
Abstract
Background
The literature on the relationship between diet and asthma has largely focused on individual nutrients, with conflicting results. People consume a combination of foods from various groups that form a dietary pattern. Studying the role of dietary patterns in asthma is an emerging area of research. The purpose of this study was to systematically review dietary patterns and asthma outcomes in adults and children, to review maternal diet and child asthma, and to conduct a meta-analysis on the association between asthma prevalence and dietary patterns in adults.
Methods
We searched Medline, Scopus, and ISI Web of Knowledge up to January 2014. Two researchers independently reviewed studies meeting the inclusion criteria using the American Dietetic Association quality criteria. A linear mixed model was used to derive the pooled effect size (95% confidence interval) for each of three dietary pattern categories (healthy, unhealthy, and neutral).
Results
Thirty-one studies were identified (16 cross-sectional, one case-control, 13 cohort, and one randomized controlled trial), including 12 in adults, 13 in children, five in pregnant woman–child pairs, and one in both children and pregnant woman–child pairs. Six of the 12 adult studies reported significant associations between dietary patterns and asthma outcomes (eg, ever asthma and forced expiratory volume in one second). Seven of ten studies examining the Mediterranean diet showed protective effects on child asthma and/or wheeze. Four of the six studies in mother-child pairs showed that maternal dietary patterns during pregnancy were not associated with child asthma or wheeze. The meta-analysis including six adult studies, the primary outcome of which was the prevalence of current or ever asthma, showed no association with healthy, unhealthy, or neutral dietary patterns.
Conclusion
The evidence suggests no association of dietary patterns with asthma prevalence in adults or of maternal diet with child asthma or wheeze. The Mediterranean diet in children may prevent asthma or wheeze, but randomized controlled trials are lacking.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
Over the past few decades, the prevalence of asthma has markedly increased. In the USA, the number of people with asthma increased from 20.3 million (6.3 million children and 14 million adults) in 2001 to 25.6 million (6.8 million children and 18.7 million adults) in 2012.Citation1,Citation2 Worldwide, asthma affects approximately 300 million people, and this number is expected to reach 400 million by 2050.Citation3
Although contributory, genetic factors alone cannot account for the rapid increase in the prevalence of asthma.Citation4 It has been hypothesized this increase is largely caused by environmental changes (eg, urbanization) and modification of lifestyle behaviors (eg, dietary transition).Citation5 Notably, the transition from a traditional to a modern diet is characterized by an increased intake of preserved foods, salt, refined sugar, and saturated fat, and a decreased intake of fruit, vegetables, milk, and dietary fiber.Citation6
Previous studies of the relationship of diet and nutrition with asthma have focused on either individual nutrients (eg, long-chain polyunsaturated fatty acids, vitamin D, and antioxidants)Citation6–Citation8 or individual food groups (eg, fruit, vegetables, and fish).Citation9–Citation11 However, diet is a complex combination of foods from various groups and nutrients, and some nutrients are highly correlated. It would be challenging to separate the effect of a single nutrient or food group from that of others in free-living populations. Chance findings may arise from indiscriminate multiple statistical testing and from inadequate control for confounding in observational studies. The available evidence from intervention trials focusing on the efficacy of single nutrients as disease-modifying agents in asthma is largely inconsistent.Citation12,Citation13
More recently, a few studies have investigated the association between overall dietary patterns and asthma. Due to the rapid evolution of research on this topic, it is worth performing a comprehensive literature review. One recently published meta-analysis of eight cross-sectional studies in children concluded that the Mediterranean diet might protect against ever asthma and current wheeze.Citation14 To date, no reviews of dietary pattern studies in adult asthma have been published. The objectives of this research were to systematically review the up-to-date findings on the effects of dietary patterns on asthma outcomes in adults and children as well as the effects of maternal dietary patterns on asthma outcomes in children, and to conduct a meta-analysis of published studies examining the effect of dietary patterns on asthma prevalence in adults.
Methods
We followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement to prepare the manuscript.Citation15
Literature search strategy
An electronic literature search was conducted using Medline (PubMed), Scopus, and ISI Web of Knowledge in January 2014 and extended back to 1950. The terms used to search titles and abstracts were (asthma OR wheezing OR wheeze OR lung function) AND (diet OR dietary OR food pattern). Further details on the literature search are shown in the Appendix 1. Only original studies with human subjects and published in English were included. In addition, cross-referencing from the articles found was used to complete the search. To be included in the systematic review, a study needed to have at least one dietary pattern predefined and measured (eg, Mediterranean) or generated from usual dietary intake using a multivariate statistical method and examine the effect or association of the dietary pattern(s) with one or more asthma outcome.
Inclusion criteria
The meta-analysis included studies of dietary patterns and asthma prevalence in adults meeting the following criteria: primary outcomes included prevalence of current or ever asthma, which was most commonly reported in the reviewed studies for adults (the number of studies assessing other asthma outcomes was too small to perform a meta-analysis); a dietary pattern score was calculated or dietary patterns were identified using a statistical method such as principal component analysis (PCA; selective solo or oligo food groups, eg, fruit and vegetables or fruit and fish, were not eligible); and odds ratio (OR) was calculated to determine the association between the dietary pattern(s) and asthma prevalence. Two researchers (NL and LX) independently reviewed the identified relevant articles and judged whether they met the inclusion criteria for meta-analysis. Uncertainties and discrepancies were resolved by consensus after discussing with a senior researcher (JM).
Quality assessment
The same two researchers (NL and LX) independently rated all the research articles included in the systematic review using the American Dietetic Association Quality Criteria Checklist.Citation16 The scientific soundness of the articles was rated using ten validity questions. Based on the answers, one of the three quality ratings was assigned: positive (answered “yes” to six or more validity questions, including four priority questions), negative (answered “no” to six or more validity questions), or neutral (the rest of the situations). Only articles with a positive or neutral quality rating were included in the meta-analysis.
Assessment of dietary patterns and data extraction
When statistically derived using PCA or factor analysis, usually multiple dietary patterns were reported. Two researchers (NL and LX) independently grouped all dietary patterns into three categories: healthy, unhealthy, or neutral, based on constituent foods of each pattern suggested by PCA or main factor loadings. Any disagreements were discussed with the senior researcher (JM). shows dietary patterns, categories, and constituent foods. A healthy dietary pattern was characterized by high intakes of fruit, vegetables, whole grains, and/or fish. An unhealthy dietary pattern tended to have high loadings of refined grain, red meat, processed meat, fast foods, high sugar foods, and/or high fat foods. A neutral dietary pattern generally consisted of a mixture of healthy and unhealthy food items. The same two researchers (NL and LX) independently extracted the data to be used for meta-analysis.
Table 1 Dietary patterns, categories, and constituent foods from six adult studies included in the meta-analysis
Statistical analysis
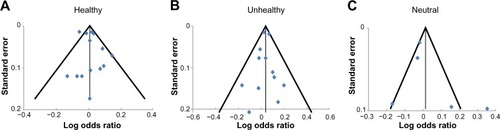
We performed a meta-analysis to evaluate the association of dietary patterns with asthma prevalence in adults. Studies reported dietary pattern scores either as continuous variables or categorized them into tertiles or quintiles. Linear mixed models were used to derive the pooled effect sizes and 95% confidence intervals (CIs) for healthy, unhealthy, and neutral dietary patterns and to assess heterogeneity between studies.Citation17 In addition, heterogeneity and publication bias were visually evaluated using Begg’s funnel plots, which displayed the scatter patterns of effect estimates against standard errors from the included studies, with a vertical line indicating the pooled estimate and diagonal lines showing the expected 95% CIs around the estimate.Citation18 All statistical analyses were conducted using SAS version 9.2 (SAS Institute Inc., Cary, NC, USA).
Results
Search results
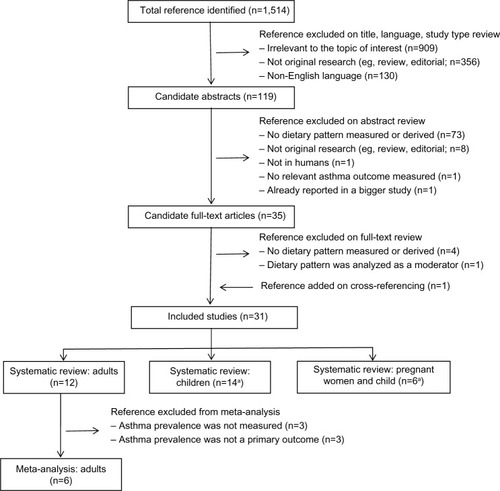
Of 1,514 references identified, 1,484 were excluded based on review of title (n=1,395), language (n=84), and study type, abstract, and full text (n=5), as shown in . One reference was added on cross-referencing. Thirty-one studies were eligible for systematic review, including 12 in adults, 13 in children, five in pregnant woman–child pairs, and one in both children alone and pregnant woman–child pairs. Six studies in adults were excluded from meta-analysis because asthma prevalence was not measured (three studies assessed asthma control, quality of life, lung function, and/or inflammatory markers) or was not a primary outcome (three studies assessed chronic obstructive pulmonary disease or persistent cough with phlegm as a primary outcome).
Figure 1 Results of search for relevant studies.
Scientific quality
OneCitation19 of the 31 studies was published as a conference abstract only and was not included in our quality review. Twenty-eight studies were rated positive (scoring 8 or 9 out of 10; –). OneCitation20 of the two studies rated as neutral was a case-control study that received a quality score of 8, but did not clearly describe whether potential confounding factors were comparable for the cases and controls, although the potential confounding variables were adjusted for in the analyses. The other studyCitation21 was a randomized controlled trial (RCT) that did not clearly describe the method of randomization or the amount of exposure to intervention. No study was excluded from meta-analysis based on quality ratings.
Table 2 Summary of 12 studies reporting an association between dietary patterns and asthma outcomes in adults
Table 4 Summary of six studies reporting the association between maternal dietary patterns and wheeze in children
Adult dietary patterns and asthma
Systematic review
shows the main characteristics and results of the 12 studies in adults, published between 2006 and 2013. These papers included four cross-sectional studies,Citation22–Citation25 six cohort studies,Citation26–Citation31 one case-control study,Citation20 and one RCT.Citation21 Six of them were conducted in Europe,Citation20,Citation23–Citation27 two in Australia,Citation21,Citation22 two in the USA,Citation28,Citation29 and two in Asia.Citation30,Citation31 Sample sizes ranged from 38 in the RCT to 156,035 in the cross-sectional studies. Two studiesCitation27,Citation28 included female subjects only and oneCitation29 male subjects only, while the remaining examined both sexes, with oneCitation22 examining men and women separately.
All studies used food frequency questionnaires (FFQs) to measure dietary intakes, with the number of food items or groups ranging from 12 to over 200. Ten studiesCitation20,Citation22–Citation24,Citation26–Citation31 derived at least two dietary patterns a posteriori using PCA (n=9) or factor analysis (n=1). Two studiesCitation21,Citation25 calculated a Mediterranean diet score defined a priori.
Asthma outcomes evaluated in these studies included prevalence of ever or current asthma, asthma-related quality of life, asthma symptoms, lung function (forced expiratory volume in one second, forced vital capacity), frequency of asthma attacks, asthma control (Asthma Control Questionnaire alone or plus fractional exhaled nitric oxide), and asthma-related inflammatory markers. The findings were mixed. Among the 12 studies, six reported significant association between dietary patterns and ever asthma,Citation22,Citation31 forced expiratory volume in one second,Citation24,Citation26 frequency of asthma attacks,Citation27 and risk of uncontrolled asthma.Citation25 Although the asthma outcomes varied across these studies, potentially protective dietary patterns tended to include cheese/brown bread, nuts and wine, a prudent pattern diet (fruit, vegetables, oily fish, and wholemeal cereals), and the Mediterranean diet. At the same time, potentially risky dietary patterns tended to include meats/cheese, Chinese traditional pattern (rice and fresh vegetables), the Netherlands traditional diet (meat and potatoes), and Western pattern (pizza, salty pies, desserts, and cured meat). In contrast, one cross-sectional,Citation23 one case-control,Citation20 and three cohort studiesCitation28–Citation30 reported no association. An RCT with 38 adults who had symptomatic asthma showed no effect of two Mediterranean diet interventions on asthma control, lung function, asthma-related quality of life, or inflammatory markers compared with no-intervention control.Citation21
Results of meta-analysis
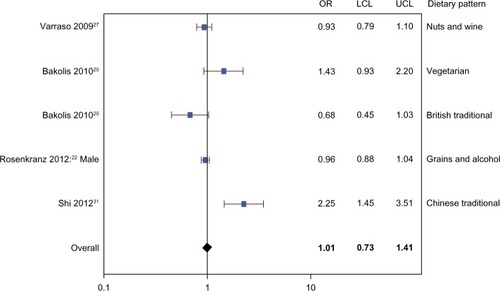
The meta-analysis included three cohort studies,Citation26,Citation27,Citation31 two cross-sectional studies,Citation22,Citation23 and one case-control study.Citation20 – show that there was no evidence of association between the prevalence of current or ever asthma and healthy (OR 1.01, 95% CI 0.78–1.31), unhealthy (OR 1.04, 95% CI 0.93–1.16), or neutral (OR 1.01, 95% CI 0.73–1.41) dietary patterns. The mixed model results show that the random effect estimates were zero, suggesting very small or negligible variance between versus within studies.
Figure 2 Meta-analysis of observational studies examining the association between healthy dietary patterns and prevalence of current or ever asthma.
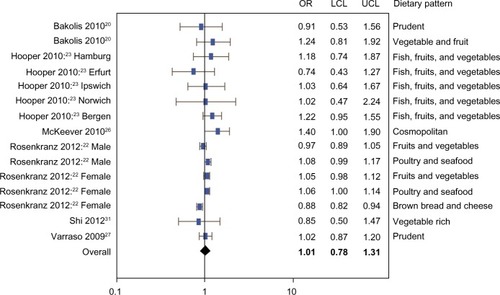
Figure 3 Meta-analysis of observational studies examining the association between unhealthy dietary patterns and prevalence of current or ever asthma.
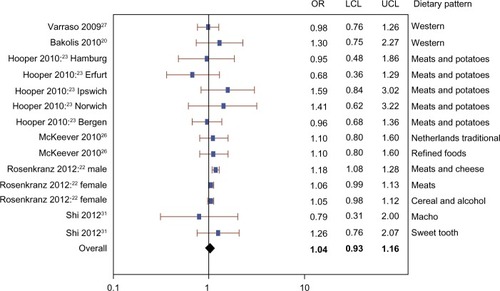
Figure 4 Meta-analysis of observational studies examining the association between neutral dietary patterns and prevalence of current or ever asthma.
Publication bias and heterogeneity
shows funnel plots of studies examining the association between healthy, unhealthy, and neutral dietary patterns separately and the prevalence of current or ever asthma. The plots were roughly symmetrical, suggesting little evidence of publication bias, and almost all the studies lay within the diagonal lines indicating 95% CIs, suggesting negligible between-study heterogeneity, which is consistent with the model-based results described above.
Figure 5 Funnel plots of studies in meta-analysis.
Child dietary patterns and asthma
The main characteristics and results of the 14 studies in children, published between 2006 and 2013, are shown in . Twelve studies were cross-sectional and twoCitation32,Citation33 were cohort studies. Nine of them were conducted in Europe,Citation19,Citation32,Citation34–Citation40 three in America (one in BrazilCitation41 and two in MexicoCitation33,Citation42), and one in Asia.Citation43 One other studyCitation44 was an international study conducted in 20 countries. All studies examined both boys and girls with sample sizes ranging from 158 (cohort) to 50,004 (cross-sectional).
Table 3 Summary of 14 studies reporting the association between dietary patterns and asthma outcomes in children
Eight of these studies (shown in the footnote to ) were included in a recent meta-analysisCitation14 to investigate whether the Mediterranean diet has a protective effect on ever asthma and current wheeze and whether these relationships were specific to the Mediterranean regions. The meta-analytic results showed adherence to the Mediterranean diet was negatively associated with current wheeze (OR 0.79, 95% CI 0.66–0.94; P=0.009) and current severe wheeze (OR 0.66, 95% CI 0.48–0.90; P=0.008) in Mediterranean regions, and with ever asthma (OR 0.86, 95% CI 0.75–0.98; P=0.027) in non-Mediterranean regions. When considering all regions together, the authors concluded adherence to the Mediterranean diet tended to have a protective effect on current wheeze and ever asthma but not on current severe wheeze.
The meta-analysisCitation14 excluded six studies for the following reasons: three studies derived dietary patterns a posteriori,Citation32,Citation41,Citation43 one measured lung function as the lone outcome,Citation33 and twoCitation34,Citation35 reported data published in other studies that were included in the meta-analysis. The limited additional studies on dietary patterns and child asthma or wheeze precluded another meta-analysis. Among these six studies, five found either a beneficial effect of the Mediterranean diet or a detrimental effect of an unhealthy (eg, Western) pattern. Interestingly, one study reported that the Mediterranean diet was a risk factor for severe asthma in girls aged 6–7 years.Citation35 The authors speculated this could be due to a reverse causal effect (families of children with severe asthma may improve their diet) and residual confounding.
Overall, the meta-analysis and six additional studies suggest that the Mediterranean diet is potentially protective against child asthma.
Maternal dietary patterns and child asthma
shows the main characteristics and results of the six studies reporting an association between maternal dietary patterns and asthma prevalence in children. All were cohort studies published between 2008 and 2013, with four conducted in Europe,Citation38,Citation45–Citation47 one in the USA,Citation48 and one in Asia.Citation49 Sample sizes ranged from 460 to 14,062.
All studies used FFQs to measure dietary intakes, with number of food items or groups ranging from 42 to 166. Three studiesCitation38,Citation45,Citation46 calculated a Mediterranean diet score defined a priori. Two studiesCitation47,Citation49 derived dietary patterns using PCA or factor analysis. One studyCitation48 used a combination of both a posteriori and a priori approaches to measure dietary patterns.
These studies examined the association between maternal dietary patterns and wheezing prevalence in children between the ages of one and 7 years. The heterogeneity of the study populations and outcomes precluded a meta-analysis. However, four of the six studies did not find any association between maternal dietary patterns and prevalence of wheezing. One studyCitation38 reported a protective effect of maternal Mediterranean diet pattern on persistent wheeze (OR 0.22, 95% CI 0.08–0.58) and atopic wheeze (OR 0.30, 95% CI 0.10–0.90) in offspring at age 6.5 years. Another studyCitation49 conducted in Japan found a beneficial effect of maternal “Western” dietary pattern on wheeze (OR 0.59, 95% CI 0.35–0.98; P=0.02) in toddlers aged 16–24 months. The authors noted that this “Western” dietary pattern in Japan might be comparatively healthier than the typical Western dietary pattern in the USA, because it was characterized by low intake of soft drinks, confectionery, and fruit, in addition to high intake of vegetable oil, salt-containing seasonings, beef, pork, processed meat, eggs, chicken, and white vegetables. Adherence to this “Western” dietary pattern was actually positively associated with a high intake of α-linolenic acid, vitamin E, and β-carotene, which were shown in some studies to have a beneficial effect on asthma and wheezing.Citation7,Citation9,Citation50,Citation51 The Japanese study suggests that dietary patterns are region-specific and population-specific, and that caution is necessary when interpreting the results of studies in diverse populations. Overall, these studies show weak evidence of any association between maternal dietary pattern and child wheezing.
Discussion and conclusion
Taken together, studies in adults and pregnant woman–child pairs failed to show that dietary patterns were associated with asthma outcomes. Only studies in children suggested a protective effect of the Mediterranean diet on current wheeze and ever asthma.
Compared with studying individual foods or nutrients, an evaluation of dietary patterns may shed light on the combinatorial effects of foods and/or nutrients on the health outcome of interest. Studying the overall effect of dietary patterns on asthma is an emerging literature; however, the findings so far have been inconsistent. We offer several possible explanations for the inconsistency and suggestions for future research.
First, the heterogeneous results may be partially explained by the notable variation in FFQs used for measuring dietary intakes and statistical approaches for deriving dietary patterns. For example, in adult studies, the FFQs included between 12 and over 200 food items or groups, which could influence the selection of foods loaded on the dietary patterns. Although most of the FFQs were validated, the dietary patterns derived from them explained only a small to medium percentage of total variance, ranging from 11% to 58% in the five adult studies that reported this information.
Two approaches, a priori and a posteriori, have been used to generate dietary patterns. Both approaches have strengths and weaknesses. The a priori approach focuses on a predefined dietary pattern based on prior knowledge of a specific diet (eg, Mediterranean) and its relationship to disease. Therefore, this approach is limited by current knowledge and could involve uncertainties in selecting individual components of the diet index and subjective decisions of defining cutoffs.Citation52 In contrast, the a posteriori approach provides opportunities to open up new areas of diet-disease research and detect dietary patterns specific to the region and/or population of interest. However, it involves important but arbitrary decisions, including the number of components to extract, the method of rotation, consolidation of food items into groups, and labeling of the components.Citation53 Researchers should choose the appropriate method according to the study objectives and dietary characteristics of the study population.
Most studies in children (eleven of 14) and pregnant woman–child pairs (four of six) used an a priori approach and defined the dietary pattern using a Mediterranean diet index, whereas ten of 12 studies in adults utilized an a posteriori approach to derive dietary patterns statistically (eg, with PCA). In addition to the Mediterranean diet, future studies may also examine the association between healthy dietary patterns in other regions (eg, the widely promoted Dietary Approaches to Stop Hypertension in the USACitation54) or alternative diet quality indices (eg, the Healthy Eating IndexCitation55) and asthma outcomes. If using the a posteriori approach, the reliability and validity of the dietary patterns generated from FFQs can be examined using a different source of dietary data (eg, dietary records). To examine the reproducibility of the dietary patterns, sensitivity analyses can be performed to test whether the arbitrary choices made during PCA or factor analysis influence the results and whether similar dietary patterns can be obtained using randomly split samples.Citation52
Statistical approaches used to derive dietary patterns a posteriori have included PCA, factor analysis, cluster analysis, and to a lesser extent, reduced rank regression. Some review papers detailed each of these approaches.Citation56,Citation57 Different from the exploratory approaches (eg, PCA, factory analysis, and cluster analysis), reduced rank regression defines linear combinations of food intakes that maximally explain the outcome variable (eg, an asthma outcome). In other words, in contrast with PCA and factor analysis, which derive dietary patterns to maximally explain the variance in food intake among participants, reduced rank regression identifies dietary patterns to maximally explain the outcome variable. Among the studies reviewed in this paper, most used PCA, two used factor analysis, and only one in children used reduced rank regression. This may be another reason why many studies of dietary patterns using PCA or factor analysis found no associations with asthma outcomes. The appropriate statistical method should be chosen based on study objectives. In doing so, one must keep in mind that PCA, factor analysis, and cluster analysis identify existing dietary patterns while reduced rank regression is likely to yield useful information for hypothesis generation but may not describe actual intake patterns in the population.Citation58
Second, the heterogeneity of reported results is also possibly attributable to the varied number of confounders controlled for in the studies. For example, the number of confounders controlled for ranged from five to 19 in the observational studies among adults. Confounding could pose challenges for interpretation of the diet–asthma relationship. Nurmatov et alCitation59 have proposed a comprehensive list of primary and secondary confounders that should be considered in future epidemiologic studies examining the early-life diet and asthma relationship in children. The authors suggested that the primary confounders should account for maternal and child characteristics, socioeconomic status, environmental exposures, and dietary factors, while the secondary confounders could be confirmed using appropriate statistical tests. Confounders in the diet–asthma relationship are different between children and adults; therefore, further research is needed to investigate confounders in the adult population. Future observational studies should select confounders based on existing knowledge of the causal mechanism in the diet– asthma relationship and suggestive evidence from statistical analysis. The criteria for selection of confounders should also be reported in observational studies, so readers can be well informed to reach a valid and reliable interpretation of findings.Citation60 In addition, very few population-based studies have been conducted to investigate the association between dietary patterns and asthma outcomes. National survey data (eg, the National Health and Nutrition Examination Survey) may be leveraged to examine the diet–asthma association and identify potential covariates.
Lastly, the inconsistent findings underline the importance of prospective studies and RCTs in helping to better understand the role of dietary patterns in the etiology and disease course of asthma. People’s dietary patterns often change over time through the lifespan and because of changes in socioeconomic and/or health status. Most of the studies reviewed were cross-sectional, precluding investigation of a temporal or causal relationship between dietary patterns and asthma. The cumulative effects of diet on asthma warrant prospective studies. Also, to date, only two RCTs have been designed to evaluate the impact of a healthy dietary pattern on asthma. One is a Mediterranean diet intervention studyCitation21 recently completed in New Zealand and the other is an ongoing Dietary Approaches to Stop Hypertension intervention studyCitation61 in the USA. More experimental studies like these are needed to elucidate the causal relationship.
This systematic review and meta-analysis has a number of strengths and limitations. This is a comprehensive review of the literature on dietary patterns and asthma from 1950 to 2014; however, it was limited to studies published in English. Because of the institutional subscription limitation, we did not include Embase as one of the databases searched for this review. Although Scopus overlaps substantially with Embase,Citation62,Citation63 any studies only indexed in Embase would have been missed. The funnel plots suggested no evidence of publication bias. Nonetheless, the meta-analysis was limited by the abovementioned inherent limitations of individual studies, including a low percentage of total variance explained by the dietary patterns, and inconsistent and possibly incomplete adjustment for potential confounders. Regardless of the limitations, this paper shows that the results of existing studies do not reveal a clear and consistent relationship between dietary patterns and asthma outcomes. Although higher adherence to the Mediterranean diet may be associated with reduced asthma risk in children, more well designed and controlled studies are needed to provide solid evidence and explore whether other healthy dietary patterns are associated with asthma outcomes in children and adults.
Disclosure
The authors report no conflicts of interest in this work.
References
- National Center for Health StatisticsNational Health Interview Survey2001 Available from: http://www.cdc.gov/asthma/nhis/01/table3-1.htmAccessed March 7, 2014
- National Center for Health StatisticsNational Health Interview Survey2012 Available from: http://www.cdc.gov/asthma/nhis/2012/table3-1.htmAccessed March 7, 2014
- MasoliMFabianDHoltSBeasleyRGlobal Initiative for Asthma (GINA) ProgramThe global burden of asthma: Executive Summary of the GINA Dissemination Committee ReportAllergy200459546947815080825
- SkadhaugeLRChristensenKKyvikKOSigsgaardTGenetic and environmental influence on asthma: a population-based study of 11,688 Danish twin pairsEur Respir J199913181410836316
- KimJHEllwoodPEAsherMIDiet and asthma: looking back, moving forwardRespir Res2009104919519921
- Torres-BorregoJMoreno-SolisGMolina-TeranABDiet for the prevention of asthma and allergies in early childhood: much ado about something?Allergol Immunopathol (Madr)201240424425222425606
- AllanKDevereuxGDiet and asthma: nutrition implications from prevention to treatmentJ Am Diet Assoc2011111225826821272700
- AllenSBrittonJRLeonardi-BeeJAAssociation between antioxidant vitamins and asthma outcome measures: systematic review and meta-analysisThorax200964761061919406861
- NurmatovUDevereuxGSheikhANutrients and foods for the primary prevention of asthma and allergy: systematic review and meta-analysisJ Allergy Clin Immunol20111273724733e721e73021185068
- IikuraMYiSIchimuraYEffect of lifestyle on asthma control in Japanese patients: importance of periodical exercise and raw vegetable dietPLoS One201387e6829023874577
- UddenfeldtMJansonCLampaEHigh BMI is related to higher incidence of asthma, while a fish and fruit diet is related to a lower– results from a long-term follow-up study of three age groups in SwedenRespir Med2010104797298020171076
- WoodsRKThienFCAbramsonMJDietary marine fatty acids (fish oil) for asthma in adults and childrenCochrane Database Syst Rev20023CD00128312137622
- MilanSJHartAWilkinsonMVitamin C for asthma and exercise-induced bronchoconstrictionCochrane Database Syst Rev201310CD01039124154977
- Garcia-MarcosLCastro-RodriguezJAWeinmayrGPanagiotakosDBPriftisKNNagelGInfluence of Mediterranean diet on asthma in children: a systematic review and meta-analysisPediatr Allergy Immunol201324433033823578354
- MoherDLiberatiATetzlaffJAltmanDGGroupPPreferred reporting items for systematic reviews and meta-analyses: the PRISMA statementJ Clin Epidemiol200962101006101219631508
- Academy of Nutrition and DieteticsEvidence Analysis Manual: Steps in the Academy Evidence Analysis ProcessChicago, IL, USAADA Research and Strategic Business Development2012
- SheuCFSuzukiSMeta-analysis using linear mixed modelsBehav Res Methods2001332102107
- BeggCBMazumdarMOperating characteristics of a rank correlation test for publication biasBiometrics1994504108811017786990
- Sanchez-SolisMValverde-MolinaJPastorMDMediterranean diet is a protective factor for asthma in children 6–8 years oldEur Respir J200650Suppl850s
- BakolisIHooperRThompsonRLShaheenSODietary patterns and adult asthma: population-based case-control studyAllergy201065560661519845575
- SextonPBlackPMetcalfPInfluence of Mediterranean diet on asthma symptoms, lung function, and systemic inflammation: a randomized controlled trialJ Asthma2013501758123157561
- RosenkranzRRRosenkranzSKNeessenKJDietary factors associated with lifetime asthma or hayfever diagnosis in Australian middle-aged and older adults: a cross-sectional studyNutr J2012118423057785
- HooperRHeinrichJOmenaasEDietary patterns and risk of asthma: results from three countries in European Community Respiratory Health Survey-IIBr J Nutr201010391354136519995472
- ShaheenSOJamesonKASyddallHEThe relationship of dietary patterns with adult lung function and COPDEur Respir J201036227728420075056
- BarrosRMoreiraAFonsecaJAdherence to the Mediterranean diet and fresh fruit intake are associated with improved asthma controlAllergy200863791792318588559
- McKeeverTMLewisSACassanoPAPatterns of dietary intake and relation to respiratory disease, forced expiratory volume in 1 s, and decline in 5-y forced expiratory volumeAm J Clin Nutr201092240841520554789
- VarrasoRKauffmannFLeynaertBDietary patterns and asthma in the E3N studyEur Respir J2009331334118829673
- VarrasoRFungTTBarrRGHuFBWillettWCamargoCAJrProspective study of dietary patterns and chronic obstructive pulmonary disease among US womenAm J Clin Nutr200786248849517684223
- VarrasoRFungTTHuFBWillettWCamargoCAProspective study of dietary patterns and chronic obstructive pulmonary disease among US menThorax200762978679117504819
- ButlerLMKohWPLeeHPProspective study of dietary patterns and persistent cough with phlegm among Chinese SingaporeansAm J Respir Crit Care Med2006173326427016239624
- ShiZYuanBWittertGAMonosodium glutamate intake, dietary patterns and asthma in Chinese adultsPLoS One2012712e5156723240044
- TrompIIKiefte-de JongJCde VriesJHDietary patterns and respiratory symptoms in pre-school children: the Generation R StudyEur Respir J201240368168922362860
- RomieuIBarraza-VillarrealAEscamilla-NunezCDietary intake, lung function and airway inflammation in Mexico City school children exposed to air pollutantsRespir Res200910112220003306
- GrigoropoulouDPriftisKNYannakouliaMUrban environment adherence to the Mediterranean diet and prevalence of asthma symptoms among 10- to 12-year-old children: the Physical Activity, Nutrition, and Allergies in Children Examined in Athens studyAllergy Asthma Proc201132535135822195687
- Gonzalez BarcalaFJPertegaSBamondeLMediterranean diet and asthma in Spanish schoolchildrenPediatr Allergy Immunol20102171021102720561232
- ArvanitiFPriftisKNPapadimitriouAAdherence to the Mediterranean type of diet is associated with lower prevalence of asthma symptoms, among 10–12 years old children: the PANACEA studyPediatr Allergy Immunol201122328328921457335
- Castro-RodriguezJAGarcia-MarcosLAlfonseda RojasJDValverde-MolinaJSanchez-SolisMMediterranean diet as a protective factor for wheezing in preschool childrenJ Pediatr20081526823828e821e82218492525
- ChatziLTorrentMRomieuIMediterranean diet in pregnancy is protective for wheeze and atopy in childhoodThorax200863650751318198206
- ChatziLApostolakiGBibakisIProtective effect of fruits, vegetables and the Mediterranean diet on asthma and allergies among children in CreteThorax200762867768317412780
- Garcia-MarcosLCanflancaIMGarridoJBRelationship of asthma and rhinoconjunctivitis with obesity, exercise and Mediterranean diet in Spanish schoolchildrenThorax200762650350817251311
- de Cassia Ribeiro SilvaRAssisAMCruzAADietary patterns and wheezing in the midst of nutritional transition: a study in BrazilPediatr Allergy Immunol Pulmonol2013261182423555072
- de BatlleJGarcia-AymerichJBarraza-VillarrealAAntoJMRomieuIMediterranean diet is associated with reduced asthma and rhinitis in Mexican childrenAllergy200863101310131618782109
- LeeSCYangYHChuangSYLiuSCYangHCPanWHRisk of asthma associated with energy-dense but nutrient-poor dietary pattern in Taiwanese childrenAsia Pac J Clin Nutr2012211738122374563
- NagelGWeinmayrGKleinerAGarcia-MarcosLStrachan DP; GroupIPTSEffect of diet on asthma and allergic sensitisation in the International Study on Allergies and Asthma in Childhood (ISAAC) Phase TwoThorax201065651652220522849
- ChatziLGarciaRRoumeliotakiTMediterranean diet adherence during pregnancy and risk of wheeze and eczema in the first year of life: INMA (Spain) and RHEA (Greece) mother-child cohort studiesBr J Nutr2013110112058206823680284
- Castro-RodriguezJAGarcia-MarcosLSanchez-SolisMPerez-FernandezVMartinez-TorresAMallolJOlive oil during pregnancy is associated with reduced wheezing during the first year of life of the offspringPediatr Pulmonol201045439540220306538
- ShaheenSONorthstoneKNewsonRBEmmettPMSherriffAHendersonAJDietary patterns in pregnancy and respiratory and atopic outcomes in childhoodThorax200964541141719213776
- LangeNERifas-ShimanSLCamargoCAJrGoldDRGillmanMWLitonjuaAAMaternal dietary pattern during pregnancy is not associated with recurrent wheeze in childrenJ Allergy Clin Immunol20101262250255e251e25420584543
- MiyakeYOkuboHSasakiSTanakaKHirotaYMaternal dietary patterns during pregnancy and risk of wheeze and eczema in Japanese infants aged 16–24 months: the Osaka Maternal and Child Health StudyPediatr Allergy Immunol201122773474121539616
- AllanKKellyFJDevereuxGAntioxidants and allergic disease: a case of too little or too much?Clin Exp Allergy201040337038019968654
- VarrasoRNutrition and asthmaCurr Allergy Asthma Rep201212320121022407651
- HuFBDietary pattern analysis: a new direction in nutritional epidemiologyCurr Opin Lipidol20021313911790957
- MartinezMEMarshallJRSechrestLInvited commentary: factor analysis and the search for objectivityAm J Epidemiol1998148117199663398
- US Department of Health and Human Services, US Department of Agriculture2010Dietary Guidelines for Americans2011 Available from: http://www.cnpp.usda.gov/dietaryguidelines.htmlAccessed December 17, 2013
- KennedyETOhlsJCarlsonSFlemingKThe Healthy Eating Index: design and applicationsJ Am Diet Assoc19959510110311087560680
- BarbareskoJKochMSchulzeMBNothlingsUDietary pattern analysis and biomarkers of low-grade inflammation: a systematic literature reviewNutr Rev201371851152723865797
- FungTTBrownLSDietary patterns and the risk of colorectal cancerCurr Nutr Rep201321485524496398
- TuckerKLDietary patterns, approaches, and multicultural perspectiveAppl Physiol Nutr Metab201035221121820383235
- NurmatovUNwaruBIDevereuxGSheikhAConfounding and effect modification in studies of diet and childhood asthma and allergiesAllergy20126781041105922712878
- von ElmEAltmanDGEggerMStrengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studiesBMJ2007335762480680817947786
- MaJStrubPLavoriPWDASH for asthma: a pilot study of the DASH diet in not-well-controlled adult asthmaContemp Clin Trials2013352556723648395
- ElsevierTraining and Support. Frequently asked questions Available from: http://www.elsevier.com/online-tools/embase/training-and-supportAccessed April 29, 2014
- BurnhamJFScopus database: a reviewBiomed Digit Libr20063116522216
Appendix
Appendix 1 Search strategy