Abstract
Thrombocytopenia is a common laboratory finding in current medical practices. The workup of thrombocytopenia can be challenging with numerous causes that can be included in the differential diagnosis. Thrombocytopenia can be due to bone marrow hypoproliferation, peripheral destruction, or sequestration. This paper presents a case of isolated thrombocytopenia in a young female and discusses the causes of thrombocytopenia.
Introduction
The workup of isolated thrombocytopenia is common in hematology practice and is often conceptually divided into causes of bone marrow hypoproliferation or peripheral destruction or sequestration. Anatomic considerations for thrombocytopenia are typically not evaluated due to the low incidence of the subsequent cause of thrombocytopenia. Congenital diaphragmatic hernias can be a cause of low platelet counts. This paper presents an unusual case of isolated thrombocytopenia: the wandering spleen.
Case report
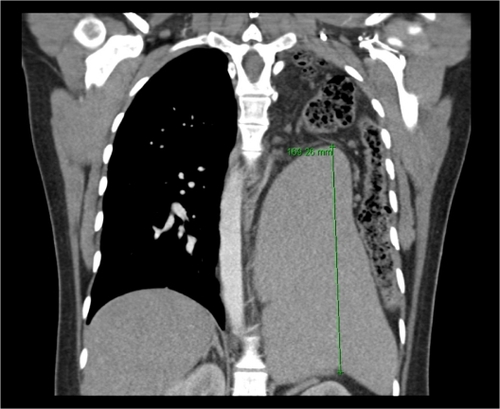
A previously healthy 21-year-old woman, 16 weeks pregnant with her first child, presented to the hospital with nausea, vomiting, and right flank pain. She was diagnosed with pyelonephritis, and treated with appropriate antibiotics. When she was 24 weeks pregnant she presented in consultation for evaluation of thrombocytopenia 8 weeks following initial hospitalization. She took only prenatal vitamins and did not drink alcohol or use nonprescribed medications or illicit drugs. Her personal and family history was unremarkable for any bleeding or clotting disorders. Physical examination demonstrated normal vital signs, normal cardiac exam, peristaltic sounds in the left chest, and a gravid uterus which precluded full examination. There were no petechiae or other signs of bleeding. At the time of consultation, platelet count was 76,000/L (150–450/L) with a mean platelet volume (MPV) of 12.3 fL (7.4–12.0 fL), hemoglobin was 10.1 mg/dL (12.0–16.0 mg/L), and white blood cell count was 4400/L (4.8–10.8/L) with a normal differential. Peripheral blood smear review confirmed thrombocytopenia, excluded microangiopathic changes, and revealed red cell morphology consistent with iron deficiency. Folate and B12 were normal. Serologic testing for viral hepatitis and human immunodeficiency virus were negative; Helicobacter pylori was not tested for during this hospitalization. Liver transaminases and bilirubin were normal. A bone marrow examination demonstrated iron deficiency, megakaryocytic hyperplasia, and no evidence of dysplasia or megaloblastic change. Cytogenetic studies were normal with 46, XX. As part of the workup during the previous illness a chest X-ray was obtained (), which demonstrated a cystic appearance to much of the left lung and elevation of the left hemidiaphragm. A computed tomography scan () with abdominal shielding was obtained and revealed herniation of abdominal contents into the left hemithorax. The spleen was intrathoracic and its craniocaudal dimension was 17 cm. The spleen was of uniform density without any focal lesions. One month after an uncomplicated delivery, the platelet count remained 73,000/L with an MPV of 12.4 fL. One year after delivery, a platelet count of 80,000/L with an MPV of 12.1 fL was obtained. The diagnosis of thrombocytopenia due to peripheral sequestration in a wandering spleen was made.
Figure 1 Cystic appearance to left lung with elevated hemidiaphragm.
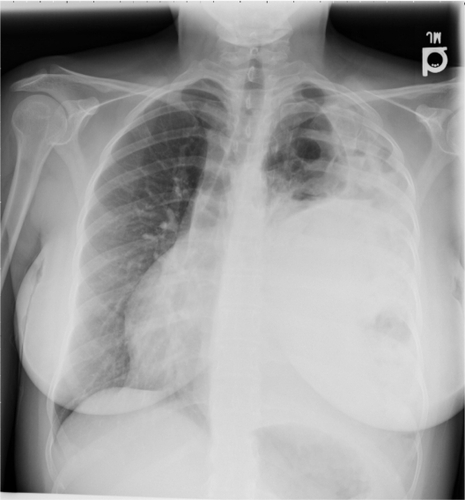
Figure 2 Abdominal contents including bowel and massively enlarged spleen.
Discussion
Thrombocytopenia can be classified according to either decreased production with bone marrow hypoproliferation or increased destruction. Common causes of thrombocytopenia in young female patients include primary immune thrombocytopenia, bone marrow suppression by infection, medication effects, and gestational thrombocytopenia.Citation1 A list of possible etiologies is included in .
Table 1 Causes of thrombocytopenia
Bone marrow suppression and primary immune thrombocytopenia are typically accompanied by a normal sized spleen. Hypersplenism as a cause of thrombocytopenia may reflect portal hypertension from cirrhosis, collagen vascular disease, or rarely primary neoplasm of the spleen. Gestational thrombocytopenia resolves after delivery by definition.
Although rarely considered, anatomical causes of thrombocytopenia do exist. Congenital diaphragmatic hernias are due to a defect in the diaphragm, either posterolateral (Bochdalek hernia), anterior retrosternal or peristernal (Morgagni hernia), or, rarely, central. The Bochdalek type of diaphragmatic hernia is the most common, but all diaphragmatic hernias can allow for abdominal contents, including bowel, viscera, and even organs such as the spleen, to herniate into the chest and impede lung formation resulting in hypoplasia.Citation2 The spleen is normally prevented from cephalad migration by the diaphragm. The spleen is usually fixed in its position in the left upper abdominal quadrant through the splenic pedicle formed by the splenorenal and gastrosplenic ligaments and contains the splenic artery and vein and the tail of the pancreas.Citation3 Asymptomatic prevalence of Bochdalek-type hernias in the general population may be as high as 0.17%.Citation4,Citation5 Diaphragmatic hernias have also been seen as a result from penetrative or blunt trauma to the chest or abdomen; approximately 100 cases of Bochdalek hernias in adulthood have been reported.Citation6
The proposed mechanism for splenic enlargement in this case is as a result of torsion or compression of the splenic pedicle with impairment of venous outflow and resultant splenic congestion and enlargement.Citation3 An ectopic abdominal placement of the spleen, or “wandering spleen,” is caused by an elongated splenic vascular pedicle and can produce splenomegaly by a similar mechanism.
Hypersplenism from splenic sequestration resulting in thrombocytopenia seen as a complication of congenital diaphragmatic hernia is a rare finding. Typically, congenital diaphragmatic hernias are detected at or near the time of delivery and most presentations involve respiratory distress secondary to a hypoplastic lung. A Bochdalek-type hernia later in life, similar to the present case, has rarely presented, where strangulation of her spleen within the left hemithorax led to the development of left-sided portal hypertension, hypersplenism, and thrombocytopenia.Citation6
Conclusion
The wandering spleen is an unusual congenital anatomic cause of thrombocytopenia and may be explained by the mechanism of peripheral sequestration in an enlarged spleen.
Disclosure
The authors report no conflicts of interest in this work.
References
- ProvanDStasiRNewlandACInternational consensus report on the investigation and management of primary immune thrombocytopeniaBlood2010115216818619846889
- BohnDCongenital diaphragmatic herniaAm J Respir Crit Care Med2002166791191512359645
- MollSIgelhartJDOrtelTLThrombocytopenia in association with a wandering spleenAm J Hematol19965342592638948667
- BurandaLLarruceaIRamosFMuñozCSánchezAFernándezIBochdalek’s hernia in adultsJ Clin Gastroenterol200132215515711205653
- MullinsMESteinJSainiSSMuellerPRPrevalence of incidental Bochdalek’s hernia in a large adult populationAJR Am J Roentgenol2001177236336611461863
- KennedyRDonaghyAAhmadJMcManusKClementsWDPortal hypertension and hypersplenism in a patient with a Bochdalek hernia: a case reportIr J Med Sci2009178111111318398560