
Abstract
Purpose
Oral corticosteroid (OCS) use for asthma is associated with considerable healthcare resource utilization (HCRU) and costs. However, no study has investigated this in relation to patterns of intermittent OCS prescription.
Methods
This historical UK cohort study used primary care medical records, linked to Hospital Episode Statistics, from 2008 to 2019, of patients (≥4 years old) with asthma prescribed intermittent OCS. Patients were categorized by OCS prescribing pattern (one-off [single], less frequent [≥90-day gap] and frequent [<90-day gap]) and matched 1:1 (by sex, age and index date) with people never prescribed OCS with/without asthma. HCRU (reported as episodes, except for length of hospital stay [days] and any prescription [records]) and associated costs were compared between intermittent OCS and non-OCS cohorts, and among intermittent OCS prescribing patterns.
Results
Of 149,191 eligible patients, 50.3% had one-off, 27.4% less frequent, and 22.3% frequent intermittent OCS prescribing patterns. Annualized non-respiratory HCRU rates were greater in the intermittent OCS versus non-OCS cohorts for GP visits (5.93 vs 4.70 episodes, p < 0.0001), hospital admissions (0.24 vs 0.16 episodes, p < 0.0001), and length of stay (1.87 vs 1.58 days, p < 0.0001). In the intermittent OCS cohort, rates were highest in the frequent prescribing group for GP visits (7.49 episodes; p < 0.0001 vs one-off), length of stay (2.15 days; p < 0.0001) and any prescription including OCS (25.22 prescriptions; p < 0.0001). Mean per-patient non-respiratory related and all-cause HCRU-related costs were higher with intermittent OCS than no OCS (£3902 vs £2722 and £8623 vs £4929, respectively), as were mean annualized costs (£565 vs £313 and £1526 vs £634, respectively). A dose–response relationship existed; HCRU-related costs were highest in the frequent prescribing cohort (p < 0.0001).
Conclusion
Intermittent OCS use and more frequent intermittent OCS prescription patterns were associated with increased HCRU and associated costs. Improved asthma management is needed to reduce reliance on intermittent OCS in primary care.
Introduction
Oral corticosteroids (OCS) are recommended by major treatment guidelines and recommendations, such as those from the Global Initiative for Asthma (GINA), for the management of asthma exacerbations.Citation1 Use of OCS, including short-term or periodic (<5 mg/day/year) for the management of asthma is associated with an increased risk of short- and long-term adverse outcomes and premature death, compared with non-use of OCS.Citation2–4 We previously demonstrated that this association is consistent across age, asthma severity (GINA treatment step) and prior inhaled corticosteroid (ICS) maintenance or short-acting β2-agonist (SABA) reliever use.Citation5 Our data also showed an association between one-off use of OCS and a significantly increased risk of OCS-related adverse outcomes versus non-OCS use.Citation5
Despite this increased risk for adverse outcomes, the limited use recommended by guidelines, and the availability of novel therapies for the chronic treatment of asthma, recent data suggest that OCS are still widely used for the management of asthma.Citation6 For example, a systematic review found that around one-quarter of patients with asthma of any severity required short-term OCS during a 1-year period,Citation7 while data from the International Severe Asthma Registry revealed that nearly one-half of patients treated at GINA Step 5 were receiving long-term OCS.Citation8 Furthermore, the use of OCS has been shown to result in a considerable healthcare burden. In the US, the individual incremental annual costs of systemic corticosteroid (SCS)-related complications were $2670, $4639 and $9162 (2014 US $) over a 1.5-year median follow-up period in patients with asthma receiving long-term low- (<5 mg/day), medium- (≥5–10 mg/day) or high-dose (>10 mg/day) corticosteroids, respectively, versus patients with asthma who had no SCS exposure.Citation9 In the UK, over an average of 8.6 years, patients with asthma receiving SCS had more frequent all-cause (excluding asthma-related) general practitioner (GP) and specialist visits, hospital admissions, emergency department visits and healthcare resource utilization (HCRU)-related costs versus patients with asthma who had no SCS exposure.Citation10
To our knowledge, no studies have investigated the association between different OCS prescribing patterns with OCS-related HCRU and costs, exclusively in patients with asthma and intermittent OCS use. In this study, we describe non-respiratory, all-cause, and OCS-related HCRU and costs, and examine associations with intermittent OCS prescribing patterns in primary care patients with asthma receiving intermittent OCS compared with matched primary care patients who had never received OCS.
Materials and Methods
Study Design and Cohorts
This was an historical, observational UK cohort study (registered at the European Network of Centres for Pharmacoepidemiology and Pharmacovigilance [ENCePP]; number EUPAS37065) of available data from 2008 to March 2019 (from 2008, the data were accredited by the UK Office for National Statistics, and 2019 was used as the cut-off to avoid effects of the COVID-19 pandemic). Detailed study design and patient inclusion and exclusion criteria have been reported previously.Citation5,Citation11
Patients with asthma aged ≥4 years old who received intermittent OCS prescriptions and who had a minimum of 12 months of clinical data prior to index date were included in the OCS cohort. The index date for the intermittent OCS cohort was the date of first OCS prescription within 3 months of an asthma event (prescription for asthma medication, asthma consultation and/or asthma diagnosis). To ensure the OCS cohort only included patients who received intermittent OCS prescriptions, a previously defined algorithm was used to exclude patients who were receiving or suspected of receiving long-term OCS prescriptions at any time during the study.Citation11 The control cohort was composed of individuals with or without asthma who had no exposure to OCS (the “non-OCS” cohort) at any time; including people without asthma was necessary since forming a control group exclusively from asthma patients who had never received OCS was infeasible due to insufficient numbers. Thereafter, participants in the control arm were matched to the intermittent OCS cohort in a 1:1 ratio based on sex, age and index date (the date of a GP visit nearest to the index date of the matched intermittent OCS patient). Individuals were excluded from the intermittent OCS and non-OCS cohorts if they ever had a diagnosis for a chronic condition other than asthma that was commonly treated with OCS (ankylosing spondylitis, Sjogren’s syndrome, systemic lupus erythematosus, temporal arteritis, ulcerative colitis, psoriatic arthritis, multiple sclerosis, polymyalgia rheumatica, Crohn’s disease, or cancer of the respiratory system), or if they had a chronic adverse event outcome under study prior to the index date (to ensure that the first diagnosis of the studied chronic condition post-index date was an incident event).
Both cohorts were followed from the index date to the end of follow-up (ie, death, leaving the primary care practice, or end of available records or last date of extraction [March 2019], whichever occurred first). OCS prescriptions included those for betamethasone, cortisone, deflazacort, dexamethasone, hydrocortisone, methylprednisolone, prednisolone, prednisone or triamcinolone, with doses converted into prednisolone equivalents per the Anatomical Therapeutic Chemical/Defined Daily Dose classification system.Citation12 Intermittent OCS prescription patterns during follow-up were categorized as either one-off (a single OCS prescription), less frequent (>1 prescription with any gaps between prescriptions ≥90 days, but no gap <90 days) or frequent (>1 prescription with <90-day gap[s] between prescriptions).Citation5,Citation11 HCRU data on hospital admissions, and emergency department and specialty visits were extracted from the Clinical Practice Research Database (CPRD) GOLD database linked to Hospital Episode Statistics (HES [see Data source section below]).Citation13
Data Source
Patients’ electronic medical records for the current analysis were extracted from the CPRD GOLD database, an ongoing primary care database of anonymized medical records from GPs in the UK using Vision™ software (Surgical Information Systems, GA, USA),Citation14 which at the time of analysis had records for over 11 million patients from 674 practices. The CPRD GOLD records were linked to HES,Citation13 a data warehouse containing details of all hospital admissions, specialist appointments and emergency department visits at National Health Service (NHS) hospitals in the UK, up to March 2019.
Study Ethics
This study was conducted in accordance with the Strengthening and Reporting of Observational Studies in Epidemiology (STROBE) guidelinesCitation15 and was approved by an Independent Scientific Advisory Committee (CPRD approval number ISAC 20_000071). The study is registered with the ENCePP registration number EUPAS37065. No patient-identifying information was accessible during the study.
Healthcare Resource Utilization
Non-respiratory-related and all-cause data for the following HCRU categories were analysed: GP visits, inpatient hospital admission spells and primary care medication prescriptions. The number of HCRU events during follow-up was counted for eight HCRU measures (described in detail in the Supplementary Appendix). Non-respiratory-related data were available for GP visits, all hospital admissions (including and excluding day cases), day cases only, length of stay for hospital attendance (both overall and excluding day cases) and number of prescriptions for any medication type, including OCS. All-cause data were available for GP visits, emergency department visits, specialist visits, all hospital admissions (including and excluding day cases), day cases only, length of stay for hospital attendance (both overall and excluding day cases) and number of prescriptions for any medication type, including OCS. We only analysed emergency department and specialist visits for all-cause data, owing to a large number of these visits (~40%) that could not be classified as respiratory or non-respiratory using the coding in the HES database.
Healthcare Resource Utilization-Associated Costs
Prices assigned to GP visit costs were taken from the most recent Personal Social Services Research Unit (PSSRU) document at the time of study conduct (2020 version).Citation16 Prices assigned to secondary care costs were based on the UK national average of hospital costs in the PSSRU document (specialist visits and hospital admissions)Citation16 or the National Cost Collection Data Publication (emergency department visits).Citation17 Drug prices were derived using the cost per item from the NHS Digital electronic prescribing data,Citation18 with any gaps filled using the electronic British National FormularyCitation19 and the Medical Index of Medicinal Substances.Citation20
HCRU-associated costs during follow-up were then calculated by multiplying HCRU counts by the unit costs associated with each HCRU event from the PSSRUCitation16 and the cost per item using NHS Digital electronic prescribing data.Citation18 Prescription costs were obtained by multiplying cost by amount prescribed. All costs were reported in 2020 British pounds. Additionally, costs of hospital admissions due to corticosteroid-related adverse outcomes were calculated (Table S1),Citation21 including costs by individual OCS-related adverse outcomes.
Statistical Analysis
Descriptive statistics were reported as the number of patients and events for categorical variables and as means with standard deviations (SD) for continuous variables (or medians with interquartile ranges [IQR] if the distributions were skewed). Missing data for body mass index (BMI) and smoking status were imputed using multiple imputation techniques (data for BMI and smoking status were missing for 39–50% and 23–39% of records, respectively, in the HES-linked CRPD database). Missing dosing instructions (23% of prescriptions in 28% of patients) for OCS and other medication groups were imputed using modal daily doses at patient–drug level and drug level, respectively. Missing data were assumed to be missing at random with regard to exposure and outcome classifications.
Annualized HCRU was calculated as events per patient-year (see equations in the Supplementary Appendix), with the units of HCRU being episodes for all categories except for hospital length of stay (with and without day cases), which were expressed as days, and prescriptions, for which the units were records. HCRU-associated costs were calculated (Supplementary Appendix) per patient and per patient-year and reported for each prescribing pattern of intermittent OCS, as well as by cause of admission. Since it was not possible to distinguish respiratory or non-respiratory emergency department and specialist care visits for a large number of patients, we do not report non-respiratory costs for those types of HCRU.
Continuous variables were compared between groups using the Mann–Whitney test and categorical variables were compared between groups using the chi-square test. Analyses were conducted using Stata SE version 14.2 (StataCorp, College Station, TX, USA), and statistical significance was defined as p < 0.05.
Multivariable analyses were conducted using generalized linear models to investigate the association of intermittent OCS prescribing patterns with HCRU categories (compared with no use of OCS), adjusting for sex, age, smoking status, BMI and GINA 2020 treatment step at baseline, which was defined as the year prior to their first OCS prescription. Adjusted incident rate ratios were calculated from patient-level costs using a generalized linear model. As far as possible, diagnostic checks were performed during the model fitting stage to ensure that the analysis was consistent with the study objectives. Multiple imputation was used to strengthen the robustness of the results. We acknowledge that further sensitivity analyses are always possible, but we consider in this case the use of such well-developed methods for this type of analysis were appropriately applied.
Results
Cohort Characteristics
Overall, 2,345,661 patients in the HES-linked CPRD database had asthma, of whom 763,136 (34%) received an OCS prescription. Of these, 149,191 met the eligibility criteria for intermittent OCS prescription and were included in the OCS cohort (; the loss of patients in the analysis was largely driven by HES linkage). Of the 149,191 matched individuals who did not receive OCS at any time and were included in the matched non-OCS cohort, 143,522 (96.2%) did not have a diagnosis of asthma (matched on sex, age and index date). Records were available prior to the index date for a median (IQR) duration of 9.0 (4.2, 17.9) years for the intermittent OCS cohort and 10.4 (5.0, 19.4) years for the non-OCS cohort. The median (IQR) follow-up was 7.0 (3.5, 12.1) years and 7.7 (3.9, 13.1) years, respectively. The mean (SD) age was 38.7 (22.4) years in the intermittent OCS cohort and 38.7 (23.2) years in the non-OCS cohort, and 52.6% were female in both cohorts (). In comparison with the matched non-OCS cohort, more patients in the intermittent OCS cohort were obese (16.1% vs 10.2%) or current or former smokers (27.6% vs 21.4% and 15.8% vs 11.4%, respectively). The total non-steroid related Cambridge Comorbidity Index score was higher in patients who received frequent intermittent OCS (0.36) compared with those who received less-frequent OCS, one-off OCS or who were OCS-naïve (0.26, 0.25 and 0.25, respectively).
Figure 1 Study population selection from the UK CPRD database. aAsthma events included prescription for asthma medication, asthma review or asthma diagnosis. bThe methodology for determining whether patients received intermittent or long-term OCS is described in detail in a prior publication.Citation11 cConditions included ankylosing spondylitis, Sjogren’s syndrome, systemic lupus erythematosus, temporal arteritis, ulcerative colitis, psoriatic arthritis, multiple sclerosis, polymyalgia rheumatica, Crohn’s disease and cancer of the respiratory system. dThe OCS cohort was grouped by OCS prescription patterns: one-off, defined as a single OCS prescription; less frequent, defined as >1 prescription with any gaps ≥90 days but no gap <90 days; and frequent, defined as >1 prescription with <90-day gap(s). eThe non-OCS cohort was defined as the absence of any OCS prescription at any time pre-index, and the index date was the date of the GP visit nearest to the index date of matched OCS patient.
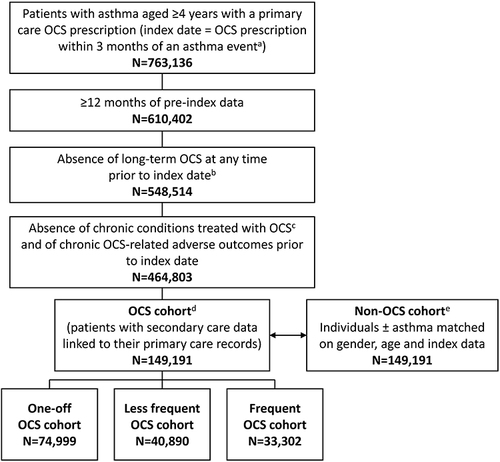
Table 1 Baseline Demographic and Clinical Characteristics of UK Patients with Asthma Receiving Intermittent OCS and Matched Non-OCS Individuals (with or without Asthma)
Of the 149,191 patients in the intermittent OCS cohort, 74,999 (50.3%), 40,890 (27.4%) and 33,302 (22.3%) were classified as having one-off, less frequent and frequent intermittent OCS prescribing patterns, respectively. Median (IQR) follow-up was 5.8 (2.8, 10.7), 9.0 (5.0, 14.0) and 7.5 (3.8, 12.5) years in the one-off, less frequent and frequent intermittent OCS groups, respectively, and the mean (SD) patient ages were 35.9 (22.7), 38.6 (23.1) and 45.2 (23.3) years, respectively. The mean (SD) cumulative OCS doses during follow-up were 183 (140) mg prednisolone equivalents for one-off, 505 (342) mg for less frequent and 1208 (2275) mg for frequent prescribing patterns of intermittent OCS ().
In the intermittent OCS cohort, 51.8% of patients were prescribed treatments indicative of mild asthma at the time of first OCS prescription (GINA 2020 treatment steps 1–2); the distribution of GINA 2020 treatment steps was similar for all three OCS prescribing patterns. Less than 1% of the intermittent OCS cohort (0.8%) were receiving therapy at GINA 2020 Step 5; of these 36% were prescribed frequent OCS. The proportion of patients receiving ≥7 ICS prescriptions in the 12 months prior to the index date increased with increasingly frequent patterns of OCS prescription, as did the proportion receiving ≥12 SABA prescriptions ().
Healthcare Resource Utilization
HCRU (unadjusted analyses) for non-respiratory-related consultations in the OCS and non-OCS cohorts, and by intermittent OCS prescribing patterns, is shown in and Table S2. Compared with the non-OCS cohort, patients in the intermittent OCS cohort had greater annualized rates per patient during the follow-up period for GP visits (5.93 vs 4.48 episodes, p < 0.0001), hospital admissions (0.24 vs 0.16 episodes, p < 0.0001), length of stay (1.87 vs 1.58 days, p < 0.0001) and any prescription that included OCS (18.09 vs 15.30 prescriptions, p < 0.0001) (). A dose–response relationship was apparent in that the rates of GP visits and any prescription increased with increasingly frequent prescribing patterns of intermittent OCS use (from 5.00 to 7.49 episodes and from 14.30 to 25.22 prescriptions, respectively; p < 0.0001 for both). For length of stay, total hospital and day-case admissions, the highest rates were observed with frequent OCS use, and the lowest rates with less frequent OCS use (both p < 0.0001) (). The exclusion of day cases from total hospital admissions resulted in similar outcomes. For all-cause consultations, the results for GP visits and any prescription in the OCS cohort were consistent with those observed for non-respiratory-related HCRU, with a trend for increasing rates with more frequent OCS prescribing patterns compared with non-use of OCS ( and Table S3).
Table 2 Non-Respiratory-Related and All-Cause and Annualized HCRU (HCRU Events/Patient-Year) for UK Patients in the Intermittent OCS Cohort, Intermittent OCS Subgroups and Non-OCS Cohort During the Entire Follow-Up Period
Results from the multivariable analysis showed that HCRU was greater in patients receiving intermittent OCS than in the non-OCS cohort for most non-respiratory-related and all-cause HCRU (). The exceptions were admissions and all prescriptions, including OCS, for patients with a one-off OCS prescribing pattern whose HCRU was lower than in the non-OCS cohort. In addition, it appeared that the difference in increased HCRU compared with the non-OCS cohort was more between the “one-off” group versus the “less frequent” and “frequent” groups rather than between these two latter groups. Overall, HCRU increased with increasing intermittent OCS prescribing pattern.
Table 3 Adjusted IRRsa for Non-Respiratory-Related and All-Cause Annualized HCRU for UK Patients According to Intermittent OCS Prescribing Pattern
Healthcare Resource Utilization-Associated Costs
Non-respiratory and all-cause healthcare costs by mean per patient and annualized per patient per year are shown in . Mean per-patient () and annualized () non-respiratory costs were higher in the OCS cohort (£3902 and £565, respectively) than in the matched non-OCS cohort (£2722 and £313, respectively). Mean per-patient costs were driven by less frequent (£4642) and frequent (£5539) OCS prescribing patterns compared with one-off OCS (£2773), and a similar trend was seen when costs were annualized (one-off, £473; less frequent, £548; frequent, £778). Likewise, mean per-patient () and annualized () all-cause costs were higher in the intermittent OCS cohort than in the matched non-OCS cohort; mean per-patient costs were £8623 and £4929 in the intermittent OCS and matched non-OCS cohort, respectively, and mean annualized costs were £1526 and £634, respectively. This cost difference was generally driven by the less frequent and frequent OCS prescription pattern groups, which incurred substantially higher mean per-patient costs than the non-OCS cohort and one-off OCS prescribing pattern group (one-off, £6955; less frequent, £10,125; frequent, £11,937). However, these trends were less clear when costs were annualized (one-off, £1443; less frequent, £1363; frequent, £1913).
Figure 2 Mean non-respiratory healthcare costs in the UK per patient (A); Mean non-respiratory healthcare costs in the UK per patient per year (B); Mean all-cause healthcare costs in the UK per patient (C); Mean all-cause healthcare costs in the UK per patient per year (D). The Any intermittent OCS group includes any patient who received intermittent OCS and includes all patients who received one-off OCS, less frequent OCS, and frequent OCS. 2020 British pounds [£] by HCRU categories and OCS use status.
![Figure 2 Mean non-respiratory healthcare costs in the UK per patient (A); Mean non-respiratory healthcare costs in the UK per patient per year (B); Mean all-cause healthcare costs in the UK per patient (C); Mean all-cause healthcare costs in the UK per patient per year (D). The Any intermittent OCS group includes any patient who received intermittent OCS and includes all patients who received one-off OCS, less frequent OCS, and frequent OCS. 2020 British pounds [£] by HCRU categories and OCS use status.](/cms/asset/22ba6ac7-b3bd-49d4-91d2-d983e0d11b5b/djaa_a_12303788_f0002_c.jpg)
Corticosteroid-Related Adverse Outcome Hospital Admission Costs
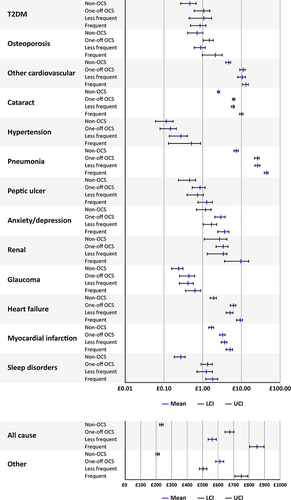
Unadjusted total annualized costs attributable to corticosteroid-related adverse outcomes are shown for hospital admissions in . In general, total annualized costs were higher in each OCS prescription pattern group compared with the non-OCS cohort. The cost differences between OCS prescribing patterns for hospital admissions associated with OCS-related adverse outcomes are less clear; costs were most likely highest with frequent prescribing, followed by one-off prescribing and lowest with less frequent OCS prescribing.
Figure 3 Total annualized costs of oral corticosteroid-related adverse outcomes identified from hospital admissions. “Other” refers to ICD-10 codes not specified for this analysis (see Table S1 for specified events) and comprised 36,877/37,668 (97.9%) inpatients in the intermittent OCS cohort and 16,109/16,506 (97.6%) inpatients in the non-OCS cohort. Costs are in 2020 British pounds (₤). x-axes are logarithmic except for All cause and Other.
Discussion
In this historical UK cohort study, patients with asthma who only received intermittent OCS prescriptions had a larger non-respiratory-related HCRU burden than patients not exposed to OCS. Patients who were prescribed intermittent OCS had increased non-respiratory-related HCRU in all areas, including GP, emergency department and specialist visits, hospital admissions (including and excluding day cases), length of stay and any prescriptions (including OCS) compared with individuals who had not been prescribed OCS. Among the intermittent OCS cohort, non-respiratory HCRU was generally highest among patients with a frequent OCS prescribing pattern compared with those with one-off and less frequent prescribing patterns, despite comparable disease severity as reflected by GINA treatment step at the time of first OCS use.
For all-cause HCRU, compared to non-OCS users, patients prescribed intermittent OCS also had increased burden across all areas. However, for emergency department, specialist visits, and all admissions, annualized all-cause HCRU was unexpectedly higher in the group of patients who received a one-off prescription of OCS than the less frequent prescribing pattern, and, subsequently, mean per-patient costs were higher with one-off OCS in these categories. Mean HCRU-associated per-patient and annualized costs for all visit types were also higher in the intermittent OCS cohort than in the non-OCS cohort, with highest costs among those with a frequent OCS prescribing pattern.
One potential explanation for the unexpectedly high annualized all-cause HCRU in patients receiving a one-off prescription of OCS is that some patients in this group did not visit primary care again after being given OCS. This may possibly be due to adverse outcomes, corticosteroid hesitancy or loss of patients from the database. Thus, the follow-up time for this group would have been shortened, inflating the annualized rates. Nevertheless, findings from multivariable analyses suggested that the main difference in increased HCRU compared with the non-OCS cohort was mostly between the one-off versus the less frequent and the frequent groups but not between these two latter groups, emphasizing the importance of preventing increasing frequency of prescription beyond the one-off pattern. The increase in mean HCRU-associated costs in the intermittent OCS cohort may potentially be attributable to OCS-related adverse outcomes, for which costs were increased with all intermittent OCS prescribing patterns compared with the non-OCS cohort. The greater prevalence of non-steroid related conditions included in the Cambridge Comorbidity Index score at baseline for the frequent prescription OCS group than the other three groups evaluated may also have had some potential impact on future HCRU.
Our results are concordant with a Swedish study, in which increasing average daily dose of OCS corresponded with increasing total annual healthcare costs in asthma patients with or without co-morbid chronic obstructive pulmonary disease;Citation22 age-adjusted costs were 3-times greater in those receiving long-term OCS (≥5 mg/day) and 1.5-times greater in the periodic OCS group (<5 mg/day) compared with non-OCS users. However, previous studies, such as the Swedish one described above, have only examined different levels of cumulative daily SCS/OCS dosages as an indicator of dosing frequency, and have included all types of prescriptions, including long-term OCS use.Citation9,Citation10,Citation23 As far as we are aware, ours is the first study to assess HCRU burden and cost exclusively associated with different patterns of intermittent OCS prescription in patients with asthma.
Our data showed that the frequency pattern of intermittent OCS prescription increased alongside total cumulative dose, which may partly reflect the association between dose and healthcare costs previously shown in the aforementioned Swedish study. However, given the observation that some patients with a one-off or less frequent pattern of OCS prescription had a higher cumulative dose than those with a frequent pattern, cumulative dose alone may not be the only factor and one should also consider the pattern of prescriptions when assessing the impact of OCS on health outcomes and HCRU.
The findings in this analysis indicate that the association between increased frequency of intermittent OCS prescription and increased risk of OCS-related adverse outcomes, as shown in our previously published study,Citation5 translates into higher HCRU and costs. This is further supported by other studies in patients with asthma that have demonstrated that OCS/SCS-related adverse outcomes are associated with additional HCRU and cost burden, either in comparison with patients with asthma who did not experience OCS-related adverse outcomesCitation24 or patients with no SCS exposure.Citation9,Citation10 This evidence provides a strong argument that improved management of patients with asthma is needed so that prescription of intermittent OCS in clinical practice can be minimized. Because corticosteroids are the cornerstone of acute asthma exacerbation management, this fosters prevention as the very first priority. Indeed, it is well known that patients with asthma tend to rely on SABA therapy and underuse ICS; however, this use of SABA without concomitant ICS does not treat the underlying inflammation,Citation25 and increasing SABA exposure is associated with an increased risk of severe exacerbations and poor asthma control.Citation26,Citation27 This, in turn, increases the likelihood that patients will receive OCS bursts to treat exacerbations. A previous analysis demonstrated that one-third of patients with asthma who received intermittent OCS had a frequent pattern of use at some point and that those with more frequent OCS prescribing patterns were more rapidly progressed to frequent OCS use;Citation11 both of these observations should be a warning signal for physicians to initiate a referral. Therefore, guidance around appropriate treatment and care to help implement strategies that could reduce the use of intermittent OCS is needed. Indeed, use of ICS-formoterol as both controller and reliever (Maintenance and Reliever Therapy) is well established and included in the GINA report to reduce the risk of exacerbations and thereby the use of OCS.Citation1 Other strategies to reduce the use of OCS include addressing risk factors for exacerbations, including smoking and poor inhaler technique, and improving adherence to treatment. These strategies should be effective even for people with severe asthma receiving biologic therapies.
This study has several strengths, including the focus on patients receiving intermittent OCS prescriptions. To our knowledge, this is the first study to examine the relationship between intermittent OCS prescribing patterns, HCRU and related costs. In addition, the use of well-established real-world databases representative of the UK population means that our results are widely generalizable, given that a large proportion of patients with asthma are managed in primary care.
Our study also has several limitations. The sophisticated classification algorithm focused on specificity (ensuring patients were intermittent OCS users) rather than sensitivity (ensuring all intermittent OCS users were captured), meaning that some intermittent OCS prescriptions may have been missed and this could affect the generalizability of the study. In addition, since most patients with asthma receive OCS at some point, the vast majority (>96%) of the non-OCS cohort consisted of individuals without asthma, and therefore one can argue that at least some of the increase in all-cause HCRU and cost may be asthma- and ICS-related.Citation28 To alleviate this issue, we focused on non-respiratory-related consultations in addition to all-cause consultations. The consistent results for non-respiratory-related and all-cause HCRU and costs suggest that the association between patterns of intermittent OCS prescriptions and HCRU and costs is real. However, these data should be interpreted with caution as many codes by cause for emergency department and specialist visits in the HES database were missing, limiting the evaluation of respiratory-related versus non-respiratory-related HCRU categories. Another limitation was that OCS prescription patterns were used as a surrogate for exposure, and so true adherence to OCS was not measured. Also, to achieve a standard comparison between the different intermittent OCS prescription groups, the costs of prescriptions were calculated in 2020 British pounds, not the cost at the time of prescription; this might have resulted in non-differential measurement error of the prescription costs across all events and could have potentially biased our results towards the null. Corticosteroid-related adverse outcome costs were based on the most prevalent OCS-related adverse outcomes and so may not have captured all corticosteroid-related adverse outcomes. Additionally, it is possible that some of the adverse outcomes detected in patients with one-off prescription of OCS were instead caused by the use of high-dose ICS, which was not assessed here. Owing to the inclusion criteria, <1% of patients were receiving therapy at GINA 2020 Step 5 and future analyses may evaluate other OCS sparing medications, including biologics and leukotriene receptor antagonists, that are used in this population. The CPRD and HES datasets used for these analyses were collected for clinical and routine use rather than for specific research purposes, and hence there were some missing data, eg BMI, smoking status, and OCS/ICS dosing instruction (with many prescribing instructions not been coded by CPRD). Although the use of multiple imputation techniques may have lessened the uncertainty due to the issue, the findings may still be subject to residual confounding from adjusting for the imputed variables or from patient characteristics not available for this analysis. Finally, participants were not matched on location, and data may therefore be affected by regional heterogeneity.
Conclusions
Our study found that intermittent prescribing of OCS in patients with asthma was associated with increased HCRU and associated costs versus no prescription of OCS, for both non-respiratory and all-cause costs. There was also a dose-related trend in that more frequent prescribing patterns of intermittent OCS were generally linked with a higher burden on healthcare resources across all areas of HCRU including GP, emergency department and specialist visits, hospital admissions and prescriptions, which led to increased costs. These findings emphasize the importance of appropriate asthma management to lessen the risk of exacerbations and thereby reduce the need for intermittent prescription of OCS. It is important that underuse of ICS and/or reliance on SABA-only rescue is addressed to minimize the risk of exacerbations requiring OCS treatment, and that OCS is only used when strictly necessary and as recommended in major treatment guidelines and reports.
Abbreviations
BMI, body mass index; BNF, British National Formulary; CPRD, Clinical Practice Research Database; GINA, Global Initiative for Asthma; GP, general practitioner; HCRU, healthcare resource utilization; HES, Hospital Episode Statistics; ICS, inhaled corticosteroids; IQR, interquartile range; NHS, National Health Service; OCS, oral corticosteroids; PSSRU, Personal Social Services Research Unit; SABA, short-acting β2-agonist; SCS, systemic corticosteroids; SD, standard deviation.
Study Ethics
This study was conducted in accordance with the Strengthening and Reporting of Observational Studies in Epidemiology (STROBE) guidelines and was approved by an Independent Scientific Advisory Committee (CPRD approval number ISAC 20_000071). The study is registered with the ENCePP registration number EUPAS37065. No patient-identifying information was accessible during the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
CA, HH, JSKC, VC and WH are employees of Observational and Pragmatic Research Institute, Singapore, who conducted this study, funded by AstraZeneca.
WH reports grants from AstraZeneca, during the conduct of the study; grants from Chiesi Pharmaceuticals, outside the submitted work.
VC works for The Optimum Patient Care Global who received funding/grant for the study.
DP has advisory board membership with AstraZeneca, Boehringer Ingelheim, Chiesi Pharmaceuticals, Mylan, Novartis, Regeneron, Sanofi. Thermofisher Scientific and Viatris; consultancy agreements with Airway Vista Secretariat, AstraZeneca, Boehringer Ingelheim, Chiesi Pharmaceuticals, EPG Communication Holdings Ltd, FIECON Ltd, Fieldwork International, GlaxoSmithKline, Medscape, Mylan, Mundipharma, Novartis, OM Pharma SA, PeerVoice, Phadia AB, Spirosure Inc, Strategic North Limited, Synapse Research Management Partners S.L., Talos Health Solutions, Teva Pharmaceuticals, Theravance Biopharma, Viatris and WebMD Global LLC; grants and unrestricted funding for investigator-initiated studies (conducted through Observational and Pragmatic Research Institute Pte Ltd) from AstraZeneca, Boehringer Ingelheim, Chiesi, Mylan, Novartis, Regeneron Pharmaceuticals, Respiratory Effectiveness Group, Sanofi, Theravance, UK National Health Service and Viatris; payment for lectures/speaking engagements from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, GlaxoSmithKline, Inside Practice, Kyorin, Medscape, Mylan, Mundipharma, Novartis, Regeneron Pharmaceuticals, Sanofi, Teva Pharmaceuticals and Viatris; payment for travel/accommodation/meeting expenses from AstraZeneca, Boehringer Ingelheim, Mundipharma, Mylan, Novartis, Teva Pharmaceuticals and Thermofisher; stock/stock options from AKL Research and Development Ltd which produces phytopharmaceuticals; owns 74% of the social enterprise Optimum Patient Care Ltd (Australia and UK) and 92.61% of Observational and Pragmatic Research Institute Pte Ltd (Singapore); 5% shareholding in Timestamp which develops adherence monitoring technology; is peer reviewer for grant committees of the UK Efficacy and Mechanism Evaluation programme and Health Technology Assessment; and was an expert witness for GlaxoSmithKline.
JC, EM, AMG, and TNT are employees of, and own stock in, AstraZeneca.
JH reports personal fees from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, Circassia and Teva unrelated to the conduct of the study.
AB has received consultancy fees and speakers’ fees from of AstraZeneca, Amgen, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis, Sanofi and Regeneron, and research grants from AstraZeneca, Boehringer Ingelheim and GlaxoSmithKline.
AMG is an employee of, and owns stock in, AstraZeneca and has received grants, advisory board fees, lecture fees and consulting fees from AstraZeneca; advisory board fees from GlaxoSmithKline; advisory board fees and lecture fees from Novartis; advisory board fees, lecture fees and travel expenses from Teva; advisory board fees from Regeneron; and advisory board fees, lecture fees and consulting fees from Sanofi.
DJJ has received consultancy fees and speakers’ fees from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Sanofi and Regeneron, and research grants from AstraZeneca.
Acknowledgments
We would like to thank Anna Mett of inScience Communications, Springer Healthcare, UK, for providing medical writing support, which was funded by AstraZeneca.
Data Sharing Statement
The dataset supporting the conclusions of this article was derived from the Optimum Patient Care Research Database (www.opcrd.co.uk). The authors do not have permission to give public access to the study dataset; researchers may request access to OPCRD data for their own purposes. Access to OCPRD can be made via the OCPRD website (https://opcrd.co.uk/our-database/data-requests/) or via the enquiries Email [email protected].
Additional information
Funding
References
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention; 2024. Available from: www.ginasthma.org. Accessed June 07, 2024.
- Ekstrom M, Nwaru BI, Hasvold P, Wiklund F, Telg G, Janson C. Oral corticosteroid use, morbidity and mortality in asthma: a nationwide prospective cohort study in Sweden. Allergy. 2019;74(11):2181–2190. doi:10.1111/all.13874
- Lefebvre P, Duh MS, Lafeuille MH, et al. Burden of systemic glucocorticoid-related complications in severe asthma. Curr Med Res Opin. 2017;33(1):57–65. doi:10.1080/03007995.2016.1233101
- Volmer T, Effenberger T, Trautner C, Buhl R. Consequences of long-term oral corticosteroid therapy and its side-effects in severe asthma in adults: a focused review of the impact data in the literature. Eur Respir J. 2018;52(4):1800703. doi:10.1183/13993003.00703-2018
- Heatley H, Tran TN, Bourdin A, et al. Observational UK cohort study to describe intermittent oral corticosteroid prescribing patterns and their association with adverse outcomes in asthma. Thorax. 2023;78(9):860–867. doi:10.1136/thorax-2022-219642
- Chan JSK, Murray RB, Price D. Oral corticosteroids in asthma and beyond: moving forward. Eur Respir J. 2022;60(3):2200776. doi:10.1183/13993003.00776-2022
- Bleecker ER, Menzies-Gow AN, Price DB, et al. Systematic literature review of systemic corticosteroid use for asthma management. Am J Respir Crit Care Med. 2020;201(3):276–293. doi:10.1164/rccm.201904-0903SO
- Wang E, Wechsler ME, Tran TN, et al. Characterization of severe asthma worldwide: data from the International Severe Asthma Registry. Chest. 2020;157(4):790–804. doi:10.1016/j.chest.2019.10.053
- Dalal AA, Duh MS, Gozalo L, et al. Dose-response relationship between long-term systemic corticosteroid use and related complications in patients with severe asthma. J Manag Care Spec Pharm. 2016;22(7):833–847. doi:10.18553/jmcp.2016.22.7.833
- Voorham J, Xu X, Price DB, et al. Healthcare resource utilization and costs associated with incremental systemic corticosteroid exposure in asthma. Allergy. 2019;74(2):273–283. doi:10.1111/all.13556
- Haughney J, Tran TN, Heatley H, et al. Application of an algorithm to analyze patterns of intermittent oral corticosteroid use in asthma. NPJ Prim Care Respir Med. 2023;33(1):9. doi:10.1038/s41533-023-00331-0
- World Health Organization Collaborating Centre for Drug Statistics Methodology. ATC/DDD Index; 2022. Available from: www.whocc.no/atc_ddd_index/. Accessed November 2, 2022.
- National Health Service Digital. Hospital Episode Statistics; 2021. Available from: https://digital.nhs.uk/data-and-information/data-tools-and-services/data-services/hospital-episode-statistics. Accessed March 4, 2022.
- Kousoulis AA, Rafi I, de Lusignan S. The CPRD and the RCGP: building on research success by enhancing benefits for patients and practices. Br J Gen Pract. 2015;65(631):54–55. doi:10.3399/bjgp15X683353
- von Elm E, Altman DG, Egger M, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007;335(7624):806–808. doi:10.1136/bmj.39335.541782.AD
- Curtis LA, Burns A. Unit Costs of Health & Social Care 2020. Kent, UK: Personal Social Services Research Unit; 2020.
- NHS England. 2019/20 National Cost Collection Data Publication; 2021. Available from: https://www.england.nhs.uk/publication/2019-20-national-cost-collection-data-publication/. Accessed February 2, 2022.
- National Health Service Digital. Prescription Cost Analysis - England, 2018; 2019. Available from: https://digital.nhs.uk/data-and-information/publications/statistical/prescription-cost-analysis/2018. Accessed February 2, 2022.
- Joint Formulary Committee. British National Formulary. 76 ed. London: BMJ Group and Pharmaceutical Press; 2018.
- Haymarket Media Group Ltd. Medical Index of Medicinal Substances (MIMS); 2021. Available from: https://www.mims.co.uk/. Accessed March 4, 2022.
- Price DB, Trudo F, Voorham J, et al. Adverse outcomes from initiation of systemic corticosteroids for asthma: long-term observational study. J Asthma Allergy. 2018;11:193–204. doi:10.2147/JAA.S176026
- Janson C, Lisspers K, Stallberg B, et al. Health care resource utilization and cost for asthma patients regularly treated with oral corticosteroids - a Swedish observational cohort study (PACEHR). Respir Res. 2018;19(1):168. doi:10.1186/s12931-018-0855-3
- Zeiger RS, Schatz M, Li Q, Chen W, Khatry DB, Tran TN. Burden of chronic oral corticosteroid use by adults with persistent asthma. J Allergy Clin Immunol Pract. 2017;5(4):1050–1060 e1059. doi:10.1016/j.jaip.2016.12.023
- Luskin AT, Antonova EN, Broder MS, Chang EY, Omachi TA, Ledford DK. Health care resource use and costs associated with possible side effects of high oral corticosteroid use in asthma: a claims-based analysis. Clinicoecon Outcomes Res. 2016;8:641–648. doi:10.2147/CEOR.S115025
- Janson C, Menzies-Gow A, Nan C, et al. SABINA: an overview of short-acting beta2-agonist use in asthma in European countries. Adv Ther. 2020;37(3):1124–1135. doi:10.1007/s12325-020-01233-0
- Bateman ED, Price DB, Wang HC, et al. Short-acting β2-agonist prescriptions are associated with poor clinical outcomes of asthma: the multi-country, cross-sectional SABINA III study. Eur Respir J. 2022;59(5): 2101402. doi:10.1183/13993003.01402-2021
- Quint JK, Arnetorp S, Kocks JWH, et al. Short-acting beta-2-agonist exposure and severe asthma exacerbations: SABINA findings from Europe and North America. J Allergy Clin Immunol Pract. 2022;10(9):2297–2309 e2210. doi:10.1016/j.jaip.2022.02.047
- Bourdin A, Suehs C, Charriot J. Integrating high dose inhaled corticosteroids into oral corticosteroids stewardship. Eur Respir J. 2020;55(1):1902193. doi:10.1183/13993003.02193-2019