
Abstract
Acute and chronic cough are common symptoms in patients with severe allergic asthma. Although asthma-related cough can be controlled by asthma-specific medications, both prescription and over-the-counter antitussives are often also necessary. The anti-immunoglobulin E monoclonal antibody omalizumab is an effective treatment for patients with moderate-to-severe asthma, but little is known about subsequent antitussive use patterns. This post hoc analysis examined data from the Phase 3 EXTRA study that included patients aged 12–75 years with inadequately controlled moderate-to-severe asthma. Baseline antitussive use was low overall (16/427, 3.7% for omalizumab and 18/421, 4.3% for placebo). Among patients with no baseline antitussive use (n = 411 omalizumab, n = 403 placebo), most patients (88.3% omalizumab, 83.4% placebo) reported not using antitussives during the 48-week treatment period. The percentage of patients using 1 antitussive was lower for patients treated with omalizumab than placebo (7.1% vs 13.2%), although the adjusted rate of antitussive use during the treatment period was similar for omalizumab and placebo (0.22 and 0.25). Non-narcotics were used more often than narcotics. In conclusion, this analysis found low use of antitussives in patients with severe asthma and suggests that omalizumab may have the potential to decrease antitussive use.
Keywords:
Introduction
Acute and chronic cough are common symptoms in patients with severe allergic asthma, and cough a significant contributor to overall symptom burden.Citation1 Asthma-related cough can be controlled by standard asthma medications, such as inhaled corticosteroids (ICS), leukotriene receptor agonists, beta-antagonists,Citation2 and tiotropium.Citation3 However, both prescription and over-the-counter antitussives are also commonly used to control cough, especially during asthma exacerbations.Citation4 Omalizumab, an anti-immunoglobulin E (IgE) monoclonal antibody, is an effective treatment for patients with moderate-to-severe allergic asthma and reduces the use of maintenance asthma medications and rescue medications.Citation5–7 But there are limited data on whether omalizumab, or any other biologic, has an impact on cough in patients with asthma. The objective of this analysis was to assess whether omalizumab affects subsequent use of antitussives in patients with inadequately controlled moderate-to-severe asthma.
Methods
Study Design
This post hoc analysis examined data from EXTRA, a prospective, randomized controlled Phase 3 clinical trial (ClinicalTrials.gov identifier: NCT00314574). This study was conducted according to US Food and Drug Administration regulations, the International Conference on Harmonization E6 Guidelines for Good Clinical Practice, and other national requirements. All sites obtained institutional review board approval to conduct this study and obtained signed informed consent from study participants before enrollment (Ethics Committees are listed in Supplementary Table 1). The design and results of the EXTRA study have been described in detail previously.Citation6 Patients (aged 12–75 years) with inadequately controlled moderate-to-severe allergic asthma who were receiving high-dose ICS (defined as a minimum dose of 500 mcg of fluticasone dry-powder inhaler twice daily or its ex-valve metered dose) and long-acting beta-2 agonists (either salmeterol 50 mcg twice daily or formoterol 12 mcg twice daily) for at least 8 weeks before screening with or without additional controller therapy were randomized 1:1 to additional placebo or omalizumab treatment for 48 weeks. Concomitant medications, including the use of antitussives, were recorded throughout the study.
Analysis
This post hoc analysis assessed the use of antitussives during the treatment period for all patients who were randomized and received ≥1 dose of study drug (n = 427 omalizumab, n = 421 placebo) and for a sub-group of patients with no baseline antitussive use (n = 411 omalizumab, n = 403 placebo). Antitussives were selected from the list of concomitant medications taken by study participants (see Supplementary Table 2), with a primary indication of cough symptom relief and not generally used to treat other conditions (such as allergic rhinitis or sinus congestion), and were defined as (i) over-the-counter or prescription medications and (ii) narcotic or non-narcotic. For analysis, if >1 antitussive was used at the same time, this was considered a single event and antitussives taken at baseline were excluded. Rate of antitussive use during treatment period was analyzed using Poisson regression with adjustment for antitussives at baseline, asthma controller use at baseline, and dosing regimen, normalized by patient-treatment period (ie, how long patients were treated for, which helps ensure the rates are comparable).
Results
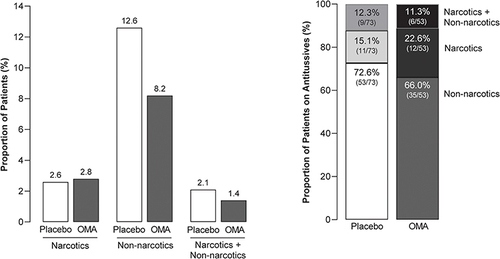
As reported in Hanania et al, baseline demographics and clinical characteristics were generally similar across treatment groups.Citation6 At baseline, antitussive use was low overall and for each treatment group (16/427, 3.7% for omalizumab and 18/421, 4.3% for placebo), and non-narcotics were used more often than narcotics (non-narcotics - placebo, 16/421, 3.8%; omalizumab, 14/427, 3.3%: narcotics - placebo, 2/421, 0.5%; omalizumab, 2/427, 0.5%). Among patients with no baseline antitussive use, >80% of patients reported not using antitussives during the 48-week treatment period (). The percentage of patients using 1 antitussive was lower for patients treated with omalizumab (29/411, 7.1%) than placebo (53/403, 13.2%). Antitussive use during the treatment period was similar for all patients who were randomized and received ≥1 dose of study drug (data not shown). The adjusted rate of antitussive use during the treatment period was similar for placebo vs omalizumab (). Non-narcotic–based antitussives were more commonly used than narcotics ().
Table 1 Antitussive Use in Patients with Severe Asthma During the Treatment Period: Patients with No Antitussive Use at Baseline
Figure 1 Type of Antitussives Used During the Treatment Period.
Overall safety results for EXTRA were previously reported; the incidence of adverse events was similar between treatment groups.Citation6
Discussion
This report of antitussive use in patients with moderate-to-severe asthma found that antitussive use was low overall both at baseline and during the treatment period in both placebo- and omalizumab-treated patients in the EXTRA trial. In addition, antitussive use was lower in omalizumab- vs placebo-treated patients at 48 weeks. We hypothesize that decreased antitussive use may indicate decreased cough and reflect reduced asthma exacerbations in the patient (as previously suggestedCitation8), potentially translating to improved asthma control and cough-related quality of life.
Notably, cough is not routinely captured in commonly used tools that measure asthma control and is not typically considered as an outcome variable in clinical trials, and most studies of cough in asthma have been confined to patients with mild disease or cough-variant asthma.Citation9 Indeed, the characteristics and clinical impact of cough in asthma are poorly understood. This is despite evidence that cough has been associated with asthma controlCitation1 and may be related to comorbidities, including allergic rhinitis, nasal polyps, and gastro-esophageal reflux.Citation10,Citation11 Further, chronic cough is associated with poor quality of life, loss of sleep, and impaired social, physical, and psychological well-being.Citation12
There are several limitations of this analysis. The exploratory post hoc nature limits interpretation; the assessment of antitussive use was limited to reports of concomitant medication (because it was not a prespecified outcome of EXTRA); and an objective, subjective, or patient-reported measure of cough (such as those considered by Turner et alCitation13) was not assessed. In addition, though expected to be uncommon in a clinical trial, there is a possibility of non-reported self-medication of antitussives. Finally, given that EXTRA was a clinical trial, antitussive use may be lower than that reported in the real world (4% versus 27% in a survey of regular pharmacy customers with asthma).Citation4
In conclusion, this exploratory analysis found low overall use of antitussives in patients with moderate-to-severe asthma and suggests that omalizumab may have the potential to decrease antitussive use. Although antitussives in general have both benefits (including amelioration of parental concerns for pediatric patients with cough, reducing the risk of a cough-induced cough cycle, and improving quality of life) and risks (lack of evidence of efficacy, adverse events, abuse potential),Citation14,Citation15 given potential concerns over the excessive use of antitussives for asthma-related cough, a reduction in antitussive use may be a valuable outcome measure and may lead to real-world benefits for patients for asthma.
Abbreviation
ICS, inhaled corticosteroids.
Data Sharing Statement
Qualified researchers may request access to individual patient-level data through the clinical study data request platform (https://vivli.org/). Further details on Roche’s criteria for eligible studies are available here (https://vivli.org/members/ourmembers/). For further details on Roche’s Global Policy on the Sharing of Clinical Information and how to request access to related clinical study documents, see here (https://www.roche.com/research_and_development/who_we_are_how_we_work/clinical_trials/our_commitment_to_data_sharing.htm).
Disclosure
CJR is an owner of Medicine Deconstructed Productions and reports personal fees from Sanofi, Regeneron, Boehringer Ingelheim, United Therapeutics, Amgen, AstraZeneca, Olympus, Moderna, and Pfizer, outside the submitted work. OII is a consultant for Blueprint Medicines and Novartis and reports grants from NIH NIAID K08AI141691, grants from 2020 American Association of Allergy, Asthma, and Immunology Foundation Faculty Development Award, outside the submitted work. KA, JK, PM and SG are employees of Genentech, Inc. SG is a shareholder of Genentech, Inc. AM has no conflicts of interest to declare.
Acknowledgments
Medical writing assistance was provided by Janelle Keys, PhD, CMPP of Envision Pharma Group, and funded by Genentech, Inc., a member of the Roche Group. Envision Pharma Group’s services complied with international guidelines for Good Publication Practice (GPP 2022).
This paper was presented at the American Thoracic Society Annual Meeting, May 13-18, 2022, in San Francisco, CA, USA, as a poster presentation with interim findings.
Additional information
Funding
References
- Holmes J, McGarvey LP, Birring SS, Fletcher H, Heaney LG. An observational study to determine the relationship between cough frequency and markers of inflammation in severe asthma. Eur Respir J. 2022;60(6):2103205. doi:10.1183/13993003.03205-2021
- Côté A, Russell RJ, Boulet LP, et al. Managing chronic cough due to asthma and NAEB in adults and adolescents: CHEST guideline and expert panel report. Chest. 2020;158(1):68–96. doi:10.1016/j.chest.2019.12.021
- Fukumitsu K, Kanemitsu Y, Asano T, et al. Tiotropium attenuates refractory cough and capsaicin cough reflex sensitivity in patients with asthma. J Allergy Clin Immunol Pract. 2018;6(5):1613–1620.e1612. doi:10.1016/j.jaip.2018.01.016
- Laforest L, Van Ganse E, Devouassoux G, et al. Dispensing of antibiotics, antitussives and mucolytics to asthma patients: a pharmacy-based observational survey. Respir Med. 2008;102(1):57–63. doi:10.1016/j.rmed.2007.08.004
- Busse W, Corren J, Lanier BQ, et al. Omalizumab, anti-IgE recombinant humanized monoclonal antibody, for the treatment of severe allergic asthma. J Allergy Clin Immunol. 2001;108(2):184–190. doi:10.1067/mai.2001.117880
- Hanania NA, Alpan O, Hamilos DL, et al. Omalizumab in severe allergic asthma inadequately controlled with standard therapy: a randomized trial. Ann Intern Med. 2011;154(9):573–582. doi:10.7326/0003-4819-154-9-201105030-00002
- MacDonald KM, Kavati A, Ortiz B, Alhossan A, Lee CS, Abraham I. Short- and long-term real-world effectiveness of omalizumab in severe allergic asthma: systematic review of 42 studies published 2008-2018. Expert Rev Clin Immunol. 2019;15(5):553–569. doi:10.1080/1744666X.2019.1574571
- Van Ganse E, Van der Linden P, Leufkens HG, Vincken W, Ernst P. Antiallergic and antitussive medications: extent of use and relationship to asthma exacerbations. Therapie. 1996;51(4):373–377.
- Holmes J, Heaney LG, McGarvey LPA. Objective and subjective measurement of cough in asthma: a systematic review of the literature. Lung. 2022;200(2):169–178. doi:10.1007/s00408-022-00527-0
- Diab N, Patel M, O’Byrne P, Satia I. Narrative review of the mechanisms and treatment of cough in asthma, cough variant asthma, and non-asthmatic eosinophilic bronchitis. Lung. 2022;200(6):707–716. doi:10.1007/s00408-022-00575-6
- Watelet JB, Van Zele T, Brusselle G. Chronic cough in upper airway diseases. Respir Med. 2010;104(5):652–657. doi:10.1016/j.rmed.2009.11.020
- Prenner B, Topp R, Beltyukova S, Fox C. Referrals, etiology, prevalence, symptoms, and treatments of chronic cough: a survey of allergy specialists. Ann Allergy Asthma Immunol. 2022;129(6):731–736. doi:10.1016/j.anai.2022.08.993
- Turner RD, Birring SS. Measuring cough: what really matters? J Thorac Dis. 2023;15(4):2288–2299. doi:10.21037/jtd-23-230
- Lam SHF, Homme J, Avarello J, et al. Use of antitussive medications in acute cough in young children. J Am Coll Emerg Physicians Open. 2021;2(3):e12467. doi:10.1002/emp2.12467
- De Blasio F, Virchow JC, Polverino M, et al. Cough management: a practical approach. Cough. 2011;7(1):7. doi:10.1186/1745-9974-7-7