
Abstract
Purpose
Hemophagocytic lymphohistiocytosis (HLH) is a potentially lethal hyperinflammatory disorder. For further understanding of the pathogenesis of HLH, we examined serum levels of high mobility group box protein 1 (HMGB1) in children with HLH.
Patients and methods
Serum HMGB1 levels were measured in 28 patients with HLH and 6 normal controls using a quantitative enzyme-linked immunosorbent assay. The patients were 21 boys and 7 girls, aged from 10 days to 21 years, with a median age of 8.5 years. The underlying conditions of HLH were infection-associated HLH in 18 patients, malignancy-associated HLH in 7 patients, and genetic HLH in 3 patients. The relations between serum HMGB1 levels and clinical symptoms and laboratory parameters were analyzed.
Results
Serum HMGB1 levels were significantly higher in patients with HLH than in normal controls (median, 6.5 ng/mL, interquartile range, 4.25–13.1). The serial serum HMGB1 levels in one patient fell to reflect the disease activity. Serum HMGB1 levels were significantly higher in patients with disseminated intravascular coagulation (DIC) than in patients without DIC (p<0.001) and were also significantly higher in patients with central nervous system (CNS) complications than in patients without CNS complications (p<0.01). Serum HMGB1 levels were positively correlated with aspartate aminotransferase (rs =0.48, p<0.01, Spearman’s rank correlation coefficient) and negatively correlated with fibrinogen (rs = −0.475, p=0.011) and hemoglobin (rs = −0.465, p=0.013).
Conclusion
Serum HMGB1 levels reflect clinical features of childhood HLH. HMGB1 is a potential mediator involved in the pathogenesis and determining the clinical findings of HLH.
Introduction
High mobility group box protein 1 (HMGB1) is a nonhistone nuclear protein that has a dual function.Citation1 Inside the cell, HMGB1 binds DNA, regulating transcription and determining chromosomal architecture. In the extracellular milieu, HMGB1 is known as a prototypical alarmin activating inflammation and innate immunity,Citation2 which was first identified as a novel lethal mediator of sepsis.Citation3 HMGB1 can be released actively from innate immune cells in response to pathogenic products and passively from injured or dying cells. Until now, HMGB1 has been reported to be involved in the pathophysiology of various infectious and noninfectious inflammatory disorders.Citation4
Hemophagocytic lymphohistiocytosis (HLH) is a life-threatening hyperinflammatory syndrome. Hypercytokinemia secreted from dysregulated hyperactivated monocytes, macrophages, T cells and NK cells has been reported to play a major role in HLH.Citation5 It has been recently revealed that alarmin and innate immunity play an important role in the pathogenesis of both primary and secondary HLH.Citation6,Citation7 There have been only three reports of serum or plasma HMGB1 levels in patients with HLH or macrophage activation syndrome,Citation8–Citation10 and further investigations are needed to define the involvement of HMGB1 in the pathophysiology of HLH.
In this study, we examined serum levels of HMGB1 in 28 children with HLH and analyzed their relation to clinical symptoms and laboratory parameters.
Materials and methods
Patients
Serum HMGB1 levels were analyzed in 28 patients who were diagnosed as having HLH in the Wakayama Medical University Hospital between 2006 and 2016 according to the diagnostic criteria of HLH 2004.Citation11 We also analyzed blood samples from six, healthy five-year-old children who underwent a preschool check-up. Written informed consent was obtained from their guardians. This study was approved by the institutional review board. The study was explained to the patients and their guardians, and a Website with additional information and including an opt-out option was set up for the study. Clinical data about patient characteristics, underlying conditions and triggers for HLH, clinical symptoms, laboratory parameters at the time of HLH diagnosis, and outcome were collected by reviewing the patients’ medical records. Central nervous system (CNS) complications were defined by altered consciousness level or seizures. Disseminated intravascular coagulation (DIC) was diagnosed by the Japanese Ministry of Health and Welfare DIC criteria.Citation12 Respiratory complications were defined by the need for oxygen inhalation. Infections were diagnosed by microbiological, serological, or molecular biological methods.
Measurement of HMGB1
Blood samples were collected from the patients at the time of diagnosis of HLH and before specific treatment for HLH. Serial serum HMGB1 levels were measured in one patient. Whole blood collected in nonheparinized tubes was left to clot at room temperature for 30 min before centrifugation at 3000 rpm for 15 min. The serum fractions were stored at −80 °C until the time of assay. Serum HMGB1 concentrations were determined using a quantitative enzyme-linked immunosorbent assay (Shino-Test Corporation, Tokyo, Japan). We also analyzed blood samples from six healthy children.
Statistical analysis
Continuous variables (serum HMGB1 levels and laboratory parameters) are presented as medians and interquartile ranges. The Mann–Whitney U test was used to test for differences. We considered p<0.05 to indicate a statistically significant difference. Correlations with serum HMGB1 levels and laboratory parameters were expressed by Spearman’s rank correlation coefficient, where rs >0.4 was considered to indicate a significant correlation. All statistical analyses were performed with EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (The R foundation for Statistical Computing, Vienna, Austria).Citation13
Results
Patient characteristics
Patient characteristics and clinical symptoms are shown in . The patients were 21 boys and 7 girls, aged from 10 days to 21 years, with a median age of 8.5 years. The underlying conditions of HLH were infection-associated HLH in 18 patients, malignancy-associated HLH in 7 patients (subdivided into two categories: 2 with malignancy-triggered HLH and 5 with HLH during chemotherapy),Citation14 and genetic HLH in 3 patients. All patients were treated with immunosuppressive drugs and intensive support therapy. One patient (patient 9) died of multiple organ failure, and one patient (patient 23) died of acute respiratory distress syndrome.
Table 1 Patients characteristics, clinical symptoms, and serum HMGB1 levels
Serum HMGB1 levels
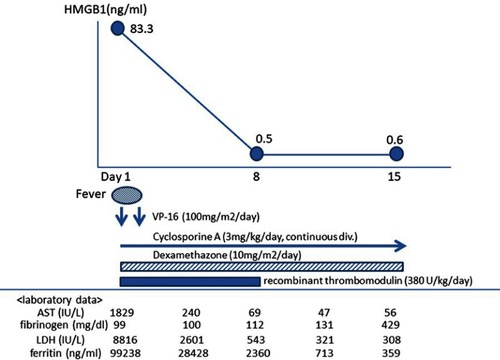
Serum HMGB1 levels in patients with HLH are shown in . The levels were significantly higher in patients with HLH than in normal controls (median [mini–max] 6.5 [1.1–574] vs 0.25 [0.2–0.4], p<0.01). The serum HMGB1 levels in patient 4 fell to reflect the disease activity (). The serum HMGB1 levels did not significantly differ among the individual types of HLH. Strikingly high levels of HMGB1 (>100 ng/mL) were seen in 3 of the 28 patients (11%): patient 6, 24, and 26.
Figure 1 Clinical course of patient 4: Epstein-Barr virus infection-associated hemophagocytic lymphohistiocytosis.
HMGB1 and clinical symptoms
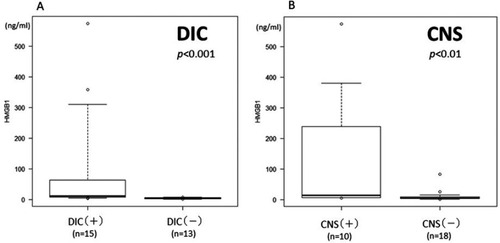
CNS complications and DIC were seen in 10 (35.7%) and 15 (53.6%) patients, respectively (). Serum HMGB1 levels were significantly higher in patients with DIC than in patients without DIC and were also significantly higher in patients with CNS complications than in those without CNS complications (). Among the patients with strikingly high HMGB1 levels, patient 6 had complicated mild leukoencephalopathy revealed by magnetic resonance imaging (MRI) and required exchange transfusion in addition to methylprednisolone pulse therapy. Patient 24 had complicated moderate leukoencephalopathy resulting in CNS sequelae and required mechanical ventilation and hemodialysis. Serum HMGB1 levels were not related to respiratory complications, the requirement of inotropic agents, or survival.
Figure 2 (A) Comparison of serum high mobility group box protein 1 (HMGB1) levels between patients with (median 11.0, IQR 7.35–63.0) and without (median 4.5, IQR 2.9–6.3) disseminated intravascular coagulation (DIC). (B) Comparison of serum HMGB1 levels between patients with (median 14.35, IQR 6.96–189.6) and without (median 5.4, IQR 3.2–8.4) central nervous system (CNS) complications.
HMGB1 and laboratory parameters
Correlations between serum HMGB1 levels and laboratory parameters are shown in . Serum HMGB1 levels in HLH patients were positively correlated with aspartate aminotransferase (AST) (rs =0.48, p<0.01) and negatively correlated with fibrinogen (rs = −0.475, p=0.011) and hemoglobin (rs = −0.465, p=0.013).
Table 2 Laboratory parameters and correlation with HMGB1
Discussion
It has recently become clear that alarmins play an important role in the induction of sterile and nonsterile inflammation.Citation2 The pathogenesis of HLH has been elucidated from the viewpoint of defective cytotoxicity of cytotoxic T cells and NK cells.Citation5 The role of alarmins in inducing additional inflammation in HLH has recently received attention.Citation6 HMGB1 is a potent alarmin that activates inflammation and innate immunity, and it is expected to be a molecular target for therapy of various inflammatory disorders including HLH.Citation15,Citation16 We conducted our study on this background, particularly focusing on the relations between serum HMGB1 levels and clinical symptoms and laboratory parameters.
Serum HMGB1 values in the patients of this study had a broad range from 1.1 to 574 ng/mL. The median level was almost the same as those in previous reports,Citation8–Citation10 but extremely high serum HMGB1 levels were seen in three patients (11%). Although these three patients recovered from HLH, two of them experienced a severe clinical course of HLH. The present study did not show that serum HMGB1 levels were correlated with outcome, but in cases of severe HLH, the presence of strikingly high levels of HMGB1 should be taken into account in management of the disease. Also, from the findings that the serial serum HMGB1 levels fell to reflect the disease activity in patient 4 (), serum HMGB1 levels may be a useful biomarker in HLH.
Interestingly, our results showed that serum HMGB1 levels are associated with two important clinical symptoms, DIC and CNS complications, which are considered to be the prognostic factors of HLH.Citation17,Citation18
In this study, serum HMGB1 levels significantly differed between patients with and without DIC. The mechanisms by which alarmins trigger DIC have been elucidated. HMGB1 triggers cell surface expression of tissue factors on monocytes, extrusion of neutrophil extracellular traps, and inhibition of the anticoagulant protein C pathway.Citation19 Although increased fibrinolysis and decreased fibrinogen production in liver damage have been discussed in relation to coagulopathy in HLH,Citation20,Citation21 our present study showed that HMGB1 may also play an important role in the development of DIC in children with HLH.
The mechanisms by which systemic inflammation causes CNS damage have been studied, particularly in a model of sepsis-induced encephalopathy. In this model, HMGB1 may be one of the mediators that cause neuroaxonal damage; thus, anti-HMGB1 antibody is a potential new treatment strategy.Citation22 Interestingly in our study, serum HMGB1 levels were significantly higher in patients with CNS complications than in patients without CNS complications. Also, leukoencephalopathy was revealed by MRI in two of the three patients who exhibited strikingly high serum HMGB1 levels. Although further study in a large cohort is needed, our results suggest that serum HMGB1 may be related to CNS complications in HLH.
Only one report has assessed correlations between serum HMGB1 levels and laboratory parameters. Wang et al reported positive correlations of HMGB1 levels with soluble CD25 and erythrocyte sedimentation rate.Citation9 In our study, serum HMGB1 levels were correlated with AST, fibrinogen, and hemoglobin levels. However, these findings must be interpreted cautiously because our sample size was small. Further study in a large cohort is needed to determine which parameters are correlated with HMGB1.
Our present study has three limitations. First, our patient cohort was small because of the rarity of HLH. Second, we measured total HMGB1 levels but did not consider HMGB1 isoforms, ie, the redox states of the three cysteines of HMGB1 and the acetylation states of the lysine residues of HMGB1. Because the redox isoforms of HMGB1 determine its specific activities, such as chemoattractant activity and cytokine-inducing activity, via interactions with different receptors, and because the acetylation isoforms could originate by passive release from dying cells or active release from NK cells and monocytes, a more precise analysis of HMGB1 in HLH is available by assessing these isoforms as previously described by Palmblad et al.Citation8 Third, we could not enroll a control group comprising patients with infection, malignancy, and systemic inflammatory response syndrome who did not develop HLH. Thus, we could not precisely analyze whether serum HMGB1 is derived from inflammation specific to HLH or damaged cells.
Conclusion
In conclusion, the present study showed that serum HMGB1 levels reflect clinical features of childhood HLH. HMGB1 is a potential mediator involved in the pathogenesis and determining the clinical findings of HLH.
Acknowledgment
This research was supported by JSPS KAKENHI Grant Number 15K19625. The authors would like to thank Enago for the English language review.
Disclosure
The authors report no conflicts of interest in this work.
References
- Yang H, Antoine DJ, Andersson U, Tracey KJ. The many faces of HMGB1: molecular structure-functional activity in inflammation, apoptosis, and chemotaxis. J Leukoc Biol. 2013;93(6):865–873. doi:10.1189/jlb.121266223446148
- Andersson U, Yang H, Harris H. High-mobility group box 1 protein (HMGB1) operates as an alarmin outside as well as inside cells. Semin Immunol. 2018;38:40–48. doi:10.1016/j.smim.2018.02.01129530410
- Wang H, Bloom O, Zhang M, et al. HMG-1 as a late mediator of endotoxin lethality in mice. Science. 1999;285(5425):248–251. doi:10.1126/science.285.5425.24810398600
- Martinotti S, Patrone M, Ranzato E. Emerging roles for HMGB1 protein in immunity, inflammation, and cancer. Immunotargets Ther. 2015;4:101–109.27471716
- Morimoto A, Nakazawa Y, Ishii E. Hemophagocytic lymphohistiocytosis: pathogenesis, diagnosis, and management. Pediatr Int. 2016;58(9):817–825. doi:10.1111/ped.1279027289085
- Brisse E, Wouters C, Matthys P. Advances in the pathogenesis of primary and secondary haemophagocytic lymphohistiocytosis: differences and similarities. Br J Haematol. 2016;174(2):203–217. doi:10.1111/bjh.1408427264204
- Alcamo AM, Pang D, Bashir DA, et al. Role of damage-associated molecular patterns and uncontrolled inflammation in pediatric sepsis-induced multiple organ dysfunction syndrome. J Pediatr Intensive Care. 2019;8(1):25–31. doi:10.1055/s-0038-167563931073505
- Palmblad K, Schierbeck H, Sundberg E, et al. High systemic levels of the cytokine-inducing HMGB1 isoform secreted in severe macrophage activation syndrome. Mol Med. 2014;20(1):538–547. doi:10.2119/molmed.2014.00183
- Wang DJ, Wang JJ, Song M, et al. Expression of serum HMGB-1 in patients with secondary hemophagocytic lymphohistiocytosis and its clinical significance. Zhongguo Shi Yan Xue Ye Xue Za Zhi. 2016;24(3):878–883.27342526
- Farias-Moeller R, LaFrance-Corey R, Bartolini L, et al. Fueling the FIRES: hemophagocytic lymphohistiocytosis in febrile infection-related epilepsy syndrome. Epilepsia. 2018;59(9):1753–1763. doi:10.1111/epi.1452430132834
- Henter JI, Horne A, Aricó M, et al. HLH-2004: diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2007;48(2):124–131. doi:10.1002/pbc.2103916937360
- Wada H, Gabazza EC, Asakura H, et al. Comparison of diagnostic criteria for disseminated intravascular coagulation (DIC): diagnostic criteria of the international society of thrombosis and hemostasis (ISTH) and of the Japanese ministry of health and welfare for overt DIC. Am J Hematol. 2003;74(1):17–22. doi:10.1002/ajh.1037712949885
- Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013;48(3):452–458. doi:10.1038/bmt.2012.24423208313
- Lehmberg K, Nichols K, Henter JI, et al. Consensus recommendations for the diagnosis and management of hemophagocytic lymphohistiocytosis associated with malignancies. Haematologica. 2015;100(8):997–1004.26314082
- Andersson U, Tracey KJ. HMGB1 is a therapeutic target for sterile inflammation and infection. Ann Rev Immunol. 2011;29:139–162. doi:10.1146/annurev-immunol-030409-10132321219181
- Brisse E, Matthys P, Wouters C. Understanding the spectrum of haemophagocytic lymphohistiocytosis: update on diagnostic challenges and therapeutic options. Br J Haematol. 2016;174(2):175–187. doi:10.1111/bjh.1408427292929
- Valade S, Azoulay E, Galicier L, et al. Coagulation disorders and bleeding in critically ill patients with hemophagocytic lymphohistiocytosis. Medicine. 2015;94(40):e1692. doi:10.1097/MD.000000000000169226448017
- Horne A, Trottestam H, Aricò M, et al. Frequency and spectrum of central nervous system involvement in 193 children with haemophagocytic lymphohistiocytosis. Br J Haematol. 2007;140(3):327–335. doi:10.1111/j.1365-2141.2007.06922.x18076710
- Liaw PC, Ito T, Iba T, et al. DAMP and DIC: the role of extracellular DNA and DNA-binding proteins in the pathogenesis of DIC. Blood Rev. 2016;30(4):257–261. doi:10.1016/j.blre.2015.12.00426776504
- Favara BE. Hemophagocytic lymphohistiocytosis: a hemophagocytic syndrome. Semin Diagn Pathol. 1992;9(1):63–74.1561489
- Yang SL, Xu XJ, Tang YM, et al. Associations between inflammatory cytokines and organ damage in pediatric patients with hemophagocytic lymphohistiocytosis. Cytokine. 2016;85:14–17. doi:10.1016/j.cyto.2016.05.02227269180
- Sankowski R, Mader S, Valdés-Ferrer SI. Systemic inflammation and the brain: novel roles of genetic, molecular, and environmental cues as drivers of neurodegeneration. Front Cell Neurosci. 2015;9:28. doi:10.3389/fncel.2015.0002825698933