
Abstract
Background
Allergic bronchopulmonary aspergillosis (ABPA) primarily complicates the course of asthma, cystic fibrosis, and chronic obstructive pulmonary disease (COPD). Mortality data of ABPA and the difference in all-cause mortality between ABPA with and without COPD are not available.
Objective
We investigated the difference in all-cause mortality between ABPA with and without COPD.
Methods
A retrospective review was performed among patients with the diagnosis of ABPA at Peking University People’s Hospital between January 2010 and March 2022. Logrank test was performed to investigate the difference between all-cause mortality for ABPA with and without COPD and Cox regression analysis was performed to investigate the independent risk factors for all-cause mortality in patients with ABPA.
Results
Sixty-one patients with ABPA were enrolled in this study. The follow-up duration was 50.38 months (3–143 months). In the COPD group, 7 patients died (7/10), while in the non-COPD group, 4 patients died (4/51). The 1-year survival rates of ABPA with and without COPD were 60% and 97.8%, respectively. The 5-year survival rates of ABPA with and without COPD were 40% and 94%, respectively. The Cox regression analysis showed that higher C-reactive protein (CRP) (HR = 1.017, 95% CI 1.004–1.031, P = 0.013) and complicating COPD (HR = 8.525, 95% CI 1.827–39.773, P = 0.006) were independent risk factors associated with mortality in patients with ABPA.
Conclusion
The all-cause mortality for ABPA with COPD is higher than that for ABPA without COPD. Higher CRP and complicating COPD are independent risk factor for mortality in patients with ABPA.
Introduction
Allergic bronchopulmonary aspergillosis (ABPA) is an allergic pulmonary disease caused by a hypersensitivity reaction to Aspergillus species.Citation1,Citation2 A meta-analysis has shown that the prevalence of ABPA in adults with asthma worldwide ranges from 0.72% to 3.5%,Citation3 and 2.5% of non-smoking adult asthma patients in China meet the diagnostic criteria for ABPA,Citation4 which reveals that ABPA is not a rare disease in asthma patients. Chronic obstructive pulmonary disease (COPD),Citation5–7 bronchiectasis,Citation8 and cystic fibrosisCitation9 can also be complicated by ABPA. Agarwal et al initially described the occurrence of ABPA in COPD in 2008.Citation10 Its prevalence ranges from 2% to 15%, with a pooled prevalence of about 9.5%,Citation11 suggesting that ABPA is not a rare comorbidity of COPD. It is well known that COPD has high morbidity and mortality worldwide.Citation12 The presence of Aspergillus sensitization in COPD is associated with frequent exacerbations,Citation13 bronchiectasis,Citation7 and poor lung function.Citation5,Citation14 Considering the fact that the combination with COPD can significantly increase the mortality of patients with asthma,Citation15 COPD may also have a similar impact on patients with ABPA. Most studies performed in patients with ABPA were case reports or cross-sectional studies with the follow-up duration ranging from 3 months to 43.7 months,Citation16–20 and few studies focused on the long-term follow-up and prognosis, especially for ABPA with COPD. Additionally, the mortality of ABPA and the difference between all-cause mortality for ABPA with and without COPD have never been reported.Citation16–23 Hence, this study aimed to retrospectively analyze the follow-up data of patients with ABPA to explore the difference between all-cause mortality for ABPA with and without COPD and to promote early identification and intervention of severe and high-risk patients.
Methods
Study Design and Ethics Approval
This study was a retrospective clinical data analysis, and the research protocol was approved by the Ethics Committee of Peking University People’s Hospital. The requirement for obtaining informed consent was waived due to the retrospective nature of the study, but all data were anonymized and data confidentiality was maintained.
Study Subjects
The medical records of patients diagnosed with ABPA in the outpatient or inpatient department of Respiratory and Critical Care Medicine from January 2010 to March 2022 in the information system of Peking University People’s Hospital were reviewed using “allergic bronchopulmonary aspergillosis” as the search term.
Inclusion and Exclusion Criteria
Patients with ABPA who met the diagnostic criteria of the “Expert Consensus on the Diagnosis and Treatment of Allergic Bronchopulmonary Aspergillosis” (2017 edition) were included in the study,Citation24 and patients with insufficient diagnostic evidence and less than 3 months of follow-up were excluded from the study. The diagnosis of COPD complied with the diagnostic criteria of the Guidelines for the Diagnosis and Treatment of COPD (2013 Revised Edition).Citation25 The diagnosis of asthma complied with the diagnostic criteria of the Guidelines for the Prevention and Treatment of Bronchial Asthma (2016 Edition).Citation26 The diagnosis of bronchiectasis complied with the diagnostic criteria of the Expert Consensus on the Diagnosis and Treatment of Adult Bronchiectasis (2012 Edition).Citation27 Central bronchiectasis (CB) was defined using two different criteria, depending on whether bronchiectasis was confined to the medial half (point midway between the hilum and chest wall) or the medial two-thirds of the lung.Citation28
Data Collection
Data, including general information, clinical manifestations, laboratory tests, chest high-resolution computed tomography (HRCT), pulmonary function (Jaeger, Germany), diagnosis course, follow-up time, treatment medicine, and survival status, were collected from the medical records of patients. Serum total immunoglobulin E (IgE) was assessed using Roche Cobas e601 electrochemiluminescence instrument; Aspergillus fumigatus m3 allergen among Thermo Fisher Scientific detection reagents was used to assess Aspergillus fumigatus specific IgE (Sp-IgE). Results of laboratory tests, chest HRCT, and pulmonary function were obtained when the patients were diagnosed with ABPA for the first time in our hospital or in another hospital. An arterial blood gas test was performed in patients without oxygen uptake before treatment.
Statistical Analysis
Data were analyzed, and graphs were drawn with SPSS (version 26.0; SPSS, Chicago, IL, USA). Categorical variables were expressed as numbers and percentages. Continuous variables were expressed as mean ± standard deviation or median with interquartile range (lQR; 25th to 75th percentile). Categorical variables were compared using Chi-square test, while Student’s t-test or Mann–Whitney U-test was used for continuous variables. Kaplan-Meier analysis was used to compare the survival distribution among different groups and Kaplan–Meier survival curves for different groups of subjects were obtained and plotted. To identify variables independently associated with mortality, we conducted the Cox regression analysis by including the variables with P ≤ 0.05 in the univariate analysis. P < 0.05 was considered to indicate statistical significance.
Results
Baseline Data of Patients with ABPA
Seventy-five inpatients and outpatients were retrieved, and 13 patients with an inadequate diagnosis and 1 patient with a follow-up period of less than 3 months were excluded. Among the 61 patients, 58 patients fully met the diagnostic criteria, and total IgE of three patients was not more than 1000 IU/mL (764.8–978.2 IU/mL). All of them were taking glucocorticoids while testing of total IgE, their clinical characteristics and imaging features met the diagnostic criteria of ABPA, and glucocorticoids and antifungal drugs were effective. Finally, 61 patients were included, including 29 males. All patients had stage I disease on admission. The follow-up time ranged from 3 to 143 months, with an average follow-up time of 50.38 months.Ten patients with COPD were identified; all of them had a long-term history of heavy smoking (32.5 [27.5–55.13] pack-years) and definite emphysema, and 4 of them were complicated with asthma. There were 11 deaths during 252 person-years of follow-up. Among the 11 patients who died, 7 died of respiratory disease, 2 died of colon cancer, 1 died of cardiovascular and cerebrovascular events, and 1 died due to an unknown cause. Seven of the 10 patients with COPD died (70%). Among the 50 patients without COPD, 4 patients died (7.84%). The mean survival time of ABPA with and without COPD was 37 months and 129.98 months, respectively. The mean age at the time of death for ABPA with and without COPD was 76 years and 74 years, respectively.
Comparison of Characteristics Between Patients Who Had ABPA with or Without COPD
Age (76.00 ± 9.64 years vs 52.78 ± 16.77 years, P < 0.001), proportion of male patients (10 [100%] vs 21 [41.18%], P = 0.002), smoking history (10 [100%]) vs 11 [21.57%], P < 0.001), pack-years of smoking (0 [0–0] vs 32.5 [27.5–55.13], P < 0.001), death rate (7 [70%] vs 4 [7.84%], P < 0.001), neutrophil count (7.45 ± 2.64 × 109/L vs 5.12 ± 3.05 × 109/L, P = 0.029), neutrophil percentage (69.04 ± 25.5% vs 55.08 ± 15.73%, P = 0.041), neutrophil-to-lymphocyte ratio (NLR) (8.68 [4.33–16.66] vs 1.90 [1.43–5.86], P < 0.001), and C-reactive protein (CRP) (15.10 mg/L [7.91–100.84 mg/L] vs 3.94 mg/L [1.00–15.40 mg/L], P = 0.011) at diagnosis were significantly higher in patients with COPD than in patients without COPD. Body mass index (BMI) (20.61±2.59 kg/m2 vs 23.07± 3.48 kg/m2, P = 0.040), eosinophil count (0.09× 109/L [0.03–0.65 × 109/L] vs 0.62 × 109/L [0.24–0.94 × 109/L], P=0.026), eosinophil percentage (1.45% [0.23–6.85%] vs 9.6 [2.61–13.5%], P = 0.006), proportion of patients with asthma (4 [40.00%] vs 48 [94.12%], P < 0.001) and with allergic rhinitis (1 [10.00%] vs 32 [60.78%], P = 0.009), forced expiratory volume in one second (FEV1)/forced vital capacity (FVC) (46.94 ± 7.79% vs 63.08 ± 15.9%), P < 0.001), percentage of FEV1 predicted (FEV1%) (37.17 ± 8.59% vs 64.82 ± 26.25%), P < 0.001), peak expiratory flow percentage (PEF) (2.80 L/s [2.57–3.58 L/s] vs 4.70 L/s [3.21–6.55 L/s], P = 0.012), percentage of PEF predicted (PEF%) (40.30% [32.50–47.15%] vs 73.80 [49.50–95.30%], P = 0.001), percentage of the diffusing capacity of carbon monoxide predicted (DLCO%) (56.56 ± 14.66% vs 75.68 ± 22.74%, P = 0.021), and diffusing capacity divided by the alveolar volume (DLCO/VA) (0.85 mmol/min/kPa/L [0.64–1.04 mmol/min/kPa/L] vs 1.47 mmol/min/kPa/L [1.24–1.60 mmol/min/kPa/L], P < 0.001) were significantly lower in patients with COPD than in patients without COPD ().
Table 1 Comparison of Characteristics Between Patients Who Had ABPA with or Without COPD
Survival Time and Rate in Patients with ABPA
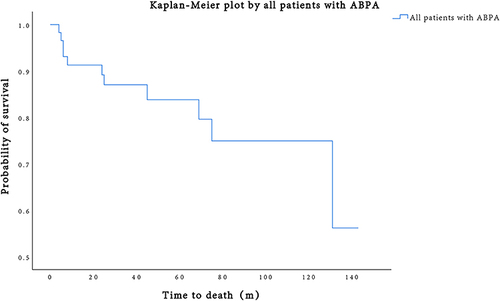
Kaplan-Meier curves showed the overall survival curve of all patients with ABPA. The average survival time was 114 months. The 1-year and 5-year survival rate was 91.3% and 83.8%, respectively ().
Figure 1 Survival curves for all-cause mortality in all patients with ABPA.
Results of the Kaplan-Meier Analysis for Mortality of ABPA
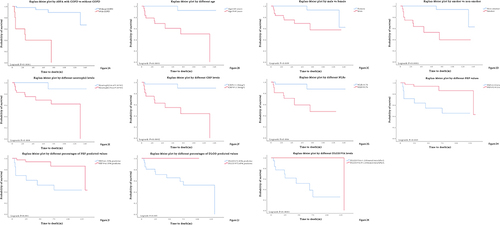
Kaplan-Meier analysis demonstrated that COPD affected the survival time of patients with ABPA, and the all-cause mortality for ABPA with COPD was much higher than that for ABPA without COPD (). According to the results of Kaplan-Meier analysis, male gender, smoking history, older age, higher CRP and NLR, lower PEF, PEF%, DLCO%, and DLCO/VA had a significantly higher risk for all-cause mortality (the cutoff value of continuous variables was calculated by the ROC curve) ( and ).
Table 2 Results of the Kaplan-Meier Analysis for Motality of ABPA
Figure 2 Survival curves for all-cause mortality in patients of different subgroups.
Comparison of the Clinical Characteristics of All Patients with ABPA Between the Death and Survival Groups
Age (73.00 ± 10.02 years vs 52.98 ± 17.37 years, P = 0.001), proportion of male patients (9 [81.82%] vs 22 [44.00%], P = 0.023), smoking history (9 [81.82%] vs 12 [24.00%], P = 0.001), pack-years of smoking (0 [0–0] vs 30 [15–50], P < 0.001), neutrophil count (7.33 ± 2.85 × 109/L vs 5.09 ± 3.01× 109/L, P = 0.030), NLR (6.50 [2.96–14.28] vs 1.97 [1.41–5.88], P = 0.002), CRP (48.16 mg/L [9.72–126.70 mg/L] vs 3.03 mg/L [0.98–10.96 mg/L], P < 0.001), erythrocyte sedimentation rate (ESR) (28.00 mm/h [15.00–67.50 mm/h] vs 13.50 [5.00–26.50 mm/h], P = 0.030), and proportion of patients with COPD (7 [63.64%] vs 3 [6.00%], P < 0.001) were significantly higher in the death group than in the survival group. Proportion of patients with allergic rhinitis (2 [18.18%] vs 30 [60.00%], P = 0.012), PEF (2.71 L/s [2.35–3.67 L/s] vs 4.68 L/s [3.31–6.53 L/s], P = 0.027), PEF% (39.6% [30.55–56.90%] vs 73.50 [48.83–94.48%], P = 0.024), DLCO% (57.57 ± 10.62% vs 76.41 ± 23.51%, P = 0.014), and DLCO/VA (1.04 mmol/min/kPa/L [0.78–1.15 mmol/min/kPa/L] vs 1.48 mmol/min/kPa/L [1.24–1.61 mmol/min/kPa/L], P < 0.001) were significantly lower in patients in the death group than in patients in the survival group (). The detailed condition of the died patients was provided ().
Table 3 Comparison of Clinical Characteristics of All Patients with ABPA Between the Death and Survival Groups
Table 4 The Detailed Condition of the Death Group
Results of Cox Regression Analysis
Cox regression analysis showed that higher CRP (HR = 1.017, 95% CI 1.004–1.031, P = 0.013) and complicating COPD (HR = 8.525, 95% CI 1.827–39.773, P = 0.006) were independent risk factors associated with mortality in patients with ABPA.
Comparison of Characteristics Between Patients Who Had ABPA with or Without CB
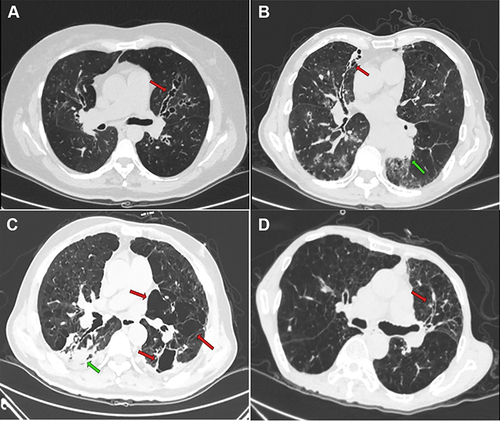
Smoking history (1 [6.25%] vs 20 [44.44%], P = 0.006), pack-years of smoking (0 [0–0] vs 0 [0–18.75], P = 0.025), and BMI (20.75 ± 3.29 kg/m2 vs 23.38 ± 3.27 kg/m2, P = 0.009) were significantly lower in patients with CB than in patients without CB. Eosinophil count (0.77 × 109/L [0.23–0.94 × 109/L] vs 0.48 × 109/L [0.05–0.71 × 109/L], P = 0.029) and Sp-IgE level (13.30 kUA/L [3.50–25.90 kUA/L] vs 0.93 kUA/L [0.54–6.10 kUA/L], P = 0.001) were significantly higher in patients who had ABPA with CB than in patients without CB (). And we showed several typical HRCT photographs of ABPA including 3 died patients ().
Table 5 Comparison of Characteristics Between Patients Who Had ABPA with or Without Central Bronchiectasis
Figure 3 HRCT scans of patients with ABPA.
Discussion
ABPA presents with symptoms that are similar to those of asthma. They include coughing, wheezing, and shortness of breath. Chronic airway diseases, including asthma and COPD, which are the background diseases of ABPA, have a high incidence in the world. Various research studies were performed to assess the characteristics and prognosis of ABPA with asthma, but few studies paid attention to the characteristics and prognosis of ABPA with COPD, although some studies showed that Aspergillus was associated with frequent exacerbations and higher mortality in COPD.Citation29
In this study, we retrospectively analyzed the long-term follow-up data of 61 patients who had ABPA with an average follow-up time of 50.38 months (range, 3–143 months), and we reported that the all-cause mortality rate of ABPA with COPD (70%) was significantly higher than that of ABPA without COPD (7.84%). The Log rank test showed that the mean survival time of ABPA with COPD was 37 months, which was much shorter than that of ABPA without COPD (129.98 months). The cause of death in patients who had ABPA with and without COPD was definitely different. Most patients with COPD and ABPA died of respiratory diseases, such as AECOPD, while death of patients without COPD was usually due to a malignant tumor, and cardiovascular and cerebrovascular events.
However, univariate analysis showed that old age, poor pulmonary function, and severe systemic inflammatory reaction were closely related to the higher mortality of ABPA. The Cox regression analysis showed that complicating COPD (HR = 8.525, 95% CI 1.827–39.773, P = 0.006) was one of the independent risk factors associated with mortality in patients with ABPA. We suppose that all these significant univariate factors are related to COPD.
The main reasons for the increased mortality in patients with COPD include the following: Firstly, the mean age of patients with ABPA and COPD in this study was 76 years, which was much higher than that of patients without COPD (53 years). The mean age of three patients with ABPA and COPD was 77 years in the study by Sun.Citation6 Another study showed that the mean age of 10 patients with ABPA and COPD was 59 years,Citation30 which was in line with the age characteristic of patients with COPD in this study. Therefore, advanced age is a prominent feature of patients with ABPA and COPD, which is in accordance with the different onset age of patients with COPD and asthma. Asthma often occurs in childhood and usually before the age of 40 years, while COPD usually occurs after the age of 50 years in smokers. On the other hand, although the incidence of ABPA in COPD might not be lower than that in asthma,Citation11 the proportion of of ABPA with COPD was much lower than that of ABPA with asthma in most of the current case studies. A previous study in China showed that none of the 77 patients with ABPA had COPD.Citation31 In another study, 1 out of 46 patients with ABPA had COPD,Citation32 and in a recent retrospective analysis by Zeng, 3 out of 193 patients with ABPA had COPD.Citation18 It can be speculated that a large number of patients with COPD and ABPA are underdiagnosed or misdiagnosed, leading to a higher age at the time of first diagnosis in these patients. These two aspects lead to the fact that the age of patients with ABPA and COPD is much higher than that of ABPA patients without COPD. A delayed diagnosis and treatment will lead to gradual aggravation of clinical symptoms, severe airflow obstruction, CB, and other structural lung damage, which seriously affect the quality of life and survival time of patients.
Secondly, patients with COPD have more severe airflow obstruction and significantly reduced diffusing function, which was significantly associated with increased mortality. The univariate analysis and Kaplan-Meier analysis showed that reduced pulmonary ventilation function and diffusing capacity were closely related to COPD and increased mortality. Smoking history was closely associated with genesis and development of COPD and worse pulmonary function, which was also demonstrated in this study. Although a retrospective study found that DLCO/VA was lower in patients who had ABPA with CB,Citation18 CB had no significant association with DLCO/VA in this study. Thus, the important factor leading to the decline in pulmonary ventilation and diffusing capacity in our patients was coexisting COPD, and not CB. Therefore, COPD-induced decline in pulmonary function is an important cause of death in patients with ABPA.
In addition to the significant differences in age and pulmonary function, the inflammatory characteristics were significantly different between patients with COPD and without COPD. Univariate analysis showed that patients with COPD had significantly a higher neutrophil count, neutrophil percentage, CRP and NLR, but the indicators related to ABPA-characteristic allergic inflammation, such as blood eosinophil count and eosinophil percentage, were significantly lower. Agarwal et al found that elderly patients with ABPA had lower serum total IgE and Sp-IgE levels and less bronchiectasis,Citation21 suggesting that patients with ABPA aged over 60 years and with COPD showed a hypoallergenic inflammatory reaction but a severe neutrophilic inflammatory reaction. NLR and CRP are sensitive indicators of systemic infection, and previous studies have found that these indicators are associated with an increased risk of acute exacerbation, hospitalization, and early death in patients with COPD.Citation33–36 We also analyzed the impact of CB on mortality. ABPA with CB did not increase the risk of mortality. Besides, our study also showed that the inflammatory characteristics of patients with COPD were significantly different from those of patients with CB. The former was dominated by increased CRP and neutrophil count, while the latter was dominated by increased ABPA-characteristic allergic inflammation indicators, such as eosinophil count and Sp-IgE level. Previous studies suggested that patients with ABPA and CB have higher levels of total IgE and Sp-IgE, more severe immunoreactivity, more aggressive clinical form and symptoms, and more frequent exacerbations.Citation17,Citation37–39 The prominent inflammatory characteristic of patients with ABPA and COPD suggests that patients with COPD may have more severe airway infections and the type and mechanism of airway inflammation in COPD with ABPA are different from those in typical asthma with ABPA. Th2 inflammation reaction and fungal colonization of the airways are important mechanisms for the pathogenesis of ABPA.Citation40 There is an interaction and overlap between infection and Th2 inflammation of the airways caused by fungal colonization. Airway inflammation was more likely secondary to fungal colonization in patients who had COPD instead of persistent allergy. It remains to be determined whether there are different pathways of airway inflammation in patients with COPD and ABPA and patients with classic asthma and ABPA.
The clinical characteristics and pathogenesis of patients with ABPA and COPD may be different from those of patients with ABPA but without COPD, which can lead to significant differences in mortality. Thus, we should increase the screening of Aspergillus sensitization and ABPA in patients with COPD to reduce misdiagnosis, improve early detection and treatment, and lower mortality. In addition, due to the limited treatment methods for ABPA, glucocorticoids and antifungal drugs are the main medications, and a higher priority is given to glucocorticoids. However, physicians are usually more cautious when applying glucocorticoids in patients with COPD and ABPA, considering their advanced age, more underlying diseases, and worse immune status. Some patients often fail to take a sufficient amount of glucocorticoids and complete the full course of treatment with glucocorticoids. The mechanism of ABPA in COPD should be explored through more research studies to identify the differences from that of ABPA based on classic asthma. It is necessary to further optimize the treatment plan according to the pathogenesis and clinical characteristics of patients with COPD and ABPA to improve their compliance, thereby improving the treatment effect and reducing the mortality.
In summary, the all-cause mortality for ABPA with COPD was much higher than that for ABPA without COPD. Older age, poorer pulmonary function, and a more severe neutrophilic inflammatory reaction were closely related to higher mortality of ABPA with COPD. Higher CRP and complicating COPD were independent risk factors for mortality in patients with ABPA. Patients with COPD should be routinely evaluated for Aspergillus sensitization and ABPA to promote early identification and intervention of severe and high-risk patients and ultimately reduce mortality.
However, our study has some limitations that should be acknowledged. It was a single-center retrospective study with a small sample size. The mortality rate obtained in this study cannot be extrapolated to all patients with ABPA. The laboratory had set the upper limit of the total IgE detection value at 2500 IU/mL, which may have influenced the significance of total IgE. Further, some new biological targeted drugs, such as the anti-IgE antibody omalizumab, were not included in our study.Citation41 Moreover, patients with COPD have a higher mortality rate versus age-matched controls. We did not compare the difference in mortality between COPD with and without ABPA in order to analyze how ABPA can contribute to mortality in patients with COPD and ABPA. Hence, a prospective large-scale research study with a longer follow-up time period is needed to explore the difference in all-cause mortality between ABPA with and without COPD and related risk factors.
Abbreviations
ABPA, Allergic Bronchopulmonary Aspergillosis;; AECOPD, Acute exacerbations of chronic obstructive pulmonary disease; BMI, Body mass index; CB, Central bronchiectasis; COPD, Chronic Obstructive Pulmonary Disease; CRP, C-reactive protein; DLCO, Diffusion capacity of carbon monoxide; VA, Alveolar volume; ESR, Erythrocyte sedimentation rate; FEV1, Forced expiratory volume in one second; FEV1/pred, Percentage of FEV1 predicted; FVC, Forced vital capacity; HRCT, High-resolution computed tomography; IgE, Immunoglobulin E; NLR, Neutrophil-to-lymphocyte ratio; NSCLC, Non-small-cell lung cancer; NSTEMI, Non-ST Segment Elevation Myocardial Infarction; PEF, Peak expiratory flow percentage; PaO2, Partial arterial oxygen pressure; PaCO2, Partial arterial pressure of carbon dioxide; SaO2, Oxygen saturation; Sp-IgE, Aspergillus fumigatus specific IgE; Th2, T helper cell type 2.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
This work was supported by Youth Scientific Research Cultivation Project of Peking University People’s Hospital Research and Development Fund (RDY2021-19). We thank Medjaden Inc. for scientific editing of this manuscript.
Additional information
Funding
References
- Kosmidis C, Denning DW. The clinical spectrum of pulmonary aspergillosis. Thorax. 2015;70(3):270–277. doi:10.1136/thoraxjnl-2014-206291
- Bains SN, Judson MA. Allergic bronchopulmonary aspergillosis. Clin Chest Med. 2012;33(2):265–281. doi:10.1016/j.ccm.2012.02.003
- Denning DW, Pleuvry A, Cole DC. Global burden of allergic bronchopulmonary aspergillosis with asthma and its complication chronic pulmonary aspergillosis in adults. Med Mycol. 2013;51(4):361–370. doi:10.3109/13693786.2012.738312
- Ma YL, Zhang WB, Yu B, Chen YW, Mu S, Cui YL. Prevalence of allergic bronchopulmonary aspergillosis in Chinese patients with bronchial asthma. Chin J Tuberculosis Respir Dis. 2011;34(34):909–913.
- Jin JM, Liu XF, Sun YC. The prevalence of increased serum IgE and Aspergillus sensitization in patients with COPD and their association with symptoms and lung function. Respir Res. 2014;15:130. doi:10.1186/s12931-014-0130-1
- Liu XF, Sun YC, Jin JM, Li R, Liu Y. Allergic bronchopulmonary aspergillosis in patients with chronic obstructive pulmonary disease: report of 3 cases. Chin J Tuberculosis Respir Dis. 2013;36(10):5.
- Agarwal RH, Basanta G, Dheeraj A, et al. Aspergillus hypersensitivity in patients with chronic obstructive pulmonary disease: COPD as a risk factor for ABPA? Med Mycol. 2010;48(7):988–994. doi:10.3109/13693781003743148
- Pasteur MC, Helliwell SM, Houghton SJ, et al. An investigation into causative factors in patients with bronchiectasis. Am J Respir Crit Care Med. 2000;162(4 Pt 1):1277–1284. doi:10.1164/ajrccm.162.4.9906120
- Stevens DA, Moss RB, Kurup VP, et al. Allergic bronchopulmonary aspergillosis in cystic fibrosis--state of the art: cystic fibrosis foundation consensus conference. Clin Infect Dis. 2003;37(Suppl 3):S225–S264. doi:10.1086/376525
- Agarwal R, Srinivas R, Jindal SK. Allergic bronchopulmonary aspergillosis complicating chronic obstructive pulmonary disease. Mycoses. 2008;51(1):83–85. doi:10.1111/j.1439-0507.2007.01432.x
- Muthu V, Prasad KT, Sehgal IS, Dhooria S, Aggarwal AN, Agarwal R. Obstructive lung diseases and allergic bronchopulmonary aspergillosis. Curr Opin Pulm Med. 2021;27(2):105–112. doi:10.1097/MCP.0000000000000755
- López-Campos JL, Tan W, Soriano JB. Global burden of COPD. Respirology. 2016;21(1):14–23. doi:10.1111/resp.12660
- Tiew PY, Ko FWS, Pang SL, et al. Environmental fungal sensitisation associates with poorer clinical outcomes in COPD. Eur Respir J. 2020;56(2):2000418. doi:10.1183/13993003.00418-2020
- Bafadhel M, McKenna S, Agbetile J, et al. Aspergillus fumigatus during stable state and exacerbations of COPD. Eur Respir J. 2014;43(1):64–71. doi:10.1183/09031936.00162912
- Sorino C, Pedone C, Scichilone N. Fifteen-year mortality of patients with asthma-COPD overlap syndrome. Eur J Intern Med. 2016;34:72–77. doi:10.1016/j.ejim.2016.06.020
- Lu HW, Mao B, Wei P, et al. The clinical characteristics and prognosis of ABPA are closely related to the mucus plugs in central bronchiectasis. Clin Respir J. 2020;14(2):140–147. doi:10.1111/crj.13111
- Agarwal R, Garg M, Aggarwal AN, Saikia B, Gupta D, Chakrabarti A. Serologic allergic bronchopulmonary aspergillosis (ABPA-S): long-term outcomes. Respir Med. 2012;106(7):942–947. doi:10.1016/j.rmed.2012.03.001
- Zeng YY, Xue XM, Cai H, et al. Clinical characteristics and prognosis of allergic bronchopulmonary aspergillosis: a retrospective cohort study. J Asthma Allergy. 2022;15:53–62. doi:10.2147/JAA.S345427
- Agarwal R, Aggarwal AN, Sehgal IS, Dhooria S, Behera D, Chakrabarti A. Utility of IgE (total and Aspergillus fumigatus specific) in monitoring for response and exacerbations in allergic bronchopulmonary aspergillosis. Mycoses. 2016;59(1):1–6. doi:10.1111/myc.12423
- Muthu V, Sehgal IS, Prasad KT, et al. Allergic bronchopulmonary aspergillosis (ABPA) sans asthma: a distinct subset of ABPA with a lesser risk of exacerbation. Med Mycol. 2020;58(2):260–263. doi:10.1093/mmy/myz051
- Muthu V, Sehgal IS, Prasad KT, et al. Epidemiology and outcomes of allergic bronchopulmonary aspergillosis in the elderly. Mycoses. 2022;65(1):71–78. doi:10.1111/myc.13388
- Wang SJ, Zhang J, Zhang CP, Shao CZ. Clinical characteristics of allergic bronchopulmonary aspergillosis in patients with and without bronchiectasis. J Asthma. 2021;58(1):1–7. doi:10.1080/02770903.2019.1656230
- Tiew PY, Lim AYH, Keir HR, et al. High frequency of allergic bronchopulmonary aspergillosis in bronchiectasis-COPD overlap. Chest. 2022;161(1):40–53. doi:10.1016/j.chest.2021.07.2165
- Asthma Group of the Respiratory Diseases Branch of the Chinese Medical Association. Experts consensus on diagnosis and treatment of allergic bronchopulmonary aspergillosis. Natl Med J China. 2017;34:2650–2656.
- Chronic Obstructive Pulmonary Disease Group of the Respiratory Diseases Branch of the Chinese Medical Association. The guidelines for the diagnosis and treatment of COPD (2013 revised edition). Chin J Front Med Sci. 2014;2:67–80.
- Lv XD. The diagnostic criteria of the guidelines for the prevention and treatment of bronchial asthma (2016 edition). Chin J Tuberculosis Respir Dis. 2016;39(9):675–697.
- Adult Bronchiectasis Diagnosis and Treatment Expert Consensus Writing Group. Expert consensus on diagnosis and treatment of adult bronchiectasis (2012 edition). Chin J Crit Care Med. 2012;5(5):20–30.
- Hansell DM, Strickland B. High-resolution computed tomography in pulmonary cystic fibrosis. Br J Radiol. 1989;62(733):1–5. doi:10.1259/0007-1285-62-733-1
- Tiew PY, Dicker AJ, Keir HR, et al. A high-risk airway mycobiome is associated with frequent exacerbation and mortality in COPD. Eur Respir J. 2021;57(3):2002050. doi:10.1183/13993003.02050-2020
- Wang MY, Qian YJ, Lin L, Wang HM. Allergic bronchopulmonary aspergillosis in patients with chronic obstructive pulmonary disease: report of 10 cases. Chin J Tuberculosis Respir Dis. 2019;42(7):543–545.
- Zhang MQ, Gao JM. Clinical analysis of 77 patients with allergic bronchopulmonary aspergillosis in Peking Union Medical College Hospital. Acta Acad Med Sinicae. 2017;39(3):352–357. doi:10.3881/j.issn.1000-503X.2017.03.009
- Zou MF, Li S, Yang Y, et al. Clinical features and reasons for missed diagnosis of allergic bronchopulmonary aspergillosis. Natl Med J China. 2019;99(16):1221–1225. doi:10.3760/cma.j.issn.0376-2491.2019.16.006
- Groenewegen KH, Postma DS, Hop WCJ, Wielders PLML, Schlösser NJJ, Wouters EFM. Increased systemic inflammation is a risk factor for COPD exacerbations. Chest. 2008;133(2):350–357. doi:10.1378/chest.07-1342
- Lonergan M, Dicker AJ, Crichton ML, et al. Blood neutrophil counts are associated with exacerbation frequency and mortality in COPD. Respir Res. 2020;21(1):166. doi:10.1186/s12931-020-01436-7
- Yao CY, Liu XL, Tang Z. Prognostic role of neutrophil-lymphocyte ratio and platelet-lymphocyte ratio for hospital mortality in patients with AECOPD. Int J Chron Obstruct Pulmon Dis. 2017;12:2285–2290. doi:10.2147/COPD.S141760
- Xiong W, Xu M, Zhao YF, Wu XL, Pudasaini B, Liu JM. Can we predict the prognosis of COPD with a routine blood test? Int J Chron Obstruct Pulmon Dis. 2017;12:615–625. doi:10.2147/COPD.S124041
- Patterson K, Strek ME. Allergic bronchopulmonary aspergillosis. Proc Am Thorac Soc. 2010;7(3):237–244. doi:10.1513/pats.200908-086AL
- Agarwal R, Gupta D, Aggarwal AN, Behera D, Jindal SK. Allergic bronchopulmonary aspergillosis: lessons from 126 patients attending a chest clinic in north India. Chest. 2006;130(2):442–448. doi:10.1378/chest.130.2.442
- Kumar R, Chopra D, Chopra RD. Evaluation of allergic bronchopulmonary aspergillosis in patients with and without central bronchiectasis. J Asthma. 2002;39(6):473–477. doi:10.1081/JAS-120004905
- Denning DW, Pashley C, Hartl D, et al. Fungal allergy in asthma-state of the art and research needs. Clin Transl Allergy. 2014;4:14. doi:10.1186/2045-7022-4-14
- Ma YL. The use of biological agents for the treatment of allergic bronchopulmonary aspergillosis. Chin J Tuberculosis Respir Dis. 2019;42(11):864–868. doi:10.3760/cma.j.issn.1001-0939.2019.11.017