
Abstract
Purpose
Asthma is a global health problem, and asthma prevalence in Asia is increasing. The REcognise Asthma and LInk to Symptoms and Experience Asia study assessed patients’ perception of asthma control and attitudes toward treatment in an accessible, real-life adult Asian population.
Patients and methods
An online survey of 2,467 patients with asthma from eight Asian countries/regions, aged 18–50 years, showed greater than or equal to two prescriptions in previous 2 years and access to social media. Patients were asked about their asthma symptoms, exacerbations and treatment type, views and perceptions of asthma control, attitudes toward asthma management, and sources of asthma information.
Results
Patients had a mean age of 34.2 (±7.4) years and were diagnosed with asthma for 12.5 (±9.7) years. Half had the Global Initiative for Asthma-defined uncontrolled asthma. During the previous year, 38% of patients visited the emergency department, 33% were hospitalized, and 73% had greater than or equal to one course of oral corticosteroids. About 90% of patients felt that their asthma was under control, 82% considered their condition as not serious, and 59% were concerned about their condition. In all, 66% of patients viewed asthma control as managing attacks and 24% saw it as an absence of or minimal symptoms. About 14% of patients who correctly identified their controller inhalers had controlled asthma compared to 6% who could not.
Conclusion
Patients consistently overestimated their level of asthma control contrary to what their symptoms suggest. They perceived control as management of exacerbations, reflective of a crisis-oriented mind-set. Interventions can leverage on patients’ trust in health care providers and desire for self-management via a new language to generate a paradigm shift toward symptom control and preventive care.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Keywords:
Introduction
Asthma is a global health problem and afflicted 334 million people worldwide in 2014.Citation1 It is more pronounced in parts of Asia, with 107 million sufferers in Southeast Asia and Western Pacific Region.Citation2,Citation3 Asthma also presents an economic cost: directly from hospitalization, treatment, and health care resources and indirectly from time lost from work, absenteeism, and premature death. In 2006, annual per patient direct cost of treatment ranged from USD108 to USD1,010 and constituted about 13.0% of the per capita GDP of countries in the Asia-Pacific.Citation4 The cost of uncontrolled asthma was estimated to be 1.51 times that of the controlled diseaseCitation4 and highlighted the need for better disease management if countries were to rein in the burden of caring for asthma patients.
The 2012 REcognise Asthma and LInk to Symptoms and Experience (REALISE) survey was the largest appraisal of asthma patients in Europe.Citation5 It showed that asthma control remained poor, and many patients perceived their asthma to be controlled and not serious despite the presence of symptoms and exacerbations. Furthermore, the optimal levels of asthma control achieved in clinical studies were often not replicated in real-life studies.Citation6 Real-life studies revealed that asthma control when assessed according to international guidelines, such as the Global Initiative for Asthma (GINA),Citation7 was poor, and this was attributed to a complex interaction of guidelines and disease-, patient-, and doctor-related factors. Many patients felt least informed about the meaning of asthma control.Citation6
While the overall prevalence of asthma in the Asian adult population (<5%) was lower than that in European populations, temporal studies of asthma prevalence in several developed Asian countries revealed a rising trend.Citation8 Asthma control in Asia remained low despite the availability of efficacious treatments. Earlier Asian studies of asthma patients were conducted through face-to-face or phone interviews and mainly addressed the burden of disease and patient’s reactions to exacerbations.Citation9–Citation11 Where available, results showed that patients often overestimated their level of control and the situation has not improved in recent years.Citation9 Earlier studies, including REALISE, used guidelines such as GINA to determine the level of control and did not seek the patient’s view of asthma control. This study, REALISE Asia, focused on patients’ perceptions of asthma control and their attitudes toward the disease and its treatment in an accessible, real-life adult Asian population. It used an online survey to seek eligible respondents from validated consumer panels who used social media to broaden the coverage and reach to the patients.
Materials and methods
Study design
REALISE Asia was a quantitative, online questionnaire-based survey, which used a similar methodology as REALISE.Citation5 The questionnaire from REALISE compared asthma symptoms and indicators of acute exacerbations across guideline-defined control levelsCitation7 and treatment types, investigated patients’ perceptions of asthma and attitudes toward asthma management, and identified that their sources of information had been cognitively tested and contained many validated elements. Our study’s working group, consisting of practicing physicians and respiratory specialists, made revisions to the original questionnaire (permission granted, see Supplementary material), taking into consideration the local context (eg, the use of Weibo in People’s Republic of China) and asking the patients what the term “well-controlled asthma” meant to them. A field-test of the questionnaire was carried out with ten respondents per country prior to the survey. The results were analyzed, and minor amendments to the questionnaire were made for clarity.
Survey population
Recruitment was done via a simple random sample of individuals aged 18–50 years from validated consumer panelsCitation12 in People’s Republic of China, Hong Kong, Indonesia, Korea, Malaysia, Philippines, Singapore, and Taiwan. Email invites were sent to these individuals between December 2013 and March 2014 asking them to complete a 30-minute online questionnaire (Supplementary material). As there were no hospital/physician associations or referrals, approvals from institutional review boards were not required. The survey was conducted according to the International Chamber of Commerce/European Society for Opinion and Market Research (ICC/ESOMAR) International Code on Market and Social Research,Citation13 which sets out ethical principles for the conduct of market research. Patient informed consent was also obtained from each respondent.
The sample size was based on factors, including population size and implementation cost, within 4%–8% error margin at 95% confidence level.Citation14 The inclusion criteria were patients aged 18–50 years who were diagnosed with asthma, given greater than or equal to two asthma-related prescriptions in the past 2 years (to ensure that patients have active asthma), and had used social media. Respondents who were employed; had relatives employed in the health care, pharmaceutical, advertising, or market research industries; or had taken part in health care-related market research in the past 3 months were excluded.
Data collection
Respondents were allowed to answer the questionnaire once. Data quality checks included confirming responses and weeding out unusual or illogical answers. Questions were designed to sieve out inconsistent or fraudulent responses, and some items were repeated for consistency and verification. Responses in the local language were interpreted and translated back to English. The working group reviewed and approved the translated materials.
Data analysis
Responses to the questionnaire were analyzed for the total eligible population. Answers relating to asthma symptoms and indicators of acute exacerbations were analyzed by GINA-defined control levelsCitation7 and treatment type. Symptoms assessed were daytime asthma symptoms, night waking, activity limitation due to asthma, and reliever useCitation15 during the past 7 days, and indicators were corticosteroids and antibiotics use, days off work, emergency department (ED) admissions, and hospitalizations. Perceptions assessed were asthma control (controlled/uncontrolled) and seriousness and concern of disease (on a 4-point scale). Attitudes were assessed on the patient’s agreement (on a 4-point scale) to statements on asthma. Patient’s views (in text) of asthma control were categorized by key messages and information sources by the frequency of selection. Tests of statistical significance were performed with Fisher’s exact test.Citation16
Results
Demographics and clinical characteristics
A total of 71,002 individuals started the questionnaire. Of them, 49,409 who did not meet the inclusion criteria and 18,672 who did not complete the survey were excluded. The most common exclusion reason was that they did not have asthma (75.6%, n=37,505). Among the eligible respondents, 454 failed data quality checks and were excluded. The final analysis set contained 2,467 patients (). The largest group was from People’s Republic of China (32.4%), followed by South Korea (20.3%) and Taiwan (12.2%). presents their demographic and clinical characteristics. The mean age of asthma patients was 34.2 (±7.4) years. Both sexes were equally represented. They had been diagnosed with asthma for 12.5 (±9.7) years. Nine of ten patients were taking medication for their asthma, and 35.3% of them used a reliever and 16.5% used a controller. About 11.5% of the patients were current smokers.
Figure 1 Survey flowchart.
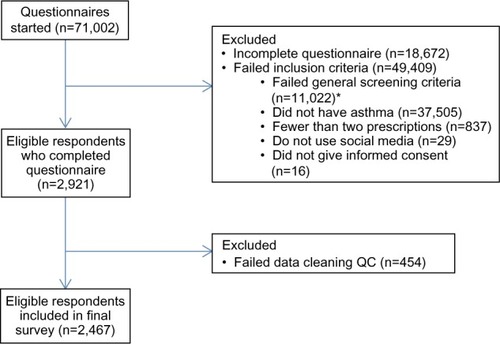
Table 1 Demographics and other clinical characteristics
Asthma control and symptoms
Using the GINA-defined criteria,Citation7 17.8% (440), 32.5% (802), and 49.7% (1,225) of patients had controlled, partially controlled, and uncontrolled asthma, respectively (). In the week before the survey, 38.2% of patients experienced asthma symptoms for >2 days, 64.2% indicated that symptoms interfered with their normal activities, and 71.2% had night awakenings due to asthma. Of the 1,887 patients who owned a reliever inhaler, 45.2% used it greater than or equal to two times during the same period. In the year prior to the survey, 38.4% of patients visited the ED and 33.1% were hospitalized for asthma. Most (76.5%) patients required greater than or equal to one course of antibiotics to treat health problems related to asthma and 73.1% had greater than or equal to one course of corticosteroids for worsening asthma during the past year. Two of three patients missed work because of asthma. Patients with controlled asthma also experienced acute exacerbations in the previous year. They were mostly treated with antibiotics (56.1%) or oral corticosteroids (46.8%).
Table 2 Asthma symptoms and indicators of exacerbations overall and by GINA-defined control levelsCitation7
Asthma symptoms and indicators of exacerbations by treatment types
shows the asthma symptoms and indicators of acute exacerbations by treatment types. Patients who were prescribed reliever-only or controller-only inhalers tended to have less symptoms compared to those on multiple therapies. Similar results were also obtained for the indicators of exacerbations. About four to five of ten patients who were prescribed relievers had used them greater than two times a week.
Table 3 Asthma symptoms and indicators of exacerbations by treatment types
Patients’ perceptions of asthma
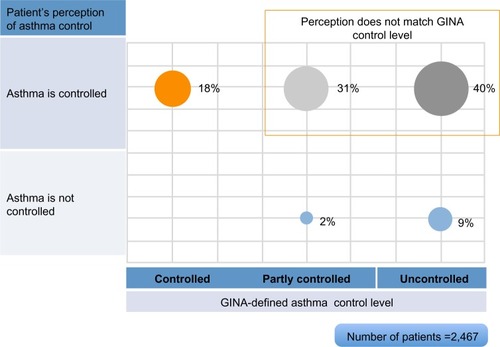
describes the patients’ view of asthma control. Two-thirds of patients related control to managing attacks: attacks are controllable with medical help (28.2%), no or reduced attacks (16.3%), prevention of attacks through medicines (10.6%), or lifestyle modification, eg, avoidance of triggers (10.4%). About 24.1% saw it as minimal symptoms or impact on normal activities. relates the patients’ perception of asthma to their condition as defined by the GINACitation7 guidelines.
Figure 2 Perceptions of asthma control.
Abbreviations: TCM, traditional Chinese medicine; w/o, without.
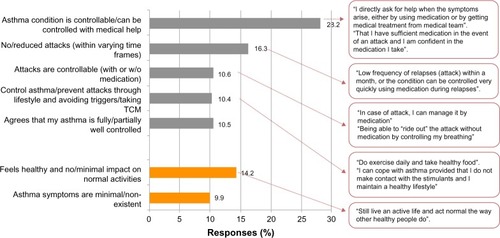
Figure 3 Perception of vs GINA-defined asthma control.
Abbreviation: GINA, Global Initiative for Asthma.
When asked about their asthma, 89.1% of patients felt that it was under control and 81.5% felt that it was not serious (). Patients with uncontrolled asthma also felt no differently (cf, 81.6% and 70.1%, respectively), but were more concerned about their condition than those with controlled asthma (58.7% vs 21.6%). For patients who experienced acute exacerbations requiring a visit to the ED or hospitalization, a smaller percentage compared to the overall population felt that their asthma was under control (83.5%, 82.5% vs 89.1%) or not serious (70.2%, 66.8% vs 81.5%). A higher percentage of them were also concerned about their asthma (60.3%, 63.3% vs 45.6%).
Table 4 Patients’ perceptions of asthma by GINA-defined control levelsCitation7 and indicators of acute exacerbations
Attitudes toward asthma and its management
shows the patient’s attitudes toward asthma in daily life. They felt that they should fit in with people around them (88.7%) and did not want to be labeled as sick (85.0%) or think about their asthma (70.0%). They also trusted their doctors and followed their instructions to manage their condition (86.8%). These percentages were similar across all the control levels. More patients with well-controlled asthma felt healthy and fit compared to those with uncontrolled asthma (82.0% vs 62.4%, P<0.01). They viewed their condition as different from sufferers with uncontrolled asthma (72.0% vs 60.7%, P<0.01). When asked if they were worried about their condition in 10 years, more patients with uncontrolled asthma agreed compared to patients with controlled asthma (72.0% vs 42.7%, P<0.01).
Table 5 Patients’ attitude toward asthma in daily life
About half of all patients agreed with statements that having inhalers was embarrassing or a nuisance. Patients with uncontrolled asthma, in particular, felt that it was an embarrassment (62.0%) or nuisance (52.2%) to use an inhaler or even carry one (56.7%) in public.
Attitudes toward controller inhalers
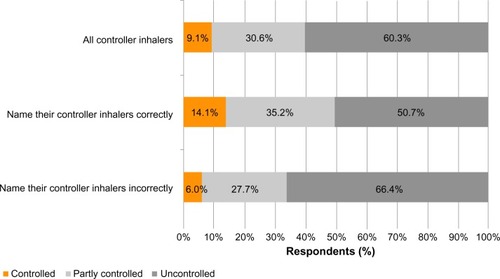
Most patients (52.8%) were aware of the need to use controller inhaler regularly to control their asthma. When asked about their controller inhalers, 19.9% of patients identified them correctly, 31.3% incorrectly, and the rest did not know. shows the frequency of controller inhaler usage in the week prior to the survey. About 13.9% of patients used it daily and 42.8% used it on some days. Of those who answered correctly, 30.0% used them daily compared to 16.7% who could not (P<0.01). The 14.1% of patients who correctly named their controller inhalers had controlled asthma compared to 6.0% of those who could not (P<0.01, ).
Figure 4 Frequency of use of controller inhalers.
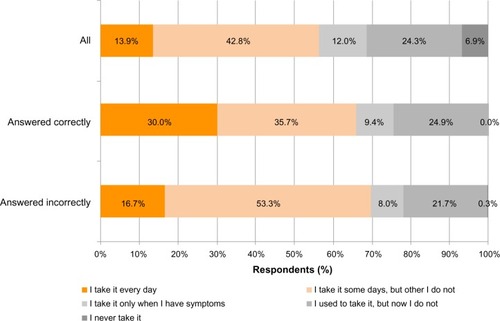
Figure 5 Knowledge of controller inhalers.
Sources of asthma information
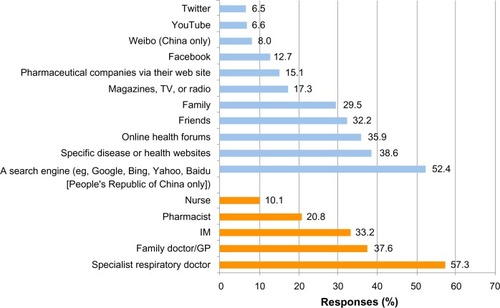
Nine-tenths of patients actively looked for information about asthma and one-third, at least once a week. Patients searched for information on asthma attack prevention, what makes asthma worse or can trigger attacks and what to do in an event of an asthma attack. shows the sources of asthma information. Online sources and health care professionals (HCPs) were cited in 42.5% and 38.4% of the responses, respectively. Health care professionals were considered trustworthy information sources and consisted of respiratory specialists (57.3% of patients), family physicians/general practitioners (37.6%), and internal medicine specialists (33.2%). Other sources of information include health websites (38.6%), online health forums (35.9%), friends (32.2%), and family (29.5%).
Figure 6 Sources of asthma information.
Abbreviations: IM, internal medicine; GP, general practitioner.
Discussion
Our study showed that patient knowledge of asthma control and inhaler medication is low. Our patients viewed asthma control as being able to manage or relieve the exacerbations or attacks instead of preventing them. This was seen in the way they understood the concept of asthma control and reflected in their medication usage: reliever users outnumbered controller users by 2:1. In addition, about half the reliever users had a high frequency of use (greater than two times per week). This suggested that the level of control could have been underestimated and the prescribed therapy was inadequate, not taken, or not appropriate. Asthma management was crisis-oriented through the widespread use of oral corticosteroids and antibiotics and emergency care – ED visits or hospitalization. Despite this, most patients held on to the belief that their asthma was not serious and under control. As a result, the level of control remained low and <one-fifth of our patients achieved GINA-defined controlled asthma.
Many patients were concerned about their condition, especially those who had experienced acute exacerbations. The knowledge of controller inhalers was low, and only one-fifth of users could correctly identify their medication. Although they understood the preventive value of the inhaler and those who use it required the least hospitalizations or ED visits, many did not use it daily citing embarrassment and nuisance as reasons for not using them. Addressing these issues could improve treatment adherence as patients who correctly identified their inhaler medication had better asthma control.
Many patients expressed confidence in their HCPs and followed their instructions. HCPs are, thus, well placed to help their patients resolve issues about their disease and its management. A study of patient–physician communication and patients’ knowledge about asthma in ItalyCitation17 showed that 28.5% of general practitioners did not encourage patients to express doubts, expectations, or concerns and that 36.9% were unlikely to involve the patient in asthma management. Our patients used social media and searched online for information, and their enquiries revealed a desire to self-manage their asthma. The Internet provides an excellent opportunity to augment the delivery of asthma management information through online channels, such as search engines, health-related websites, and health forums.
Our survey relied on patients’ responses to the online questionnaire. These responses could not be clinically verified, and some patients might have inaccurately recalled certain events. Our respondents were patients who used social media and may not represent the cross-section of the asthmatic population. Compared to other Asian studiesCitation9–Citation11 that utilized face-to-face or phone interviews, the lower average age (34.2 years vs 40.5–45.0 years) and smaller female representation (46.3% vs 54.0%–57.5%) reflect the younger, male-predominant online population of our patients. REALISECitation5 patients also had a lower average age. However, clinical findings such as daytime symptoms or seeking help at EDs was consistent with these studies (38.2% vs 23.9%–57.8% and 38.4% vs 40.0%–42.7%, respectively).Citation5,Citation9–Citation11 Our study population and that of REALISECitation5 also had higher percentages of patients with controlled asthma (18%–20% vs 2%–3%).Citation7–Citation9 These two populations could have better access to asthma information and put them at an advantage compared to the general asthma population. Segmentation of patients could provide further insights of their attitudes on asthma control, given the disparities in socioeconomic status of patients in different countries of multicultural Asia.
Implications of results for asthma management policy and practice
Our study revealed a crisis-oriented approach to asthma management: high reliever and oral corticosteroid use, ED visits, and hospitalizations. This mind-set is similarly evident in how patients understand the concept of well-controlled asthma. Asthma management strategies need to evolve from relief to prevention. As patients are not always able to understand asthma control, HCPs are best positioned to educate patients on their condition, address the perception discrepancy, help patients overcome their anxieties, and influence their attitudes toward treatment. Patient education, however, needs a new language to promote a shared understanding of asthma control between patients and physicians.
Conclusion
Patients consistently overestimate their level of asthma control rather than what their clinical symptoms suggest. This discrepancy may be due to the patients’ perception that asthma control is about managing exacerbations instead of achieving a predefined level of symptom control. Patients also expressed concern about their asthma and sought information on how to manage their condition. Interventions to address patients’ perception of asthma control and attitudes toward the use of controller inhalers can leverage on their confidence in their HCPs and desire for better self-management. A new language to communicate the guideline-defined asthma control and promote the preventive use of controller medication is needed.
Author contributions
All the authors were involved in conceptualizing the study design, drafting the article, or revising it critically for important intellectual content, and all the authors approved the final version to be submitted for publication. All the authors have full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Acknowledgments
This study was supported and funded by Mundipharma Pte Ltd. Online survey and statistical analysis were performed by Pei-Li Teh, Rachel Howard, Tsin-Li Chua, and Jie Sun of Research Partnership Pte Ltd. Medical writing support was provided by Sen-Kwan Tay of Research2Trials Clinical Solutions Pte Ltd.
Disclosure
The authors received honoraria from Mundipharma for their participation in the REALISE Asia Working Group meetings and discussions. Professor Price has board membership with Mundipharma and also received speaker fees, grants, and unrestricted funding support from Mundipharma. Professors Liam and Yunus and Associate Professor David-Wang and Assistant Professor Tan are members of the Asia-Pacific Advisory Board of Mundipharma. Professors Cho and Yunus and Associate Professor David-Wang and Assistant Professor Tan received speaker fees from Mundipharma in the past. Assistant Professor Tan received conference sponsorship from Mundipharma. Dr Neira is an employee of Mundipharma. The authors have no other conflicts of interest in this work.
References
- Global Asthma Network (GAN)The Global Asthma Report 20142014 Available from: http://www.globalasthmareport.org/burden/burden.phpAccessed March 25, 2015
- AahmanEBeggSBlackBThe Global Burden of Disease: 2004 Update. World Health Organisation Available from: http://www.who.int/healthinfo/global_burden_disease/2004_report_update/en/Accessed February 10, 2015
- LaiCKBeasleyRCraneJGlobal variation in the prevalence and severity of asthma symptoms: phase three of the International Study of Asthma and Allergies in Childhood (ISAAC)Thorax20096447648319237391
- LaiCKimYYKuoSHSpencerMWilliamsAEon behalf of the Asthma Insights and Reality in Asia Pacific Steering CommitteeCost of asthma in the Asia-Pacific regionEur Respir Rev2006151016
- PriceDFletcherMvan der MolenTAsthma control and management in 8,000 European patients: the recognise asthma and link to symptoms and experience (REALISE) surveyNPJ Prim Care Respir Med2014241400924921985
- BraidoFFailure in asthma control: reasons and consequencesScientifica2013201354925224455432
- http://www.ginasthma.org[homepage on the Internet], The Global Initiative for Asthma (GINA) Science CommitteeGlobal Strategy for Asthma Management and Prevention2014 Available from: http://www.ginasthma.org/documents/4Accessed November 12, 2014
- SongWJKangMGChangYSChoSHEpidemiology of adult asthma in Asia: toward a better understandingAsia Pac Allergy20144758524809012
- ThompsonPJSalviSLinJInsights, attitudes and perceptions about asthma and its treatment: findings from a multinational survey of patients from 8 Asia-Pacific countries and Hong KongRespirology20131895796723730953
- LaiCKKoFWBhomeARelationship between asthma control status, the asthma control test and urgent health-care utilization in AsiaRespirology20111668869721362102
- ZainudinBMLaiCKSorianoJBJia-HorngWDe GuiaTSAsthma Insights and Reality in Asia-Pacific Steering CommitteeAsthma control in adults in Asia-PacificRespirology20051057958616268910
- LightspeedGMILightspeed GMI Quality Suite. How We Do It: Ensuring Unique Responses2015 Available from: http://www.lightspeedgmi.com/services/lightspeed-gmi-quality-suite/Accessed March 30, 2015
- http://www.esomar.org[homepage on the Internet]European Society for Opinion and Market Research (ESOMAR)ICC/ESOMAR International Code on Market and Social Research2008 Available from: http://www.esomar.org/knowledge-and-standards/codes-and-guidelines.phpAccessed August 25, 2014
- http://www.raosoft.comRaosoft, Inc. [homepage on the Internet]Raosoft Sample Size Estimator2004 Available from: http://www.raosoft.com/samplesize.htmlAccessed December 16, 2014
- iharp.org [homepage on the Internet]Optimum Patient CareiHARP: Inhaler Technique Assessment Initiative Helping Asthma in Real-life Patients Available from: http://iharp.org/questionnaire.aspxAccessed October 3, 2014
- research.microsoft.com [homepage on the Internet], Microsoft ResearchFisher’s Exact Test Calculator for 2×2 Contingency Tables2014 Available from: http://research.microsoft.com/en-us/um/redmond/projects/mscompbio/fisherexacttest/Accessed December 18, 2014
- BraidoFBaiardiniIMenoniSAsthma management failure: a flaw in physicians’ behavior or in patients’ knowledge?J Asthma20114826627421381864