
Abstract
Eosinophilic asthma is now recognized as an important subphenotype of asthma based on the pattern of inflammatory cellular infiltrate in the airway. Eosinophilic asthma can be associated with increased asthma severity, atopy, late-onset disease, and steroid refractoriness. Induced sputum cell count is the gold standard for identifying eosinophilic inflammation in asthma although several noninvasive biomarkers, including fractional exhaled nitric oxide and periostin, are emerging as potential surrogates. As novel therapies and biologic agents become increasingly available, there is an increased need for specific phenotype-directed treatment strategies. Greater recognition and understanding of the unique immunopathology of this asthma phenotype has important implications for management of the disease and the potential to improve patient outcomes. The present review provides a summary of the clinical features, pathogenesis, diagnosis, and management of eosinophilic asthma.
Introduction
An estimated 8.4% of the US population has a diagnosis of asthma and approximately 10%–20% of those individuals remain poorly controlled despite high-dose inhaled corticosteroids and long-acting beta-agonists.Citation1,Citation2 Asthma has been traditionally defined as a chronic respiratory disease characterized by reversible airflow obstruction, bronchial hyperresponsiveness, and airway inflammation. It is now recognized that the term “asthma” actually represents a heterogeneous collection of respiratory diseases with distinct phenotypes originating from the complex interplay between individual genetic and environmental factors. Therefore, rather than a “one size fits all” approach to asthma treatment, evidence is now emerging that unique pathophysiologic mechanisms may drive airway inflammation in each subtype of the disease and alter the response to conventional therapies. By better identifying asthma phenotypes, we may be able to use more targeted therapies, both existing and novel, to achieve asthma control in patients who have failed standard treatment.
Phenotype-targeted therapies are especially important for patients with severe refractory asthma, who represent less than 10% of all asthmatics, but are responsible for a disproportionate share of morbidity and health care costs related to the disease.Citation3 Several strategies have been proposed to categorize severe asthma phenotypes based on characteristics such as patient age, disease onset, corticosteroid resistance, chronic airflow obstruction, or type of cellular infiltrate in the airway lumen or lung tissue.Citation4,Citation5 A newly proposed approach to asthma classification is based on “endotypes” that represent specific cellular patterns along with clinical characteristics within each patient subgroup.Citation6 Analysis of induced sputum samples has allowed for determination of inflammatory phenotypes according to granulocytic composition, namely eosinophilic, neutrophilic, mixed granulocytic, or paucigranulocytic.Citation7 Interestingly, patients with severe adult-onset asthma can be divided into a neutrophilic inflammatory phenotype or have eosinophilic inflammation that is unresponsive to high-dose steroids.Citation8,Citation9 This discussion focuses on our current understanding of “eosinophilic asthma” as a distinct asthma phenotype in US populations, with special attention paid to pathophysiology, diagnostic evaluation, and management.
Eosinophils in the pathogenesis of asthma
Eosinophils have long been implicated in the pathogenesis of asthma. Post mortem pathologic studies of patients who have died from asthma attacks show airway mucosa infiltrated with activated eosinophils.Citation10 Over 20 years ago, Bousquet et al published their findings demonstrating that chronic asthmatics had an increase in eosinophils in peripheral blood and bronchoalveolar lavage fluid, along with lung biopsy specimens that correlated with the severity of asthma.Citation11 The presence of eosinophils in the airway lumen, as identified by sputum cell counts, has since been shown to be predictive of loss of asthma control after discontinuation of inhaled corticosteroids.Citation12,Citation13 Further, the persistence of eosinophils in sputum despite high doses of corticosteroids may also be a marker of disease severity.Citation14 Generally, the eosinophilic phenotype is associated with a good response to corticosteroids and to T-helper type 2 (Th2) targeted therapy, such as anti-interleukin (IL)-5 treatments discussed below.Citation15–Citation17
Eosinophilic asthma has classically been associated with allergic sensitization and a Th2-dominant inflammatory response. The Th2-driven phenotype arises from dysregulated innate and adaptive immune responses. During allergic sensitization, inhaled allergens are taken up by antigen-presenting dendritic cells in the airway and presented to T-cells.Citation18 The cytokine milieu leads to T-helper cell differentiation and production of IL-4, IL-5, and IL-13, resulting in immunoglobulin (Ig)E class switching, eosinophil recruitment, mucus production, airway hyperresponsiveness, and remodeling features.Citation19,Citation20 IL-5 is a critical cytokine for eosinophil generation in the bone marrow, as well as eosinophil recruitment, activation, and survival. Upon airway allergen re-exposure, allergen cross-linking of IgE on mast cells and basophils results in inflammatory degranulation with the release of preformed and newly synthesized mediators including histamine, cysteinyl leukotrienes, prostaglandin D2, and chemokines, resulting in acute allergic reactions with vasodilation, edema, and bronchospasm. This is followed by the influx of activated cells, including eosinophils and cytokine-producing T cells into the airway, contributing to airway hyperresponsiveness that characterizes an asthma exacerbation.
In addition to the classic allergen-mediated Th2 paradigm, innate immune stimuli such as environmental factors, air pollution, weather changes (eg, thunderstorms), and viral infections may be capable of eliciting Th2 responses associated with eosinophilia.Citation21,Citation22 Cytokines derived from bronchial epithelium, including thymic stromal lymphoprotein, IL-25, and IL-33, are released in response to an allergen, viral antigen, or mucosal injury, and may drive Th2 polarization as well as activation of innate type 2 pathways.Citation23 Thymic stromal lymphopoietin (TSLP) induced by respiratory syncytial virus has been shown to promote a type 2 response to infection by promoting a dendritic cell/CD4+ Th2 cell activation pathway through OX40/OX40 ligand interactions.Citation24,Citation25 TSLP also induces dendritic cells to release chemokine ligand 13 (human monocyte chemoattractant protein-4) and chemokine ligand 17 (thymus and activation regulated chemokine), which recruit Th2 cells via chemokine receptor 4.Citation26 Other cell types including basophils, natural killer T-cells, and group 2 innate lymphoid cells are also important sources of type 2 cytokines, which regulate eosinophil influx into the lungs. Despite the significant complexity of redundant and nonredundant inflammatory pathways in asthma, critical steps that lead to eosinophil influx into the airway have been elucidated.
Recruitment of eosinophils into the airway in allergic asthma is mediated by the coordinated action of cytokines and chemokines including IL-5, IL-13, eotaxins, and the adhesion molecules P-selectin and vascular cell adhesion molecule-1.Citation27 Maturation of eosinophils from myeloid precursors in the bone marrow is promoted by IL-5, IL-3, and granulocyte macrophage-colony stimulating factor (GM-CSF).Citation28 Eosinophils then circulate in the peripheral blood and are normally present in peripheral tissue and respiratory mucosa, but increase in number in the setting of acute inflammation. IL-5 is a potent eosinophil activator and facilitates recruitment into tissues that is further enhanced by eotaxins and chemokine ligand 5 (also known as RANTES) released by immune and airway resident cells.Citation29 GM-CSF is upregulated after allergen challenge and is localized to alveolar macrophages and lymphocytes as well as eosinophils themselves, suggesting an autocrine pathway.Citation30,Citation31 Other chemoattractants for eosinophils include complement product C5a and the lipid mediators platelet-activating factor and leukotriene B4. Upon migration from the blood, eosinophils bind to endothelial cells expressing E-selectin and vascular cell adhesion molecule-1 (ligand for VLA-4 integrin), which facilitate migration into the tissue.Citation32 Eosinophil infiltration also depends on chemokine ligand 11 (eotaxin-1), which is produced by the respiratory epithelium and binds to the eosinophil chemokine receptor 3 (CCR3).Citation33
Once activated, eosinophils secrete their granule contents which consist of four principal proteins: major basic protein, eosinophilic cation protein, eosinophilic-derived neurotoxin, and eosinophil peroxidase. Eosinophils also release inflammatory lipid mediators, including cysteinyl leukotrienes C4 and D4, platelet-activating factor, and prostaglandin D2 which further propagate the allergic response. Murine models have suggested that IL-5 and eosinophils may also promote airway remodeling via eosinophil expression of transforming growth factor-β.Citation34 Other important growth factors and Th2 cytokines that may contribute to airway remodeling in asthma include vascular endothelial growth factor, IL-9, and IL-13, which may also be produced by eosinophils.Citation20 These pathways along with therapeutic targets are highlighted in .
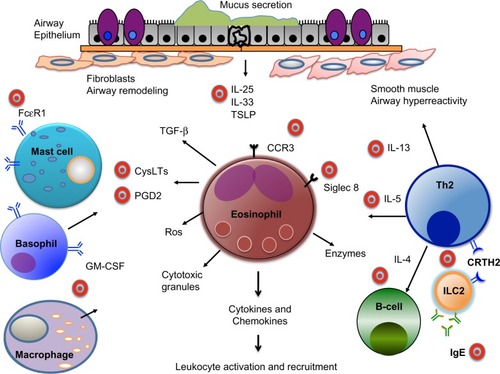
Figure 1 Schematic of eosinophils in airway inflammation and therapeutic targets. In response to allergens, viruses, or mucosal injury, airway epithelial cells produce cytokines, including IL-25, IL-33, and TSLP, which promote differentiation of Th2 cells, as well as activation of mast cells, macrophages, and type 2 innate lymphoid cells. IL-4 and IL-13 produced by Th2 and other cells results in eotaxin production, B-cell IgE class switching, airway hyperresponsiveness, and mucus secretion. IL-5 stimulates bone marrow eosinophil generation, and mediates recruitment, activation, and survival of eosinophils. GM-CSF produced by alveolar macrophages and eosinophils contributes to maturation and survival of eosinophils. Eosinophils release major basic protein, ROS, and enzymes, as well as Th2 cytokines and inflammatory lipid mediators including cysteinyl leukotrienes and prostaglandin D2. These products result in recruitment and activation of immune and structural cells. Further, production of Th2 cytokines and growth factors, such as TGF-β, contribute to features of airway remodeling in chronic asthma. A number of therapeutic targets (depicted by bullseyes) have been identified for eosinophilic asthma and are currently under investigation.
Defining eosinophilic asthma
Eosinophilic asthma has been defined as a distinct phenotype of asthma that is associated with tissue and sputum eosinophilia, thickening of the basement membrane zone, and often by corticosteroid responsiveness.Citation15,Citation35 The advent of sputum induction has allowed for improved classification of airway inflammation, identification of asthma phenotypes, and drawing associations with other biomarkers.Citation35 Sputum cell counts defining eosinophilic asthma vary between studies ranging from 1% to 3%. Importantly, normalization of induced sputum eosinophil counts has also been shown to be an effective strategy for preventing severe asthma exacerbations and hospitalizations, and suggests clinical utility in ongoing asthma management.Citation36
In several studies, the number of eosinophils in induced sputum has been detected at higher levels in patients with more severe asthma.Citation37–Citation39 Woodruff et al demonstrated that the percentage of eosinophils in induced sputum was independently associated with more severe airflow obstruction and methacholine reactivity in over 200 subjects.Citation37 Another study stratified asthmatics into four subgroups based on sputum inflammatory cell type and observed the highest degree of airway hyperresponsiveness to mannitol in the purely eosinophilic group.Citation39 Although these studies further implicate the eosinophil in a subset of severe asthmatics, additional investigations suggest that there may be a dissociation between airway hyperresponsiveness and eosinophilia.Citation40
Early pathologic studies by Wenzel et al led to the description of subgroups of severe asthmatics on the basis of the presence or absence of eosinophils.Citation8 Miranda et al reported that the majority of severe asthmatics had elevated airway eosinophils despite chronic treatment with high-dose oral steroids.Citation41 However, they found that far fewer patients who developed asthma early in life demonstrated tissue eosinophilia, as compared with the group with late-onset asthma (36% early-onset versus 63% late-onset). Surprisingly, there was evidence of persistent eosinophilia in the late-onset asthmatics despite a lower rate of skin prick sensitization. However, in the early onset group, the presence of eosinophils on biopsy was associated with an increased prevalence of near-fatal events (intubations). This study highlights the association between numbers of eosinophils and severity of asthma in patients with corticosteroid-refractory disease and suggests discordance between atopy and eosinophilic airway disease in a subset of patients.
Importantly, ten Brinke et al challenged the notion of steroid-refractory eosinophilic asthma in a follow-up study in which sputum eosinophils were eliminated in nearly all severe asthmatics using high doses of parenteral triamcinolone.Citation42 These results suggest that the persistence of eosinophilia was more likely due to inadequate therapy rather than a lack of steroid response. However, further studies have supported an association between sputum eosinophils and severe adult-onset asthma.Citation9 These individuals are largely nonatopic, yet have persistent eosinophilic airway inflammation, further supporting a distinct underlying mechanism of eosinophilic inflammation apart from allergy.
Notably, eosinophilic asthma is very prevalent in individuals with nonsevere disease. Berry et al studied subjects with mild to moderate asthma and stratified them by the presence or absence of eosinophils in their sputum.Citation15 They found that subjects with eosinophilia had increased thickness of the subepithelial basement membrane zone and improved short-term response to treatment with inhaled corticosteroids. In addition, they found higher numbers of T-lymphocytes, mast cells, and macrophages in the subgroup of subjects with severe asthma and eosinophilia.
In support of distinct subtypes of eosinophilic asthma, airway infiltration of eosinophils is present in other respiratory conditions, including allergic bronchopulmonary aspergillosis, Churg–Strauss syndrome, aspirin-exacerbated respiratory disease, and eosinophilic bronchitis. Eosinophilic bronchitis differs from eosinophilic asthma in several ways. Clinically, patients with eosinophilic bronchitis have symptoms of cough, but in contrast with asthmatics, have normal lung function and lack airway responsiveness.Citation43 Further, although both conditions are associated with eosinophilic infiltration in the airways, they have distinct immunohistochemical features. Biopsy specimens from patients with asthma, as compared with eosinophilic bronchitis, reveal a striking increase in the number of mast cells in smooth muscle bundles.Citation44 Further, vascular endothelial growth factor levels and airway permeability are increased in asthma, but not in eosinophilic bronchitis.Citation45 Vascular endothelial growth factor is believed to increase vascular permeability, promote angiogenesis, and play a role in several aspects of airway remodeling. The principal source of vascular endothelial growth factor in the airway is not entirely clear, but may include eosinophils, macrophages, epithelial cells, and smooth muscle.Citation20 Thus, the presence and activity of other inflammatory cells in conjunction with eosinophils may underlie a severe asthma endotype.
Diagnostic evaluation of eosinophilic asthma
Traditional guideline-based treatment decisions in asthma target symptoms and lung function, but specific therapies targeting the underlying inflammatory process may be needed in a subset of patients. Sputum eosinophils are an accurate reflection of Th2-dominant mechanisms in uncontrolled asthma, and eosinophilic asthma is generally defined by >1%–3% of eosinophils. Induced sputum is the most reliable measure of inflammatory cell counts although quantitative sputum cell counts are difficult to obtain in routine practice and require access to specific laboratories with trained personnel. The utility of several alternative markers of eosinophilic inflammation are currently being investigated including peripheral blood eosinophil counts, fractional exhaled nitric oxide (FeNO), serum IgE, and periostin levels.
Peripheral blood eosinophil counts are easily obtained and widely available, but lack both specificity and sensitivity. Although few asthmatics may demonstrate an increase in blood eosinophils,Citation46 in those asthmatics with peripheral eosinophilia, there is a suggested correlation with severity of asthma symptoms and an inverse correlation in pulmonary function as measured by forced expiratory volume in one second (FEV1).Citation47 Nonetheless, blood eosinophil counts have not been shown to correlate reliably with elevated sputum eosinophils in asthma. Hastie et al recently evaluated multiple variables including exhaled nitric oxide levels, FEV1, total IgE, and blood eosinophil counts in predicting asthma phenotype.Citation48 The authors demonstrated that levels of blood eosinophils >300/μL had a positive predictive value of only 50% in identifying an eosinophilic asthma phenotype based on sputum eosinophils of >2%. Further, longitudinal studies examining sputum cell counts in consecutive exacerbations showed significant heterogeneity in the type of cellular inflammation within the same individuals.Citation49 Taken together, these findings suggest that peripheral blood eosinophilia may be a marker of disease severity in asthma, but does not correlate consistently with sputum eosinophilia.
As discussed, eosinophilic asthma can be associated with Th2-mediated allergic disease and allergen sensitization, especially in earlier onset disease. Surprisingly, there does not appear to be a correlation with total serum IgE, as demonstrated in a study by Good et al in which bronchoscopy was used to assess asthma phenotypes.Citation50 The authors demonstrated a lack of correlation between total IgE levels and the presence of eosinophils in bronchoalveolar lavage fluid or biopsy specimens, despite the fact that over 80% of patients with evidence of eosinophils had positive skin testing. Thus, although IgE levels may be helpful in the diagnosis of allergic bronchopulmonary aspergillosis, with features of asthma and eosinophilia, the total IgE has little utility in evaluation of most patients with asthma.
Nitric oxide is a reactive molecule synthesized by nitric oxide synthase expressed on cells within the airway epithelium. FeNO as measured by breath tests is often used as a noninvasive marker of airway inflammation in asthma. In contrast with bronchoscopy and sputum induction, FeNO measurement is rapid, simple, and noninvasive. There is growing evidence that FeNO measurement may be useful as a clinical tool in managing asthma and guiding therapy; however, conflicting studies have resulted in some controversy about the utility of FeNO.Citation51–Citation53 Smith et al studied more than 90 asthmatics and found that FeNO was a useful tool in stepping down inhaled corticosteroid therapy.Citation54 Tseliou et al also demonstrated that FeNO levels >19 parts per billion predicted sputum eosinophilia with a sensitivity of 78% and a specificity of 73% in patients with moderate to severe asthma, some of whom were prednisone-dependent.Citation55 On the other hand, Nair et al reported a lack of correlation between sputum eosinophil percentages and FeNO levels in patients with prednisone-dependent asthma who participated in a clinical trial with the anti-IL-5 antibody mepolizumab.Citation17
Periostin is an extracellular matrix protein upregulated by IL-13 and has been shown to facilitate allergen-induced eosinophil recruitment to the lungs by mediating eosinophil adhesion to fibronectin.Citation56 In murine models, periostin-deficient mice challenged with Aspergillus fumigatus demonstrated a decrease in airway eosinophilia as compared with wild-type mice, but no change in tissue lymphocytes or neutrophils.Citation56 Further, periostin has been shown to induce survival of lung cancer cells through the Akt/PKB pathway, and perhaps periostin could promote the survival of eosinophils, although this has not been tested.Citation57 Overall, periostin has potential as a systemic biomarker for identification of airway eosinophilia in asthmatics, possibly due to its role in induction of tissue of eosinophilia.
Using a logistic regression model including age, sex, body mass index, IgE levels, blood eosinophils, FeNO levels, and serum periostin levels in 59 patients with severe asthma, Jia et al recently reported that serum periostin was the best predictor of airway eosinophilia.Citation58 A serum periostin level >25 ng/mL had a positive predictive value of 93% and a negative predictive value of 37% for sputum eosinophils (>3%) or tissue eosinophilia. Further, in a recent anti-IL-13 treatment study, patients with higher periostin levels had greater improvements in FEV1 suggesting that periostin levels may be predictive of therapeutic response.Citation59 While the airway epithelium can be stimulated by IL-4 and IL-13 to secrete periostin,Citation60 the precise role of periostin in asthma is not clear. Apart from a role in eosinophilia, animal models suggest that periostin may be involved in airway remodeling via transforming growth factor-β and may also have a protective role in allergen-induced airway hyperresponsiveness.Citation61
A recent study by Kulkarni et al evaluated the use of eosinophil protein in airway macrophages as a noninvasive biomarker of eosinophilic airway inflammation.Citation62 The burden of tissue eosinophilia is a balance between the eosinophilic influx and clearance by airway macrophages. Therefore, they assessed eosinophil protein levels by means of flow cytometry, immunofluorescence, and cytoplasmic hue change after macrophage ingestion of apoptotic eosinophils. They concluded that airway macrophage eosinophil protein content was increased in subjects with severe asthma and may have clinical utility in predicting ongoing eosinophilic inflammation and success of weaning from corticosteroids.
Therapeutics in eosinophilic asthma
Current management of eosinophilic asthma begins with standard guideline-based therapy, including inhaled corticosteroids and bronchodilators which have been reviewed extensively elsewhere.Citation63 Generally, the presence of eosinophils has been associated with responsiveness to corticosteroids although some patients with eosinophilic asthma have been reported to be “steroid-refractory”. Specific therapeutics targeting inflammatory mediators are currently under investigation in clinical trials for patients who have failed standard therapy and remain steroid-dependent or refractory.
Agents targeting corticosteroid resistance
Several mechanisms that may account for corticosteroid-resistant asthma have been reported including activation of p38 mitogen-activated protein kinase and inflammatory genes regulated through transcription factor nuclear factor-κB.Citation64 P38 mitogen-activated protein kinase is important in the activation of GATA3, the master Th2 cytokine transcription factor.Citation65 Small molecule p38 inhibitors have been demonstrated to attenuate asthmatic features in mice.Citation65 However, clinical trials in humans for the treatment of inflammatory disease have been associated with substantial systemic side effects.Citation66 Phosphoinositide 3-kinase (PI3K) also regulates inflammatory pathways, and activation of the isozyme PI3Kδ by oxidative stress may decrease corticosteroid responsiveness through reductions in histone deacetylase 2, an enzyme targeted by theophylline.Citation67 Other mechanisms for steroid-refractory asthma may include increased expression of the alternatively spliced variant of the glucocorticoid receptor and increased production of macrophage migratory inhibitory factor, which may block the anti-inflammatory effects of corticosteroids.Citation67,Citation68
Biologic therapies
Availability of biologic agents for the treatment of asthma began with the approval of an anti-IgE monoclonal antibody, omalizumab (Xolair®; Genentech/Novartis, Basel, Switzerland), for the treatment of uncontrolled disease. Drugs targeting specific Th2 cytokines, including monoclonal antibodies against IL-5 and IL-13, have also shown promise in the treatment of refractory eosinophilic asthma.Citation69 As data accumulate supporting patient-specific and phenotype-directed therapeutic responses, use of these agents may reduce the burden of disease for those with refractory symptoms despite current treatments. However, the cost of such agents may preclude their widespread use, although reductions in emergency room visits and hospitalizations may outweigh the expense of therapy.
Omalizumab
Omalizumab is a recombinant humanized monoclonal antibody (IgG1) that binds to the Fc portion of IgE that recognizes its high-affinity receptor (FcεR1) on the surface of mast cells and basophils, resulting in receptor downregulation and inhibition of inflammatory mediator release.Citation70 Several large-scale randomized controlled trials now support the therapeutic efficacy of subcutaneously administered omalizumab as add-on therapy for severe persistent allergic asthma.Citation71–Citation77 In asthmatic patients inadequately controlled despite high-dose inhaled corticosteroids and long-acting beta-agonist therapy, omalizumab significantly reduced the rate of severe exacerbations and emergency visits.Citation71 Data combined from seven randomized controlled trials indicated that total IgE was the only predictor of response to therapy.Citation78 However, allergic sensitization to aeroallergens by skin prick testing was a key inclusion criterion in several of these studies.Citation71–Citation74
IgE has a central role in the pathophysiology of allergic responses and omalizumab attenuates both the early-phase and late-phase responses to inhaled allergens in patients with asthma.Citation79 While total serum IgE levels do not correlate diagnostically with the degree of tissue eosinophilia, treatment with anti-IgE therapy has been shown to be efficacious and reduce airway and blood eosinophils.Citation80–Citation82 One of the initial studies in asthmatics treated with omalizumab demonstrated a significant reduction in eosinophils in induced sputum and airway tissue (8.0 at baseline compared with 1.5 post-treatment).Citation82 A later report showed that 16 weeks of treatment decreased blood eosinophils from 6.2% at baseline to 1.3%.Citation81 Therefore, while total serum IgE is not useful as a diagnostic marker for eosinophilic asthma, total serum IgE levels should be obtained if considering anti-IgE therapy.
One explanation for the apparent paradox that anti-IgE therapy is useful for treatment in eosinophilic asthma despite IgE levels not being predictive of response may be related to downregulation of FcεR1 on the surface of mast cells, basophils, and dendritic cells by anti-IgE. A reduction in FcεR1-expressing cells limits allergen-induced IgE-mediated responses, preventing cytokine release and eosinophil recruitment into the airway.Citation83 Additionally, treatment with anti-IgE may lead to decreased levels of airway dendritic cellsCitation84 resulting in a reduction in Th2 differentiation and the Th2 cytokines necessary for survival and recruitment of eosinophils. Therefore, while total serum IgE may not be predictive of eosinophilic asthma or clinical response, omalizumab has been shown to have an important role in asthma management and reduces airway eosinophils.
Interestingly, Noga et al have demonstrated that omalizumab may also have proapoptotic effects on eosinophils.Citation79 In a study of 19 patients with allergic asthma, markers of eosinophil apoptosis (Annexin V) were significantly increased in patients who had received 12 weeks of omalizumab as compared with placebo. The authors also showed a reduction in IL-2, IL-13, and GM-CSF+ lymphocytes in the omalizumab group. Reduction in levels of mast cell mediators that promote eosinophil survival may have led to the apoptosis of eosinophils in omalizumab-treated individuals. Notably, omalizumab has also been found to be a steroid-sparing agent in chronic eosinophilic pneumonia, a disease characterized by bilateral pulmonary infiltrates and marked accumulation of eosinophils in bronchoalveolar lavage fluid and blood.Citation85 Thus, the effects of anti-IgE therapy on lung eosinophilia have provided further insight into the mechanisms of allergic inflammation, which may lead to improved phenotype-specific treatment.
Targeting IL-5
IL-5 plays a critical role in promoting eosinophil growth, differentiation, recruitment, and activation in tissues. Early reports demonstrated increased expression of IL-5 in bron-choalveolar lavage fluid and bronchial biopsies from patients with asthma.Citation86 Additionally, IL-5 messenger RNA (mRNA) was shown to be upregulated in the bronchial mucosa after allergen challenge, and levels correlated with disease activity.Citation87 In animal models, airway eosinophil recruitment and airway hyperresponsiveness in response to allergen challenge were reduced after anti-IL-5 treatment.Citation88 Thus, there is ample rationale for targeting IL-5 in human asthma to specifically reduce eosinophil maturation, migration, and survival, which may contribute to multiple aspects of the pathogenesis of asthma.
Mepolizumab is a humanized noncomplement-fixing monoclonal antibody (IgG1) specific for human IL-5.Citation89 Mepolizumab blocks the binding of human IL-5 to the alpha chain of the IL-5 receptor complex expressed on the eosinophil cell surface with high affinity. Anti-IL5 therapy has been shown to induce maturational arrest of bone marrow eosinophil precursors and decrease CD34+IL-5Rα+ eosinophil progenitors in the bronchial mucosa of atopic individuals.Citation90
Early studies examining mepolizumab in the treatment of asthma were somewhat disappointing because they failed to show a significant effect on airway hyperresponsiveness or a late asthmatic reaction after inhaled allergen challenge.Citation91–Citation93 These studies may have failed to show a meaningful treatment effect due to the endpoints not being closely associated with eosinophilic airway inflammation as well as the broad inclusion of a heterogeneous study population. Despite this, the early studies did show that a single dose of anti-IL5 decreased blood eosinophils for up to 16 weeks and sputum eosinophils for up to 4 weeks.Citation92 Of interest, mepolizumab appears to have a differential effect in various tissues, with nearly complete reduction in blood and sputum eosinophils, but only 55% reduction in bronchial mucosa.Citation93 Flood-Page et al postulated that varying degrees of tissue penetration, altered IL-5 receptor expression, or downregulation could be responsible for these differences.Citation93 It is also possible that once recruited into the tissue, airway eosinophils may rely on eotaxins, GM-CSF, or IL-3 for their survival.
Two recent studies suggest that there may be a beneficial effect of mepolizumab in specific groups of patients with eosinophilic asthma. In a double-blind, placebo-controlled study of 61 subjects with refractory eosinophilic asthma and a history of recurrent severe exacerbations, mepolizumab-treated patients showed a significant reduction in exacerbations, as well as improvement in symptom scores after monthly infusions of mepolizumab for one year.Citation16 A study by Nair et al enrolled asthmatic patients with persistent sputum eosinophilia despite systemic treatment with prednisone.Citation17 The authors showed that monthly intravenous mepolizumab reduced sputum and blood eosinophilia, and had a steroid-sparing effect with a substantial decrease in prednisone use in the treatment group. Anti-IL5 therapy also resulted in improved asthma control, FEV1, and quality of life. Importantly, these improvements were maintained for at least 8 weeks after the last infusion. Thus, targeting specific subsets of asthmatics with eosinophilia appears to hold the most promise for anti-IL-5 treatment.
Reslizumab, an IgG4 humanized monoclonal antibody against IL-5, has also been given to patients with poorly controlled eosinophilic asthma.Citation94 A recent study showed a significant reduction in sputum eosinophils and improvement in lung function when compared with placebo after 15 weeks of treatment with reslizumab 3 mg/kg given at monthly intervals. There was also a trend towards a decrease in exacerbations, but the study failed to show improvement in asthma control (as measured by the Asthma Control Questionnaire). The beneficial effects of reslizumab were most pronounced in a subgroup of patients with nasal polyps and in those with the highest levels of blood and sputum eosinophils. Interestingly, in addition to eosinophil levels, the presence of nasal polyposis may identify asthmatic patients who benefit the most from anti-IL-5 therapy, although studies designed to investigate this further are needed.
Lastly, benralizumab is a humanized afucosylated monoclonal antibody targeted against IL-5Rα on eosinophils and is currently in Phase II trials. An open Phase I trial in 2010 enrolled 44 subjects with mild asthma to determine safety and effective dosing.Citation95 The primary outcome was met at all doses administered with a reduction in blood eosinophil counts to nearly undetectable levels (approximately 10 cells/mL) within 24 hours. This effect persisted for at least 2–3 months in subjects dosed in the 0.03–3 mg/kg range. In a follow-up Phase II study, Laviolette et al examined the effect of a single 1 mg/kg dose of benralizumab given intravenously compared with three monthly subcutaneous doses (100 mg or 200 mg) or placebo in adults with eosinophilic asthma.Citation96 The authors demonstrated that the intravenous and subcutaneous routes led to a reduction in eosinophil counts in the airway mucosa and sputum, and nearly complete suppression of eosinophil counts in bone marrow and peripheral blood for up to 28 days after the final dose of benralizumab. Anti-IL-5 therapies undoubtedly hold promise for the treatment of eosinophilic severe asthmatics especially as both approved treatments as well as routine diagnostics to appropriately identify patients become available.
Targeting IL-4 and IL4Rα
IL-4 and IL-13 expressed by Th2 cells, mast cells, basophils, and innate lymphoid cells are key cytokines in the pathogenesis of allergic asthma and atopic disease. IL-4 is responsible for many features of asthma, including Th2 differentiation, mucus production, and B cell isotype switching. Both IL-4 and IL-13 signal through two different but overlapping heterodimeric receptors that share the alpha subunit of the IL-4 receptor (IL-4Rα).Citation97 Receptor ligation activates a common signal transducer and activator of transcription 6 (STAT-6)-mediated signaling pathway critical to development of the Th2 inflammation characteristic of asthma. Importantly, eotaxins that promote eosinophilic recruitment also depend on IL-4/IL-13 activation of STAT6. Several drugs are now under investigation targeting the IL-4/IL-13/STAT6 pathway.
The humanized IL-4 monoclonal antibody pascolizumab has been evaluated in animal studies and Phase I/II trials. In a Phase I trial, pascolizumab was well tolerated in adult patients with mild to moderate asthma; however, a subsequent large-scale Phase II trial was discontinued because it failed to show clinical effects in symptomatic patients who were steroid-naïve.Citation98 Altrakincept is a recombinant human IL-4Rα antagonist, and inhibited airway eosinophilic infiltration and mucus hypersecretion when administered during allergen challenges in a mouse model.Citation99 In a Phase I/II trial, a single inhalation of the drug improved lung function and asthma symptoms.Citation100 Pitrakinra is an antagonist targeting the IL-4/IL-13 cytokine heterodimeric receptor, composed of IL-13Rα1 and IL-4Rα subunits. When administered by the subcutaneous or inhaled route, pitrakinra inhibited allergen-induced early-phase and late-phase reactions.Citation101
Dupilumab, a humanized monoclonal antibody to the IL-4Rα subunit, was recently studied by Wenzel et al in a double-blind, placebo-controlled study.Citation102 The study enrolled 104 patients with moderate to severe persistent asthma and eosinophilia who were randomized to receive dupilumab 300 mg or placebo subcutaneously once weekly for 12 weeks. The study found a significant improvement in lung function in the treatment group, with an associated reduction in asthma exacerbations when long-acting beta-agonists and inhaled glucocorticoids were withdrawn. Additional findings included significant changes from baseline in Th2-associated biomarkers, including FeNO, chemokine ligand 17 (thymus and activation regulated chemokine), IgE, and chemokine ligand 26 (eotaxin-3) in the dupilumab group at 12 weeks. Blood and sputum eosinophil levels were no different after dupilumab treatment, although there were limited numbers of patients who provided sputum, thus precluding statistical analysis. Overall, targeting IL-4R alpha signaling (which also affects IL-13 signaling) appears to be a promising therapeutic strategy in eosinophilic asthma.
Targeting IL-13
In mouse models, IL-13 plays a critical role in eosinophil recruitment into the airway in a manner dependent on the synergistic activity of eotaxin and IL-5.Citation103 Further, several studies suggest that IL-13 may be responsible for glucocor-ticoid resistance in asthma.Citation104 Animal models using IL-13 blockade strategies have shown reductions in allergen-induced inflammation, airway hyperresponsiveness, and airway remodeling.Citation105,Citation106 Therefore, pharmaceuticals targeting this cytokine are currently under investigation in patients with steroid-refractory eosinophilic asthma. A Phase II clinical trial of anrukinzumab, a fully human IL-13 targeted antibody, carried out in mild atopic asthmatics showed a reduction in allergen-induced late asthmatic responses after subcutaneous administration of two doses (2 mg/kg) separated by 2 weeks.Citation107
A recent study evaluated lebrikizumab, a humanized anti-IL-13 monoclonal antibody, in 219 adults with inadequately controlled asthma despite inhaled corticosteroids and long-acting beta-agonists.Citation59 The study results showed improvement in FEV1 in the treatment arm after 12 weeks of therapy, with a more pronounced effect in patients with high pretreatment serum periostin levels. Interestingly, in post hoc analysis, elevated FeNO as well as high Th2 markers including peripheral eosinophilia, total IgE, chemokine ligand 13 (human monocyte chemoattractant protein-4) and chemokine ligand 17 (thymus and activation regulated chemokine) levels were also associated with a greater reduction in rates of severe exacerbations in the lebrikizumab group compared with placebo. Another anti-IL-13 antibody, tralokinumab, has also shown efficacy in improving lung function in a Phase II study of patients with moderate to severe asthma.Citation108
Other therapies
Other agents under investigation for the treatment of asthma include antagonists targeting thymic stromal lymphoprotein, IL-25, IL-33, GM-CSF, and chemokine receptor 3 expressed on eosinophils.Citation63 Neutralizing antibodies to the innate cytokines IL-25, IL-33, and thymic stromal lymphoprotein demonstrate the ability to attenuate allergic airway inflammation in mice,Citation109–Citation111 and antibodies targeting thymic stromal lymphoprotein are currently in development as intravenous therapy for patients with mild atopic asthma (ClinicalTrials.gov identifier: NCT01405963).Citation112 Additionally, inhaled antisense oligonucleotides that block the common beta chain of IL-3, IL-5, and GM-CSF receptors together with chemokine receptor 3 have shown a small overall effect in reducing the allergen-induced inflammatory response.Citation113 Further, a human monoclonal antibody targeting GM-CSF shown to decrease the survival and activation of eosinophils, is currently in Phase II trials for patients with moderate to severe asthma inadequately controlled by corticosteroids.Citation63,Citation114
Therapies targeting inflammatory lipid mediators such as prostaglandin D2, which binds to CRTH2 (chemoattractant homologous receptor expressed on Th2 cells) are also in clinical development. Several studies evaluating the ability of CRTH2 antagonists to block the chemotactic effect of prostaglandin D2 on Th2 cells and eosinophils are now underway.Citation63 Induction of eosinophilic apoptosis through the Siglec-8 (sialic acid binding Ig-like lectin 8) receptor by an activating antibody or glycan ligand-conjugated nanoparticles is also a potential therapeutic strategy under investigation.Citation115 Finally, it is worth mentioning that therapies blocking tumor necrosis factor-α, including etanercept, infliximab, and golimumab, have so far demonstrated mixed results in the treatment of asthma.Citation116,Citation117
Finally, bronchial thermoplasty, which applies thermal energy to the bronchial wall to reduce airway smooth muscle hypertrophy, has recently been studied as a potential treatment in severe asthma.Citation118 Large clinical trials have showed somewhat mixed results, with small improvements in asthma-specific quality of life measures and exacerbation rates but an overall increase in hospitalizations.Citation119 It is unclear exactly how this procedure affects the structural airways or the release of inflammatory mediators by airway smooth muscle cells, and this procedure has not been specifically evaluated in patients with eosinophilic asthma or other phenotypes.Citation120
Summary
In summary, identification of specific phenotypes of asthma with unique underlying pathophysiologic mechanisms may be particularly important for the treatment of patients with severe asthma. One proposed classification based on distinct patterns of inflammatory cell infiltrate in the airway distinguishes eosinophilic from noneosinophilic subgroups. Traditionally, airway eosinophilic infiltration has been associated with Th2-mediated allergic asthma, but there is now evidence that eosinophils are present in the airways of severe asthmatics without allergic disease. The emergence of novel biologic treatments, including monoclonal antibodies and small molecule inhibitors targeted against IgE, Th2 cytokines, and specific inflammatory mediators, has led to an enhanced understanding of the pathogenesis of asthma and highlighted the importance of patient-specific treatment. Development of noninvasive biomarkers is becoming increasingly important for subsets of asthmatic patients, including those with eosinophilic inflammation, as they may predict the response to therapy.
Acknowledgments
This research was supported by a grant from the National Institutes of Health 1K08AI080938-01A1 and the American Lung Association/American Academy of Allergy, Asthma, and Immunology Allergic Respiratory Diseases Award to TAD.
Disclosure
The authors report no conflicts of interest in this work.
References
- BatemanEDBousheyHABousquetJGOAL Inverstigators GroupCan guideline-defined asthma control be achieved? The Gaining Optimal Asthma Control studyAm J Respir Crit Care Med2004170883684415256389
- Centers for Disease Control and PreventionVital signs: asthma prevalence, disease characteristics, and self-management education: United States, 2001–2009MMWR Morb Mortal Wkly Rep2011601754755221544044
- CisternasMGBlancPDYenIHA comprehensive study of the direct and indirect costs of adult asthmaJ Allergy Clin Immunol20031111212121812789219
- WenzelSEAsthma: defining of the persistent adult phenotypesLancet200636880481316935691
- AndersonGPEndotyping asthma: new insights into key pathogenic mechanisms in a complex, heterogeneous diseaseLancet20083721107111918805339
- LotvallJAkdisCABacharierLBAsthma endotypes: a new approach to classification of disease entities within the asthma syndromeJ Allergy Clin Immunol201112735536021281866
- SimpsonJLScottRBoyleMJGibsonPGInflammatory subtypes in asthma: assessment and identification using induced sputumRespirology200611546116423202
- WenzelSESchwartzLBLangmackELEvidence that severe asthma can be divided pathologically into two inflammatory subtypes with distinct physiologic and clinical characteristicsAm J Respir Crit Care Med19991601001100810471631
- AmelinkMde GrootJCde NijsSBSevere adult-onset asthma: a distinct phenotypeJ Allergy Clin Immunol201313233634123806634
- HoustonJCDe NavasquezSTrounceJRA clinical and pathological study of fatal cases of status asthmaticusThorax1953820721313102418
- BousquetJChanezPLacosteJYEosinophilic inflammation in asthmaN Engl J Med1990323103310392215562
- JatakanonALimSBarnesPJChanges in sputum eosinophils predict loss of asthma controlAm J Respir Crit Care Med2000161647210619799
- DeykinALazarusSCFahyJVSputum eosinophil counts predict asthma control after discontinuation of inhaled corticosteroidsJ Allergy Clin Immunol200511572072715805990
- MeijerRJPostmaDSKauffmanHFArendsLRKoeterGHKerstjensHAAccuracy of eosinophils and eosinophil cationic protein to predict steroid improvement in asthmaClin Exp Allergy2002321096110312100060
- BerryMMorganAShawDEPathological features and inhaled corticosteroid response of eosinophilic and non-eosinophilic asthmaThorax2007621043104917356056
- HaldarPBrightlingCEHargadonBMepolizumab and exacerbations of refractory eosinophilic asthmaN Engl J Med200936097398419264686
- NairPPizzichiniMMKjarsgaardMMepolizumab for prednisone-dependent asthma with sputum eosinophiliaN Engl J Med200936098599319264687
- HamidQTulicMImmunobiology of asthmaAnnu Rev Physiol20097148950719575684
- BarrettNAAustenKFInnate cells and T helper 2 cell immunity in airway inflammationImmunity20093142543719766085
- DohertyTBroideDCytokines and growth factors in airway remodeling in asthmaCurr Opin Immunol20071967668017720466
- GartyBZKosmanEGanorEEmergency room visits of asthmatic children, relation to air pollution, weather, and airborne allergensAnn Allergy Asthma Immunol1998815635709892028
- D’AmatoGCecchiLLiccardiGThunderstorm-related asthma: not only grass pollen and sporesJ Allergy Clin Immunol200812153753818155276
- HolgateSTInnate and adaptive immune responses in asthmaNat Med20121867368322561831
- LeeHCHeadleyMBLooYMThymic stromal lymphopoietin is induced by respiratory syncytial virus-infected airway epithelial cells and promotes a type 2 response to infectionJ Allergy Clin Immunol201213011871196. e522981788
- ZieglerSFThymic stromal lymphopoietin and allergic diseaseJ Allergy Clin Immunol201213084585222939755
- BarnesPJThe cytokine network in asthma and chronic obstructive pulmonary diseaseJ Clin Invest20081183546355618982161
- WardlawAJBrightlingCGreenRWoltmannGPavordIEosinophils in asthma and other allergic diseasesBr Med Bull200056985100311359633
- CollinsPDMarleauSGriffiths-JohnsonDAJosePJWilliamsTJCooperation between interleukin-5 and the chemokine eotaxin to induce eosinophil accumulation in vivoJ Exp Med1995182116911747561691
- ZietkowskiZTomasiakMMSkiepkoRBodzenta-LukaszykARANTES in exhaled breath condensate of stable and unstable asthma patientsRespir Med20081021198120218603420
- BroideDHPaineMMFiresteinGSEosinophils express interleukin 5 and granulocyte macrophage-colony-stimulating factor mRNA at sites of allergic inflammation in asthmaticsJ Clin Invest199290141414241401075
- BroideDHFiresteinGSEndobronchial allergen challenge in asthma. Demonstration of cellular source of granulocyte macrophage colony-stimulating factor by in situ hybridizationJ Clin Invest199188104810531885766
- DaviesDLarbiKAllenAVCAM-1 contributes to rapid eosinophil accumulation induced by the chemoattractants PAF and LTB4: evidence for basal expression of functional VCAM-1 in rat skinImmunology19999715015810447726
- StirlingRGvan RensenELBarnesPJChungKFInterleukin-5 induces CD34(+) eosinophil progenitor mobilization and eosinophil CCR3 expression in asthmaAm J Respir Crit Care Med20011641403140911704586
- ChoJYMillerMBaekKJInhibition of airway remodeling in IL-5-deficient miceJ Clin Invest200411355156014966564
- FahyJVEosinophilic and neutrophilic inflammation in asthma: insights from clinical studiesProc Am Thorac Soc2009625625919387026
- GreenRHBrightlingCEMcKennaSAsthma exacerbations and sputum eosinophil counts: a randomised controlled trialLancet20023601715172112480423
- WoodruffPGKhashayarRLazarusSCRelationship between airway inflammation, hyperresponsiveness, and obstruction in asthmaJ Allergy Clin Immunol200110875375811692100
- LouisRLauLCBronAORoldaanACRadermeckerMDjukanovicRThe relationship between airways inflammation and asthma severityAm J Respir Crit Care Med200016191610619791
- PorsbjergCLundTKPedersenLBackerVInflammatory subtypes in asthma are related to airway hyperresponsiveness to mannitol and exhaled NOJ Asthma20094660661219657904
- CrimiESpanevelloANeriMIndPWRossiGABrusascoVDissociation between airway inflammation and airway hyperresponsiveness in allergic asthmaAm J Respir Crit Care Med1998157499445270
- MirandaCBusackerABalzarSTrudeauJWenzelSEDistinguishing severe asthma phenotypes: role of age at onset and eosinophilic inflammationJ Allergy Clin Immunol200411310110814713914
- ten BrinkeAZwindermanAHSterkPJRabeKFBelEH“Refractory” eosinophilic airway inflammation in severe asthma: effect of parenteral corticosteroidsAm J Respir Crit Care Med200417060160515215154
- ThomsonNCChaudhuriRWhy is eosinophilic bronchitis not asthma?Am J Respir Crit Care Med20041704515220118
- BrightlingCEBraddingPSymonFAHolgateSTWardlawAJPavordIDMast-cell infiltration of airway smooth muscle in asthmaN Engl J Med20023461699170512037149
- KanazawaHNomuraSYoshikawaJRole of microvascular permeability on physiologic differences in asthma and eosinophilic bronchitisAm J Respir Crit Care Med20041691125113015044203
- FrickWESedgwickJBBusseWWThe appearance of hypodense eosinophils in antigen-dependent late phase asthmaAm Rev Respir Dis1989139140114062729749
- UlrikCSPeripheral eosinophil counts as a marker of disease activity in intrinsic and extrinsic asthmaClin Exp Allergy1995258208278564720
- HastieATMooreWCLiHBiomarker surrogates do not accurately predict sputum eosinophil and neutrophil percentages in asthmatic subjectsJ Allergy Clin Immunol2013132728023706399
- D’SilvaLCookRJAllenCJHargreaveFEParameswaranKChanging pattern of sputum cell counts during successive exacerbations of airway diseaseRespir Med20071012217222017606366
- GoodJTJrKolakowskiCAGroshongSDMurphyJRMartinRJRefractory asthma: importance of bronchoscopy to identify phenotypes and direct therapyChest201114159960621835905
- SilkoffPELentAMBusackerAAExhaled nitric oxide identifies the persistent eosinophilic phenotype in severe refractory asthmaJ Allergy Clin Immunol20051161249125516337453
- MahrTAMalkaJSpahnJDInflammometry in pediatric asthma: a review of fractional exhaled nitric oxide in clinical practiceAllergy Asthma Proc20133421021923462278
- BarnesPJDweikRAGelbAFExhaled nitric oxide in pulmonary diseases: a comprehensive reviewChest201013868269220822990
- SmithADCowanJOBrassettKPHerbisonGPTaylorDRUse of exhaled nitric oxide measurements to guide treatment in chronic asthmaN Engl J Med20053522163217315914548
- TseliouEBessaVHillasGExhaled nitric oxide and exhaled breath condensate pH in severe refractory asthmaChest201013810711320173051
- BlanchardCMinglerMKMcBrideMPeriostin facilitates eosinophil tissue infiltration in allergic lung and esophageal responsesMucosal Immunol2008128929619079190
- OuyangGLiuMRuanKSongGMaoYBaoSUpregulated expression of periostin by hypoxia in non-small-cell lung cancer cells promotes cell survival via the Akt/PKB pathwayCancer Lett200928121321919328625
- JiaGEricksonRWChoyDFPeriostin is a systemic biomarker of eosinophilic airway inflammation in asthmatic patientsJ Allergy Clin Immunol2012130647654. e1022857879
- CorrenJLemanskeRFHananiaNALebrikizumab treatment in adults with asthmaN Engl J Med20113651088109821812663
- MasuokaMShiraishiHOhtaSPeriostin promotes chronic allergic inflammation in response to Th2 cytokinesJ Clin Invest20121222590260022684102
- GordonEDSidhuSSWangZEA protective role for periostin and TGF-beta in IgE-mediated allergy and airway hyperresponsivenessClin Exp Allergy20124214415522093101
- KulkarniNSHollinsFSutcliffeAEosinophil protein in airway macrophages: a novel biomarker of eosinophilic inflammation in patients with asthmaJ Allergy Clin Immunol20101266169. e320639010
- BarnesPJSevere asthma: advances in current management and future therapyJ Allergy Clin Immunol2012129485922196524
- IrusenEMatthewsJGTakahashiABarnesPJChungKFAdcockIMp38 Mitogen-activated protein kinase-induced glucocorticoid receptor phosphorylation reduces its activity: role in steroid-insensitive asthmaJ Allergy Clin Immunol200210964965711941315
- ManeechotesuwanKXinYItoKRegulation of Th2 cytokine genes by p38 MAPK-mediated phosphorylation of GATA-3J Immunol20071782491249817277157
- CuendaARousseauSp38 MAP-kinases pathway regulation, function and role in human diseasesBiochim Biophys Acta200717731358137517481747
- BarnesPJAdcockIMGlucocorticoid resistance in inflammatory diseasesLancet20093731905191719482216
- MizueYGhaniSLengLRole for macrophage migration inhibitory factor in asthmaProc Natl Acad Sci U S A2005102144101441516186482
- PelaiaGVatrellaAMaselliRThe potential of biologics for the treatment of asthmaNat Rev Drug Discov20121195897223197041
- SainiSSMacGlashanDWJrSterbinskySADown-regulation of human basophil IgE and FC epsilon RI alpha surface densities and mediator release by anti-IgE-infusions is reversible in vitro and in vivoJ Immunol19991625624563010228046
- HumbertMBeasleyRAyresJBenefits of omalizumab as add-on therapy in patients with severe persistent asthma who are inadequately controlled despite best available therapy (GINA 2002 step 4 treatment): INNOVATEAllergy20056030931615679715
- AyresJGHigginsBChilversERAyreGBloggMFoxHEfficacy and tolerability of anti-immunoglobulin E therapy with omalizumab in patients with poorly controlled (moderate-to-severe) allergic asthmaAllergy20045970170815180756
- VignolaAMHumbertMBousquetJEfficacy and tolerability of anti-immunoglobulin E therapy with omalizumab in patients with concomitant allergic asthma and persistent allergic rhinitis: SOLARAllergy20045970971715180757
- BusseWCorrenJLanierBQOmalizumab, anti-IgE recombinant humanized monoclonal antibody, for the treatment of severe allergic asthmaJ Allergy Clin Immunol200110818419011496232
- SolerMMatzJTownleyRThe anti-IgE antibody omalizumab reduces exacerbations and steroid requirement in allergic asthmaticsEur Respir J20011825426111529281
- LanierBQCorrenJLumryWLiuJFowler-TaylorAGuptaNOmalizumab is effective in the long-term control of severe allergic asthmaAnn Allergy Asthma Immunol20039115415912952109
- HolgateSTChuchalinAGHebertJEfficacy and safety of a recombinant anti-immunoglobulin E antibody (omalizumab) in severe allergic asthmaClin Exp Allergy20043463263815080818
- BousquetJRabeKHumbertMPredicting and evaluating response to omalizumab in patients with severe allergic asthmaRespir Med20071011483149217339107
- NogaOHanfGBrachmannIEffect of omalizumab treatment on peripheral eosinophil and T-lymphocyte function in patients with allergic asthmaJ Allergy Clin Immunol20061171493149916751018
- DjukanovicRWilsonSJKraftMEffects of treatment with anti-immunoglobulin E antibody omalizumab on airway inflammation in allergic asthmaAm J Respir Crit Care Med200417058359315172898
- NogaOHanfGKunkelGImmunological and clinical changes in allergic asthmatics following treatment with omalizumabInt Arch Allergy Immunol2003131465212759489
- MilgromHFickRBJrSuJQTreatment of allergic asthma with monoclonal anti-IgE antibody. rhuMAb-E25 Study GroupN Engl J Med19993411966197310607813
- HolgateSCasaleTWenzelSBousquetJDenizYReisnerCThe anti-inflammatory effects of omalizumab confirm the central role of IgE in allergic inflammationJ Allergy Clin Immunol200511545946515753888
- ChandHSSchuylerMJosteNAnti-IgE therapy results in decreased myeloid dendritic cells in asthmatic airwaysJ Allergy Clin Immunol201012511571158. e520304471
- KayaHGumusSUcarEOmalizumab as a steroid-sparing agent in chronic eosinophilic pneumoniaChest201214251351622871762
- HamidQAzzawiMYingSExpression of mRNA for interleukin-5 in mucosal bronchial biopsies from asthmaJ Clin Invest199187154115462022726
- HumbertMCorriganCJKimmittPTillSJKayABDurhamSRRelationship between IL-4 and IL-5 mRNA expression and disease severity in atopic asthmaAm J Respir Crit Care Med19971567047089309982
- GarlisiCGKungTTWangPEffects of chronic anti-interleukin-5 monoclonal antibody treatment in a murine model of pulmonary inflammationAm J Respir Cell Mol Biol1999202482559922215
- GnanakumaranGBabuKSTechnology evaluation: mepolizumab, GlaxoSmithKlineCurr Opin Mol Ther2003532132512870444
- Menzies-GowAFlood-PagePSehmiRAnti-IL-5 (mepolizumab) therapy induces bone marrow eosinophil maturational arrest and decreases eosinophil progenitors in the bronchial mucosa of atopic asthmaticsJ Allergy Clin Immunol200311171471912704348
- KipsJCO’ConnorBJLangleySJEffect of SCH55700, a humanized anti-human interleukin-5 antibody, in severe persistent asthma: a pilot studyAm J Respir Crit Care Med20031671655165912649124
- LeckieMJten BrinkeAKhanJEffects of an interleukin-5 blocking monoclonal antibody on eosinophils, airway hyper-responsiveness, and the late asthmatic responseLancet20003562144214811191542
- Flood-PagePSwensonCFaifermanIA study to evaluate safety and efficacy of mepolizumab in patients with moderate persistent asthmaAm J Respir Crit Care Med20071761062107117872493
- CastroMMathurSHargreaveFReslizumab for poorly controlled, eosinophilic asthma: a randomized, placebo-controlled studyAm J Respir Crit Care Med20111841125113221852542
- BusseWWKatialRGossageDSafety profile, pharmacokinetics, and biologic activity of MEDI-563, an anti-IL-5 receptor alpha antibody, in a phase I study of subjects with mild asthmaJ Allergy Clin Immunol201012512371244. e220513521
- LavioletteMGossageDLGauvreauGEffects of benralizumab on airway eosinophils in asthmatic patients with sputum eosinophiliaJ Allergy Clin Immunol201313210861096. e523866823
- IngramJLKraftMIL-13 in asthma and allergic disease: asthma phenotypes and targeted therapiesJ Allergy Clin Immunol201213082984222951057
- HartTKBlackburnMNBrigham-BurkeMPreclinical efficacy and safety of pascolizumab (SB 240683): a humanized anti-interleukin-4 antibody with therapeutic potential in asthmaClin Exp Immunol20021309310012296858
- HendersonWRJrChiEYMaliszewskiCRSoluble IL-4 receptor inhibits airway inflammation following allergen challenge in a mouse model of asthmaJ Immunol20001641086109510623860
- BorishLCNelsonHSCorrenJEfficacy of soluble IL-4 receptor for the treatment of adults with asthmaJ Allergy Clin Immunol200110796397011398072
- WenzelSWilbrahamDFullerRGetzEBLongphreMEffect of an interleukin-4 variant on late phase asthmatic response to allergen challenge in asthmatic patients: results of two phase 2a studiesLancet20073701422143117950857
- WenzelSFordLPearlmanDDupilumab in persistent asthma with elevated eosinophil levelsN Engl J Med20133682455246623688323
- PopeSMBrandtEBMishraAIL-13 induces eosinophil recruitment into the lung by an IL-5- and eotaxin-dependent mechanismJ Allergy Clin Immunol200110859460111590387
- SpahnJDSzeflerSJSursWDohertyDENimmagaddaSRLeungDYA novel action of IL-13: induction of diminished monocyte glucocorticoid receptor-binding affinityJ Immunol1996157265426598805670
- YangGVolkAPetleyTAnti-IL-13 monoclonal antibody inhibits airway hyperresponsiveness, inflammation and airway remodelingCytokine20042822423215566951
- BreeASchlermanFJWadanoliMIL-13 blockade reduces lung inflammation after Ascaris suum challenge in cynomolgus monkeysJ Allergy Clin Immunol20071191251125717379289
- GauvreauGMBouletLPCockcroftDWEffects of interleukin-13 blockade on allergen-induced airway responses in mild atopic asthmaAm J Respir Crit Care Med20111831007101421057005
- PiperEBrightlingCNivenRA phase II placebo-controlled study of tralokinumab in moderate-to-severe asthmaEur Respir J20134133033822743678
- TamachiTMaezawaYIkedaKIL-25 enhances allergic airway inflammation by amplifying a TH2 cell-dependent pathway in miceJ Allergy Clin Immunol200611860661416950278
- FujitaJKawaguchiMKokubuFInterleukin-33 induces interleukin-17F in bronchial epithelial cellsAllergy20126774475022540331
- ShiLLeuSWXuFLocal blockade of TSLP receptor alleviated allergic disease by regulating airway dendritic cellsClin Immunol200812920221018757241
- AmgenDouble-blind, Multiple Dose Study in Subjects With Mild Atopic Asthma Available from: http://clinicaltrials.gov/show/NCT01405963. NLM identifier: NCT01405963Accessed February 3, 2014
- GauvreauGMBouletLPCockcroftDWAntisense therapy against CCR3 and the common beta chain attenuates allergen-induced eosinophilic responsesAm J Respir Crit Care Med200817795295818244953
- KrinnerEMRaumTPetschSA human monoclonal IgG1 potently neutralizing the pro-inflammatory cytokine GM-CSFMol Immunol20074491692516697465
- KiwamotoTKawasakiNPaulsonJCBochnerBSSiglec-8 as a drugable target to treat eosinophil and mast cell-associated conditionsPharmacol Ther201213532733622749793
- WenzelSEBarnesPJBleeckerERA randomized, double-blind, placebo-controlled study of tumor necrosis factor-alpha blockade in severe persistent asthmaAm J Respir Crit Care Med200917954955819136369
- HolgateSTNoonanMChanezPEfficacy and safety of etanercept in moderate-to-severe asthma: a randomised, controlled trialEur Respir J2011371352135921109557
- CastroMMusaniAIMayseMLShargillNSBronchial thermoplasty: a novel technique in the treatment of severe asthmaTher Adv Respir Dis2010410111620435668
- CastroMRubinASLavioletteMEffectiveness and safety of bronchial thermoplasty in the treatment of severe asthma: a multicenter, randomized, double-blind, sham-controlled clinical trialAm J Respir Crit Care Med201218111612419815809
- ThomsonNCRubinASNivenRMLong-term (5 year) safety of bronchial thermoplasty: Asthma Intervention Research (AIR) trialBMC Pulm Med201111821314924