaea was followed by Phleum pratense, Cupressus arizonica, Salsola kali, Artemisia vulgaris, Parietaria judaica, and Platanus acerifolia. However, these differences did not reach significance. When comparing Spanish and Moroccan adolescents, the pattern of recognition to pollens was similar.
Regarding Olea europaea allergens, 61% of children and 62% of adolescents had SPT+ to the major allergen Ole e 1. The proportion of SPT+ was significantly higher in participants of Spanish compared to Moroccan descent (64% vs 38%; p=0.02). SPT+ to Ole e 7 was found in 9% of children and in 13% of adolescents, and in 15% of the Spanish group compared to 9% of the Moroccan group, though these differences were not significant.
Overall, rhinitis, conjunctivitis, and rhinitis plus asthma were more frequent in adolescents (p<0.0001, p<0.0001 and p<0.007, respectively) and in the Spanish group (p=0.03, p=0.02, p=0.007, respectively), with no significant differences in the prevalence of asthma (). Rhinitis, asthma, and rhinitis plus asthma were more frequent in Spanish children (p<0.05, p<0.05, p<0.05, respectively) (), with no differences for conjunctivitis. In adolescents, conjunctivitis was also more frequent in the Spanish group (p<0.01), with no differences for the remaining clinical entities ().
Table 2 Participants’ Clinical Characteristics, by Age (Children vs Adolescents) and Ancestry (Spanish vs Moroccan Descent)
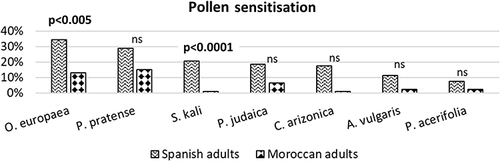
A total of 220 Spanish and 120 Moroccan parents completed the study. Regarding sensitisation, differences were observed not only for the number of people sensitised to pollens but also for the recognition pattern, with Olea europaea and Salsola kali sensitisation higher in Spanish parents (p<0.005 and p<0.0001, respectively) (). Sensitisation to pollen allergens was present in 43% of Spanish fathers and 58% of mothers, with no differences when compared with their children. In the Moroccan group, 20% of the fathers and 30% of the mothers were sensitised, with significant differences compared to their children (p<0.05 in both cases). The annual income in Spanish households was EUR 16,940 (SD 5830) and in Moroccan households, EUR 12,240 (SD 2980) (p<0.0001).
Figure 3 Pollen sensitisation in Spanish vs Moroccan adults.
We considered sensitisation to each pollen as independent variables and tested the association with the clinical entities by constructing three bivariate models. A higher risk of rhinitis was associated with SPT+ to P. pratense (odds ratio [OR] 2.53, 95% confidence interval [CI] 1.69–3.9), C. arizonica (OR 2.57, 95% CI 1.59–4.24), O. europaea (OR 2.81, 95% CI 2.01–4.01), A. vulgaris (OR 2.5, 95% CI 1.16–5.60), and P. judaica (OR 2.31, 95% CI 1.00–5.31), but not to Ole e 1 or Ole e 7. Asthma was associated with SPT+ to P. pratense (OR 1.97, 95% CI 1.19–3.2), O. europaea (OR 1.63, 95% CI 1.04–2.56), P. acerifolia (OR 4, 95% CI 1.91–8.35), and A. vulgaris (OR 3.29, 95% CI 1.48–7.30). No statistically significant differences were found for Ole e 1 or Ole e 7. Rhinitis plus asthma was more frequent in those with SPT+ to P. pratense (OR 2.48, 95% CI 1.46–4.18), C. arizonica (OR 2.04, 95% CI 1.10–3.75), O. europaea (OR 1.63, 95% CI 2.15–3.48), P. acerifolia (OR 4.28, 95% CI 2.02–9.09), and A. vulgaris (OR 4.04, 95% CI 1.81–9.01). As with the other conditions, no statistically significant differences were detected for Ole e 1 and Ole e 7 ().
Table 3 Bivariate Analysis for Sensitisation to Each Pollen and the Risk of Experiencing the Clinical Entities
Concerning ancestry, children and adolescents of Spanish descent were more likely to have SPT+ to Ole e 1 (OR 2.50, 95% CI 1.45–5.54), rhinitis (OR 1.51, 95% CI 1.03–2.2), and conjunctivitis (OR 1.89, 95% CI 1.25–2.85). No differences were observed between participants of Spanish versus Moroccan descent for sensitisation to O. europaea, Ole e 7, pollen sensitisation, asthma, or rhinitis plus asthma.
Discussion
Our main objective was to determine whether differences in ancestry could contribute to the patterns of sensitisation and symptoms found in children and adolescents of Spanish versus Moroccan descent.Citation3–7 Published data are rather heterogeneous, and studies have usually included a low number of cases.Citation35
In our study, adolescents were more likely to be female, to present atopy, and to be sensitised to more pollens (). The pattern of pollen response was similar, with adolescents more frequently sensitised, as reported by other authors,Citation36,Citation37 with highly significant differences for the most prevalent pollens (). Other studies in Spanish adolescents have shown a lower prevalence of atopy and sensitisation to common pollens compared to children.Citation38,Citation39 However, one of these surveys was performed more than 30 years ago before our study, which could explain the difference.Citation38 Regarding the clinical entities, these were significantly more prevalent in adolescents (). In contrast, other authors have reported a higher prevalence of asthmaCitation39 and a lower prevalence of rhinoconjunctivitis in adolescents compared to children.Citation38 These differences could be due to the large number of cases we included and, consequently, the age intervals considered.
The prevalence of atopy was similar in participants of Spanish versus Moroccan descent, whereas the number of pollens involved in sensitisation was slightly but non-significantly higher in the Spanish group (). The frequency of sensitisation to each individual pollen was higher in Spanish children (no significant differences), but the sensitisation pattern was different: Olea europaea was the most prevalent in both groups, but in children of Spanish descent it was followed by Salsola kali, Phleum pratense, and Cupressus arizonica, whereas in children of Moroccan descent Phleum pratense displaced Salsola kali as the second most prevalent. These pollen sensitisation patterns in children may be related to that in their parents, and they tend converge in adolescence, suggesting that the environment has a stronger influence than ancestry as children grow older.Citation40 Lower sensitisation to outdoor allergens has been found in native children compared to immigrants,Citation28,Citation41 although another study reported a higher sensitisation to pollens in Moroccan children born in the Netherlands.Citation42
Concerning allergic diseases – rhinitis, asthma, and rhinitis plus asthma – prevalence was significantly higher in children of Spanish versus Moroccan descent (). These results are consistent with other studies,Citation28,Citation30,Citation43 although one study reported a higher incidence of nasal allergies in immigrant children.Citation32 On the other hand, evidence suggests that asthma has a lower incidence and prevalence in immigrant children and adolescents,Citation30,Citation32,Citation41,Citation44 as well as in second-generation immigrants.Citation40
Since Olea europaea sensitisation was the most prevalent in all groups, as reported in previous studies in this population,Citation24,Citation25 we analysed the response to the two relevant molecular components: Ole e 1 and Ole e 7. Sensitisation to Ole e 1 was significantly higher in the Spanish group, but there were no differences regarding Ole e 7. Other studies have reported higher values for Ole e 7; however, participants were exposed to very high pollen levels and had only severe symptoms.Citation45 Regarding Ole e 1, sensitisation values were almost double in the children of Spanish compared to Moroccan descent. This could suggest that, similarly to the pollen sensitisation profile, genetic and epigenetic factors may be contributors.Citation40,Citation46 According to our data, it seems that once people become positive to Olea europaea, sensitisation to Ole e 1 remains stable over time, but for Ole e 7 an upward trend was observed, which needs to be confirmed with a larger sample size.
Spanish parents showed a high prevalence of atopy, defined as a positive skin prick test, with similar values compared to their children. In contrast, there were significant differences between Moroccan parents and their offspring, with higher values for mothers (p<0.05).
Bivariate logistic regression showed an increased risk of rhinitis, asthma, and rhinitis plus asthma in those sensitised to O. europaea, P. pratense, or A. vulgaris; of rhinitis and rhinitis plus asthma when sensitised to C. arizonica; of asthma and rhinitis plus asthma when sensitised to P. acerifolia; and of rhinitis when sensitised to P. judaica. As reported previously, sensitisation was a risk factor for developing allergic diseases.Citation47 We did not observe any association between Ole e 1 and Ole e 7 sensitisation and any of the allergic conditions analysed, contradicting other published data.Citation45,Citation48
In our study, Spanish ancestry was a risk factor for sensitisation to Ole e 1, rhinitis and conjunctivitis. No differences were found between second-generation Moroccan immigrants and native children and adolescents with regard to O. europaea, Ole e 7, and pollen sensitisation, asthma, or rhinitis plus asthma.
Despite the similarities in sensitisation in Spanish versus Moroccan groups, there were differences in clinical entities and in parents’ sensitisation patterns, suggesting that environment may be more important than genetics or epigenetics.
Several studies have proposed a role for socioeconomic status in the development of allergy as well as for asthma and rhinitis in cases of children living in poverty, with poor housing conditions and parents with low incomes.Citation14,Citation49 However, despite significant differences in annual income in our cohort, this factor did not seem to contribute to these outcomes. In fact, prevalence of rhinitis and asthma was higher in the Spanish group, whose income was higher.
The study has several limitations. We did not include a control group of children and adolescents born in Morocco, as this group was absent in our population. Furthermore, our classification of Moroccan and Spanish origin was based on parental country of birth, entailing a general connection among people from the same geographical origin rather than genetic similarity. Although complex to define,Citation50 this classification has also been used in other studies.Citation43,Citation44 Regarding socioeconomic status, although several variables can be measured as reported by Hill et al, we decided to include only the annual income, but we might also speculate that living and housing conditions were poorer in the Moroccan families.
Summarising, our data suggest that although environment and ancestry may contribute to sensitisation and clinical symptoms, environment has a stronger influence in the induction of sensitisation, while other factors may contribute to the differences observed between the populations studied in the prevalence of the clinical entities. To our knowledge, this is the first population-based study comparing native children and adolescents at all ages with those born in the same area to immigrant parents from a single origin.
Ethical Approval
The study was approved by our Institutional Ethics Committee of Hospital General Universitario Gregorio Marañón (approval number: 41/18) and Research Ethics Committee of the Hospital Universitario Infanta Leonor and Hospital Virgen de la Torre (approval number: 100/20).
Informed Consent
Informed consent was obtained from all individual participants (or their parents or guardians) included in the study, in compliance with the Declaration of Helsinki.
Author Contributions
All authors have made substantial contributions to ALL of the following: made a significant contribution to the work reported in conception, study design, execution, acquisition of data, analysis or interpretation; have drafted or written, or substantially revised or critically reviewed the article; have agreed on the journal to which the article will be submitted; reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage; agree to take responsibility and be accountable for the contents of the article. Maria Luisa Somoza and Natalia Pérez-Sánchez contributed equally to this work as first authors. José Antonio Cornejo-García, Gabriela Canto and Miguel Blanca contributed equally to this work as last authors.
Disclosure
EAFG and EFC are employees of Inmunotek laboratories. The remaining authors declare that they do not have any conflicts of interest.
Acknowledgments
We thank Mr Carlos Goetz (Pertica®, Madrid, Spain) for the statistical analysis and Meggan Harris for language editing. We also thank Universidad Complutense de Madrid (Madrid, Spain) for the academic support.
Additional information
Funding
References
- Pawankar R, Canonica W, Holgate ST, et al. White Book on Allergy. World Health Organization; 2013.
- Zuberbier T, Lotvall J, Simoens S, et al. Economic burden of inadequate management of allergic diseases in the European Union: a GA (2)LEN review. Allergy. 2014;69:1275–1279. doi:10.1111/all.12470
- Wickman M, Asarnoj A, Tillander H, et al. Childhood-to-adolescence evolution of IgE antibodies to pollens and plant foods in the BAMSE cohort. J Allergy Clin Immunol. 2014;2:580–582. doi:10.1016/j.jaci.2013.09.009
- Kulig M, Bergmann R, Klettke U, et al. Natural course of sensitization to food and inhalant allergens during the first 6 years of life. J Allergy Clin Immunol. 1999;103(6):1173–1179. doi:10.1016/S0091-6749(99)70195-8
- Roberts G, Zhang H, Karmaus W, et al. Trends in cutaneous sensitization in the first 18 years of life: results from the 1989 Isle of Wight birth cohort study. Clin Exp Allergy. 2012;42(10):1501–1509. doi:10.1111/j.1365-2222.2012.04074.x
- Arshad SH, Holloway JW, Karmaus W, et al. Cohort Profile: the Isle of Wight Whole Population Birth Cohort (IOWBC). Int J Epidemiol. 2018;47(4):1043–44i. doi:10.1093/ije/dyy023
- Matricardi PM, Bockelbrink A, Keil T, et al. Dynamic evolution of serum immunoglobulin E to airborne allergens throughout childhood: results from the multi-centre allergy study birth cohort. Clin Exp Allergy. 2009;39(10):1551–1557. doi:10.1111/j.1365-2222.2009.03348.x
- Cárdaba B, Cortegano I, Florido F, et al. Update in the understanding of genetic predisposition to olive pollen sensitization. Allergy. 2002;57(s71):41–46. doi:10.1034/j.1398-9995.2002.057s71041.x
- Blumenthal MN, Langefeld CD, Barnes KC, et al. A genome-wide search for quantitative trait loci contributing to variation in seasonal pollen reactivity. J Allergy Clin Immunol. 2006;117:79–85. doi:10.1016/j.jaci.2005.09.038
- Gheerbrant H, Guillien A, Vernet R, et al. Associations between specific IgE sensitization to 26 respiratory allergen molecules and HLA class II alleles in the EGEA cohort. Allergy. 2021;76(8):2575–2586. doi:10.1111/all.14820
- Pointner L, Bethanis A, Thaler M, et al. Initiating pollen sensitization – complex source, complex mechanisms. Clin Transl Allergy. 2020;10(1):36. doi:10.1186/s13601-020-00341-y
- Yang D, Han Z, Oppenheim JJ. Alarmins and immunity. Immunol Rev. 2017;280(1):41–56. doi:10.1111/imr.12577
- McKennan C, Naughton K, Stanhope C, et al. Longitudinal data reveal strong genetic and weak non-genetic components of ethnicity-dependent blood DNA methylation levels. Epigenetics. 2021;16(6):662–676. doi:10.1080/15592294.2020.1817290
- Ho S-M. Environmental epigenetics of asthma: an update. J Allergy Clin Immunol. 2010;126(3):453–465. doi:10.1016/j.jaci.2010.07.030
- Dietert RR, Zelikoff JT. Early-life environment, developmental immunotoxicology, and the risk of pediatric allergic disease including asthma. Birth Defects Res B Dev Reprod Toxicol. 2008;83(6):547–560. doi:10.1002/bdrb.20170
- Galanter JM, Gignoux CR, Oh SS, et al. Differential methylation between ethnic sub-groups reflects the effect of genetic ancestry and environmental exposures. Elife. 2017;6:e20532. doi:10.7554/eLife.20532
- Acevedo N, Scala G, Merid SK, et al. DNA methylation levels in mononuclear leukocytes from the mother and her child are associated with IgE sensitization to allergens in early life. Int J Mol Sci. 2021;22(2):801. doi:10.3390/ijms22020801
- Finch CE, Crimmins EM. Inflammatory exposure and historical changes in human life-spans. Science. 2004;305(5691):1736–1739. doi:10.1126/science.1092556
- Yang IV, Pedersen BS, Liu AH, et al. The nasal methylome and childhood atopic asthma. J Allergy Clin Immunol. 2017;139(5):1478–1488. doi:10.1016/j.jaci.2016.07.036
- Brozek JL, Bousquet J, Agache I, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines—2016 revision. J Allergy Clin Immunol. 2017;140(4):950–958. doi:10.1016/j.jaci.2017.03.050
- Akdis CA, Agache I. Global Atlas of Allergy. The European Academy of Allergy and Clinical Immunology; 2014.
- Leynaert B, Bousquet J, Neukirch C, et al. Perennial rhinitis: an independent risk factor for asthma in nonatopic subjects: results from the European Community Respiratory Health Survey. J Allergy Clin Immunol. 1999;104(2):301–304. doi:10.1016/S0091-6749(99)70370-2
- Platt-Mills T. The allergy epidemics: 1870–2010. J Allergy Clin Immunol. 2015;136(1):3–13. doi:10.1016/j.jaci.2015.03.048
- Somoza ML, Garrido-Arandia M, Victorio Puche L, et al. Peach tree pollen and Pru p 9 may induce rhinoconjunctivitis and asthma in children. Pediatr Allergy Immunol. 2019;30:662–665. doi:10.1111/pai.13067
- Victorio Puche L, Somoza ML, López-Sánchez JD, et al. Peach tree pollen and Pru p 9 sensitisation and allergy in children and adolescents. Int Arch Allergy Immunol. 2019;180(3):212–220. doi:10.1159/000502352
- Victorio Puche L, López-Sánchez D, Blanca-Lopez N, et al. Peach pollen sensitisation is highly prevalent in areas of great extension of peach tree cultivar. J Allergy Clin Immunol. 2018;141(2):AB31. doi:10.1016/j.jaci.2017.12.099
- Cabieses B, Uphoff E, Pinart M, et al. A systematic review on the development of asthma and allergic diseases in relation to international immigration: the leading role of the environment confirmed. PLoS One. 2014;9(8):1–16. doi:10.1371/journal.pone.0105347
- Lombardi C, Fiocchi A, Raffetti E, et al. Cross-sectional comparison of the characteristics of respiratory allergy in immigrants and Italian children. Pediatric Allergy Immunol. 2014;25(5):473–480. doi:10.1111/pai.12250
- Blanca M, Victorio Puche L, Garrido-Arandia M, et al. Pru p 9, a new allergen eliciting respiratory symptoms in subjects sensitized to peach tree pollen. PLoS One. 2020;15(3):e0230010. doi:10.1371/journal.pone.0230010
- Garcia-Marcos L, Robertson CF, Ross Anderson H; ISAAC Phase Three Study Group, et al. Does migration affect asthma, rhinoconjunctivitis and eczema prevalence? Global findings from the international study of asthma and allergies in childhood. The ISAAC Phase Three Study Group. Int J Epidemiol. 43;2014:1846–1854. doi:10.1093/ije/dyu145
- García-Marcos L, Quirós AB, Hernández GG, et al. Stabilization of asthma prevalence among adolescents and increase among schoolchildren (ISAAC phases I and III) in Spain. Allergy. 2004;59(12):1301–1307. doi:10.1111/j.1398-9995.2004.00562.x
- Marcon A, Cazzoletti L, Rava M, et al. Incidence of respiratory and allergic symptoms in Italian and immigrant children. Respir Med. 2011;105(2):204–210. doi:10.1016/j.rmed.2010.09.009
- Heinzerling Heinzerling L, Mari A, Bergmann KC, et al. The skin prick test – European standards. Clin Transl Allergy. 2013;3(1):3. doi:10.1186/2045-7022-3-3
- Johansson SG, Bieber T, Dahl R, et al. Revised nomenclature for allergy for global use: report of the nomenclature review committee of the World Allergy Organization 2003. J Allergy Clin Immunol. 2004;113(5):832. doi:10.1016/j.jaci.2003.12.591
- Tedeschi A, Barcella M, Bo GA, et al. Onset of allergy and asthma symptoms in extra-European immigrants to Milan, Italy: possible role of environmental factors. Clin Exp Allergy. 2003;33(4):449–454. doi:10.1046/j.1365-2222.2003.01628.x
- Nissen SP, Kjaer HF, Høst A, et al. The natural course of sensitization and allergic diseases from childhood to adulthood. Pediatr Allergy Immunol. 2013;24(6):549–555. doi:10.1111/pai.12108
- Schoos AM, Chawes BL, Rasmussen MA, et al. Atopic endotype in childhood. J Allergy Clin Immunol. 2016;137(3):844–851. doi:10.1016/j.jaci.2015.10.004
- García-González JJ, Vega-Chicote JM, Rico P, et al. Prevalence of atopy in students from Málaga, Spain. Ann Allergy Asthma Immunol. 1998;80(3):237–244. doi:10.1016/S1081-1206(10)62964-X
- Segura N, Fraj J, Cubero JL, et al. Mould and grass pollen allergy as risk factors for childhood asthma in Zaragoza, Spain. Allergol Immunopathol. 2016;44(5):455–460. doi:10.1016/j.aller.2016.02.003
- Marks GB. Environmental factors and gene-environment interactions in the aetiology of asthma. Clin Exp Pharmacol Physiol. 2006;33(3):285–289. doi:10.1111/j.1440-1681.2006.04360.x
- Grüber C, Illi S, Plieth A, et al. Cultural adaptation is associated with atopy and wheezing among children of Turkish origin living in Germany. Clin Exp Allergy. 2002;32(4):526–531. doi:10.1046/j.0954-7894.2002.01331.x
- van Amsterdam JG, Bischoff EW, Hady M, et al. The prevalence of allergic sensitisation in immigrant children in The Netherlands. Int Arch Allergy Immunol. 2004;133(3):248–254. doi:10.1159/000076831
- Silverberg JI, Simpson EL, Durkin HG, et al. Prevalence of allergic disease in foreign-born American children. JAMA Pediatr. 2013;167(6):554–560. doi:10.1001/jamapediatrics.2013.1319
- Shani MS, Band Y, Kidon MI, et al. The second generation and asthma: prevalence of asthma among Israeli born children of Ethiopian origin. Respir Med. 2013;107(4):519–523. doi:10.1016/j.rmed.2012.12.024
- Alcántara M, Sáenz de San Pedro B, Cañada C, et al. Steps towards clarifying the clinical relevance of minor olive allergens in areas with extremely high levels of olive pollen. J Investig Allergol Clin Immunol. 2017;27(2):138–140. doi:10.18176/jiaci.0134
- Chan MA, Ciaccio CE, Gigliotti MN, et al. DNA methylation levels associated with race and childhood asthma severity. J Asthma. 2017;54(8):825–832. doi:10.1080/02770903.2016.1265126
- Barber D, de la Torre F, Feo F, et al. Understanding patient sensitization profiles in complex pollen areas: a molecular epidemiological study. Allergy. 2008;63(11):1550–1558. doi:10.1111/j.1398-9995.2008.01807.x
- Florido Lopez JF, Quiralte Enriquez J, de Saavedra Alías JM A, et al. An allergen from Olea europaea pollen (Ole e 7) is associated with plant-derived food anaphylaxis. Allergy. 2002;71:53–59. doi:10.1034/j.1398-9995.2002.057s71053.x
- Hill TD, Graham LM, Divgi V. Racial disparities in pediatric asthma: a review of the literature. Curr Allergy Asthma Rep. 2011;11(1):85–90. doi:10.1007/s11882-010-0159-2
- Mathieson I, Scally A. What is ancestry? PLoS Genet. 2020;16(3):e1008624. doi:10.1371/journal.pgen.1008624