
Abstract
Background
Human brucellosis is a multisystem disease with a wide range of clinical signs which often leads to misdiagnosis and treatment delay. Early diagnosis of this disease can prevent the serious complications and mismanagements. This study aimed to evaluate the hematological parameters with predictive value for the diagnosis of brucellosis.
Methods
In this prospective case–control study which was done during 2015–2017 in Imam Reza Hospital, Kermanshah Province, west Iran, 100 patients with a confirmed diagnosis of brucellosis (brucellosis group) and 100 healthy individuals (control group) were studied. The hematological parameters, including hemoglobin (Hb), red blood cell (RBC), white blood cell (WBC) count, lymphocyte count, neutrophil count, platelet count (PLTs), mean platelet volume (MPV), platelet distribution width (PDW), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) of both groups were recorded. The data were statistically compared between the brucellosis and the control groups.
Results
The mean age of patients and healthy groups was 44.04 ± 23.11 and 37.92 ± 24.80, respectively (P = 0.062). The WBC, CRP and neutrophil counts were significantly higher in the brucellosis group (P < 0.05). Based on the receiver operating characteristic (ROC) analysis, the sensitivity and specificity were 54% and 66% for the WBC, 45% and 71% for the neutrophil and 65% and 72% for the CRP, respectively. There was no statistically significant difference between the two groups in terms of Hb, RBC, WBC, lymphocyte and platelet count, MPV, PDW and ESR (P > 0.05).
Conclusion
The results of this study indicate that WBC, CRP and neutrophil count can be used as valuable markers in the preliminary diagnosis of brucellosis. However, further researches are required to standardize these parameters for various forms of brucellosis.
Introduction
Brucellosis is an infectious disease caused by a gram-negative coccobacillus of the genus Brucella, with various clinical manifestations. More than half a million people are diagnosed with brucellosis every year.Citation1 After acquiring Brucella, bacteria spread through hematogenous dissemination and affect various organs, such as the urinary, respiratory, central nervous system and cardiovascular. The spread of infection triggers common symptoms of illness, such as fever, nocturnal hyperhidrosis, weight loss, anorexia, arthralgia, and fatigue.Citation1,Citation2 This zoonotic disease, which remains a major public and economic health issue in many developing countries, is endemic to the Middle East, South and Central America, the Mediterranean region, and India.Citation3 Based on reports Iran ranks second in the world in terms of brucellosis and its annual incidence is 98 to 130 people per 100,000 populations.Citation4 Early and accurate diagnosis of this disease, therefore, plays an important role in controlling and eradicating brucellosis for improving public health. Various laboratory tests, such as bacteriological, serological and molecular methods, have been developed to diagnose brucellosis.Citation5 While bacterial culture is the gold standard for brucellosis diagnosis, in most cases Brucella culture is not promising due to the lack of optimum conditions. Therefore, serological tests are often used as diagnostic and screening tools.Citation5,Citation6 Serological tests sometimes have false results, in particular in case of cross-reactions with other gram-negative bacteria such as Escherichia coli, Yersinia enterocolitica, and Salmonella Urbana.Citation5 Since a high rate of false-positive results with serological tests, the confirmatory tests are required for positive samples.
Recently, diverse hematological and inflammatory factors have been widely considered as markers of bacterial infections with abundant evidence to support their usefulness in the preliminary diagnosis of infections.Citation7,Citation8 Because Brucella is an intracellular bacterium, it can live in phagocytic cells, such as neutrophils and macrophages.Citation9 Brucellosis is often presented with inflammatory symptoms. Following infection, Brucella spreads to the lymph nodes and from there to the blood and causes systemic infection.Citation6 As a result, the increase in the number of leukocytes and neutrophils, as well as changes in inflammatory indices, occurs during infection.Citation10,Citation11 Research has shown that platelets also contribute to the inflammatory response.Citation12–Citation14 Changes in hematological markers are commonly observed in brucellosis.Citation6 Hematological markers, including white blood cell count, platelet count (PLT), mean platelet volume (MPV), platelet distribution width (PDW), red cell distribution width (RDW), neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), monocyte to lymphocyte ratio (MLR), and CRP test, have been used in the preliminary diagnosis of brucellosis, along with serological tests.Citation14 Both diagnosis and follow-up of treatment for brucellosis are complicated, and it may be helpful to use routine laboratory tests for better management of this disease.Citation15 The purpose of this research was to evaluate the hematological and inflammatory markers for laboratory diagnosis and follow-up of brucellosis.
Patients and Methods
Participants
This prospective and case–control study was carried out on the brucellosis patients who had been referred to the Imam Reza Hospital between July 2015 and March 2017. This Hospital is the referral center for infectious diseases located in Kermanshah, West of Iran. Furthermore, as a control group, the healthy people of similar age and gender admitted to the Imam Reza Hospital for routine check-up were selected during the same period.
The diagnosis of brucellosis cases was based on clinical of symptoms (fever, joint pain, sweating and fatigue) and laboratory results (Wright, Coombs Wright and 2-mercaptoethanol (2ME) tests). People with a history of brucellosis or inflammatory diseases, anemia, malignancies, platelet disorders, blood transfusion within the last 3 months, HIV infection, diabetes mellitus, hypertension and other kinds of diseases were excluded from this study. None of the subjects had received steroid therapy or another anti-inflammatory drug. Information regarding age, sex and medical history were recorded from individual’s files or interviews. All subjects were agreed to sign an informed written consent for this study. This study was approved by the Ethics Committee of the Kermanshah University of Medical Sciences.
Blood Test
Five mL of venous blood sample was collected from the participant and stored in tubes containing EDTA. A complete blood count analysis was done with automated analyzers Coulter HmX from Beckman Coulter at admission. Hemoglobin (Hb), Red blood cell (RBC) count, white blood cell (WBC) count, lymphocyte count, neutrophil count, platelet count (PLTs), mean platelet volume (MPV), platelet distribution width (PDW), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) were recorded for each individual. The reference values in the affiliated Imam Reza laboratory were 3.5–9.5×109/μL for WBC count, 1.8–6.3 ×109/μL for neutrophil count, 40–70% for neutrophil percentage, 181–300 ×109/μL for PLT, 9.4–12.5 fL for MPV and 15.5–18.1% for PDW.
Data Analysis
The SPSS software was used for statistical analysis (version 20, SPSS Inc., Chicago, IL, USA). The Kolmogorov–Smirnov test was applied to evaluate the normal distribution of the data in each group. Continuous variables have been presented as mean ± standard deviation (SD). Independent samples t-test or Mann–Whitney U-test was used for comparison of two groups. Categorical variables were compared using chi-square test. The cut-off value for WBC and neutrophil count that best distinguishes between healthy controls and brucellosis patients were performed using receiver operating characteristic (ROC) curves analysis, for which sensitivity and specificity values were calculated. Correlations between numerical variables were assessed using Pearson’s or Spearman correlation analysis. P value <0.05 was taken as significant.
Results
The 100 brucellosis patients and 100 healthy people with age and gender matched as the control group were included in this study. There were 52 male participants in the brucellosis and 59 in the control group (P =0.319). Mean age of brucellosis and the control group was 44.04 ± 23.11 and 37.92± 24.80 years, respectively (P =0.062). There was no statistical difference between the two groups in terms of age and sex (P>0.05).
The comparisons of blood parameters between brucellosis and control groups have been given in . No significant difference was detected in the RBC count, neutrophil count, lymph count, ESR percentage, Hb, RDW, PLRC, PDW, PLT, and MPV values between the two groups (P>0.05). The WBC and neutrophil counts were 7.1 and 57 in the control group, which were significantly lower than that in brucellosis patients with 8.9, and 65, respectively (P < 0.05).
Table 1 The Comparison of Laboratory Findings of Brucellosis and Control Groups
Based on the ROC analysis, in the brucellosis group, the cut-off values of the WBC and neutrophil were 7.55 and 53.7, respectively (). The sensitivity and specificity were 54% and 66% for the WBC, 45% and 71% for the neutrophil and 65% and 72% for the CRP, respectively. The area under the curve (AUC) of the WBC and neutrophil were 0.62 and 0.58, respectively ().
Figure 1 ROC curve for the WBC and neutrophil.
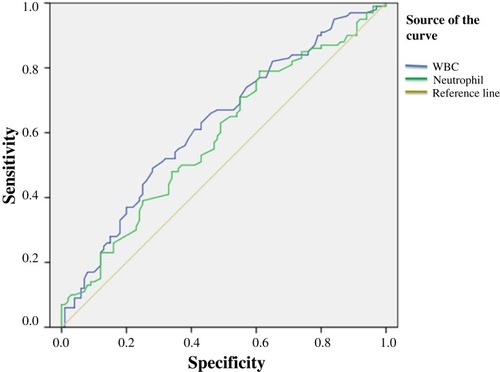
Table 2 Results of ROC Analysis for Blood Parameters
Spearman correlation coefficient revealed an inverse and significant correlation between the number of neutrophils and the number of lymphocytes (r coefficient: -0.817, p<0.001). In other words, as the number of neutrophils increased, the number of lymphocytes decreased. Also, the number of neutrophils showed a direct and significant relationship with the number of WBC (r coefficient: -0.817, P<0.032).
Discussion
Brucellosis is an important health problem in Iran, where animal husbandry is an important livelihood. According to a systematic review and meta-analysis in Iran, the highest rate of brucellosis was related to Kermanshah Province with 276.42/100,000 people.Citation16 B. mellitensis accounts for the majority of the disease in humans in various provinces of Iran, followed by B. abortus.Citation17
This is not the first study on changes in the hematological parameters in patients with brucellosis. However, given the impact of biological and environmental factors on microbial infection, it can provide a better local view for these parameters. Research results show that hematological parameters in patients with brucellosis differ from patient to patient and these parameters can return to their normal value after the treatment of brucellosis.Citation6 The inflammatory process that occurs during brucellosis is associated with an increase in acute-phase reactants.Citation18
CRP is an acute-phase protein that increases up to 1000-fold in the blood of patients with infection or inflammation. During some bacterial infections, CRP level elevates in the response to cytokines, mainly tumor necrosis factor-α, interleukin (IL)-1β and IL-6.Citation19 The production of this cytokine is one of the primary phagocyte responses.Citation19 CRP is able to binds to various bacteria with exposed phosphocholine (PCh) groups. This interaction activates the classical complement system to destroy the ligand and kill off the pathogen.Citation20 However, Healy and Freedman suggested that the level of serum CPR could only indicate the presence of infection.Citation21 A study in Turkey reported that the level of CRP was higher in osteoarticular brucellosis patients than in non-osteoarticular brucellosis patients.Citation22 Another study reported that patients with the acute brucellosis exhibited higher CRP levels than the control group.Citation6,Citation13,Citation23 Some other studies have suggested that elevated CRP level may also be associated with disease severity and mortality in hospitalized patients with community-acquired pneumonia.Citation24 In our study, CRP was significantly higher in brucellosis patients, which indicates that CRP is a valuable marker for the diagnosis of brucellosis.
WBC count can be considered as a marker for leukocytosis in brucellosis.Citation13 Neutrophils and lymphocytes play an important role in inflammatory processes. Physiological immune responses are characterized by an increase in the number of neutrophils and a decrease in the number of lymphocytes.Citation6 Our findings revealed that the mean of WBC and neutrophil count in Brucella patients were significantly higher than in control groups. Therefore, they can be reliable markers for the evaluation of brucellosis along with other clinical findings and blood marker changes. Research has shown that the number of leukocytes and neutrophils increases in infections, especially in bacterial infections that indicate an inflammatory response.Citation25,Citation26 Brucella lipoproteins also have pro-inflammatory properties through direct neutrophil activation.Citation6 The results of the study by Aktar et al showed that the mean values for neutrophils and leukocytes in children with Brucella arthritis were higher than the control group (P<0.05).Citation12 Imani-Rastabi et al examined changes in blood factors in sepsis and indicated that there was a statistically significant difference in the WBCs count before and after sepsis.Citation27
In addition to regulating the immune system responses, studies have reported that platelets also play an active role in the inflammation process.Citation6,Citation12 For this purpose, when platelets are activated, they actively participate in host defense through phagocytosis and the development of cytotoxic-free radicals and oxidative molecules.Citation28 Platelets are involved in inflammatory responses through the involvement of neutrophils and macrophages, increased vascular permeability, leukocyte infiltration and inflammatory mediators such as cytokines and chemokines.Citation5,Citation15,Citation29 It has been reported that in thrombocytopenia, edema and leukocyte infiltration are reduced.Citation29 MPV is an essential platelet marker linked to the platelet activity and function. PDW which indicates changes in platelet size is correlated with the activity of the platelet.Citation13,Citation30 Changes in this index have been reported as a marker to evaluate various inflammatory and infectious diseases.Citation13,Citation31 In our study, although the mean values for PLT, MPV, and PDW were lower in the brucellosis group, there were no statistically significant changes (P>0.05). Our findings are consistent with the Togan et al, which found that MPV levels were in the normal range in treatment and control groups.Citation13 Several studies suggested that the values of MPV and PLT were lower in the brucellosis group than in the control group (P<0.05).Citation15,Citation18,Citation32 Nevertheless, a number of studies have documented that differed MPV levels in specific inflammatory conditions. One indicated that in children with Kawasaki disease, MPV was not a valuable marker for predicting coronary artery abnormalities.Citation33 A second reported that the benefit of MPV as an inflammatory marker to determine the disease activity in TB patientsCitation34 and a third noted a higher MPV in children infected with Helicobacter pylori infection than in healthy controls.Citation35 Overall, it is thought that during an acute infection such as septicemia the initial increase in MPV level can be related to thrombocytopenia and during chronic or persisted bacterial infection a delayed decline in MPV level can be related to thrombocytosis.Citation36
Here, we should report some limitations of this study. The sample size was small and failed to the evaluation of all clinical forms of brucellosis such as acute, chronic, or focal forms. Therefore, to reach more valuable results, a more comprehensive study in several centers with a larger sample size is recommended.
Conclusion
As a result, hematological parameters in patients with brucellosis are relatively different in various studies. Our analysis and most of the studies have shown that the most significant signs of brucellosis are an increase in the number of leukocytes and a decrease in the number of thrombocytes and lymphocytes. It seems that along with clinical symptoms and serological and culture methods, hematological parameters, such as WBC, neutrophil, and CRP which are inexpensive and available in hospitals, can be useful in the preliminary diagnosis and assessment of brucellosis infection.
Data Sharing Statement
The data sets used and/or analyzed during this study are available from the corresponding author on reasonable request and were received permission for use by the Kermanshah University of Medical Sciences Ethics Committee.
Ethics and Consent Statement
All the participants provided written informed consent prior to the study and this study was conducted in accordance with the Declaration of Helsinki. The protocol was approved by the Kermanshah University of Medical Sciences Ethics Committee.
Acknowledgments
The authors want to thank their colleagues in Imam Reza Therapeutic Educational hospital of Kermanshah, Iran for their contribution to the patient’s diagnosis. We also extend our thanks to the clinical research development center of Imam Reza Hospital affiliated to Kermanshah University of Medical Sciences for their kind support.
Disclosure
The authors report no conflicts of interest in this work.
References
- Cift A, Yucel MO. Comparison of inflammatory markers between brucella and non-brucella epididymo-orchitis. Int Braz J Urol. 2018;44(4):771–778. doi:10.1590/s1677-5538.ibju.2018.0004.029697933
- Bashiri H, Sayad B, Madani SH. Study of the assimilation rate of immunoenzymatic tests and traditional serological methods in the diagnosis of human brucellosis. Jundishapur J Microbiol. 2013;6(4):1–4. doi:10.5812/jjm
- Baldane S, Sivgin S, Alkan TS, et al. An atypical presentation of brucellosis in a patient with isolated thrombocytopenia complicated with upper gastrointestinal tract bleeding. Case Rep Med. 2012;2012:473784. doi:10.1155/2012/47378423118764
- Marvi A, Asadi-Aliabadi M, Darabi M, Abedi G, Siamian H, Rostami-Maskopaee F. Trend analysis and affecting components of human brucellosis incidence during 2006 to 2016. Med Arch. 2018;72(1):17–21. doi:10.5455/medarh.29416212
- Bonfini B, Chiarenza G, Paci V, et al. Cross-reactivity in serological tests for brucellosis: a comparison of immune response of Escherichia coli O157: H7and Yersinia enterocolitica O:9 vs brucella spp. Vet Ital. 2018;54(2):107–114. doi:10.12834/VetIt.1176.6539.230019327
- Bozdemir SE, Altıntop YA, Uytun S, et al. Diagnostic role of mean platelet volume and neutrophil to lymphocyte ratio in childhood brucellosis. Korean J Intern Med. 2017;32(6):1075. doi:10.3904/kjim.2016.09227951626
- Markanday A. Acute phase reactants in infections: evidence-based review and a guide for clinicians. Open Forum Infect Dis. 2015;2(3):ofv098. doi: 10.1093/ofid/ofv09826258155
- Akya A, Rostami-Far Z, Chegene Lorestani R, et al. Platelet indices as useful indicators of urinary tract infection. Iran J Ped Hematol Oncol. 2019;9(3):159–165.
- Lopez-Santiago R, Sanchez-Argaez AB, De Alba-nunez LG, Baltierra-Uribe SL, Moreno-Lafont MC Immune response to mucosal brucella infection. Front Immunol. 2019;10:1759. doi:10.3389/fimmu.2019.0175931481953
- Ulug M, Yaman Y, Yapici F, Can-Ulug N. Clinical and lab-oratory features, complications and treatment outcome of brucellosis in childhood and review of the literature. Turk J Pediatr. 2011;53(4):413–424.21980844
- Caylak SD, Sozen H, Gonen I, et al. A brucellosis case presenting with vesicular and maculopapular rash and febrile neutropenia. J Microbiol Infect Dis. 2014;4(1):39–41. doi:10.5799/ahinjs.02.
- Aktar F, Tekin R, Bektas MS, et al. Diagnostic role of inflammatory markers in pediatric brucella arthritis. Ital J Pediatr. 2016;42(1):3. doi:10.1186/s13052-016-0211-526753565
- Togan T, Narci H, Turan H, Ciftci O, Kursun E, Arslan H. The impact of acute brucellosis on mean platelet volume and red blood cell distribution. Jundishapur J Microbiol. 2015;8(2):e20039. doi:10.5812/jjm.20039.25825650
- Afyon M, Artuk C. Could mean platelet volume be a useful marker for infectious diseases? A review of literature. Medicine. 2016;5(4):1059–1062.
- OztUrk ZA, Kuyumcu ME, Yesil Y, et al. Mean platelet volume in assessment of brucellosis disease. Biomed Res. 2012;23(4):541–546.
- Mirnejad R, Jazi FM, Mostafaei S, Sedighi M. Epidemiology of brucellosis in Iran: a comprehensive systematic review and meta-analysis study. Microb Pathog. 2017;109:239–247. doi:10.1016/j.micpath.2017.06.00528602839
- Golshani M, Buozari S. A review of brucellosis in Iran: epidemiology, risk factors, diagnosis, control, and prevention. Iran Biomed J. 2017;21(6):349–359. doi:10.18869/acadpub.ibj.21.6.34928766326
- Bozkurt F, Aslan E, Deveci O, Tekin R. Evaluation of mean platelet volume levels in patients with brucellosis. Anatol J Clin Investig. 2014;8(3):126–129.
- Sproston, NR, Ashworth JJ. Role of C-reactive protein at sites of inflammation and infection. Front Immunol. 2018;9:754. doi:10.3389/fimmu.2018.0075429706967
- Mortensen RF. C-reactive protein, inflammation, and innate immunity. Immunol Res. 2001;24(2):163–176. doi:10.1385/IR:24:211594454
- Healy B, Freedman A. Infections. Br Med J. 2006;332(7545):838–841. doi:10.1136/bmj.332.7545.83816601046
- Balın SO, Tartar AS, Akbulut A. The predictive role of haematological parameters in the diagnosis of osteoarticular brucellosis. Afr Health Sci. 2018;18(4):988–994. doi:10.4314/ahs.v18i4.1930766564
- Mobaien A, Esna-Ashari F, Eini P, et al. A retrospective evaluation of epidemiological, clinical and laboratory features of brucellosis in 230 patients in Hamadan, Iran&58; a brief report. Tehran Uni Med J. 2012;70(2):130–135.
- Ruiz-Gonzalez A, Utrillo L, Bielsa S, et al. The diagnostic value of serum C-reactive protein for identifying pneumonia in hospitalized patients with acute respiratory symptoms. J Biomark. 2016;2198745.27610265
- Zwerdling A, Delpino MV, Pasquevich KA, et al. Brucella abortus activates human neutrophils. Microbes Infect. 2009;11(6–7):689–697. doi:10.1016/j.micinf.2009.04.01019376263
- Skendros P, Boura P. Immunity to brucellosis. Rev Sci Tech. 2013;32(1):137–147. doi:10.20506/rst.issue.32.1.5223837372
- Imani-Rastabi R, Shahabi G, Fazel A. Study of variances in some blood factors during sepsis diagnosis and their interrelations. J Shahrekord Uuni Med Sci. 2013;15(2):86–93.
- Tekin R, Aktar F, Ayaz C. Comparison of inflammatory markers between adult and pediatric brucellosis patients. Open Forum Infect Dis. 2017;4(1):S350–S351. doi:10.1093/ofid/ofx163.844
- Gros A, Ollivier V, Ho-Tin-Noe B. Platelets in inflammation: regulation of leukocyte activities and vascular repair. Front Immunol. 2015;5(678):1–8. doi:10.3389/fimmu.2014.00678
- Zayed KMS, Abdelhakeem AM, Gafar HS, et al. Diagnostic value of platelet parameters versus interleukin-6 in children with urinary tract infection. Gaz Egypt Paediatr Assoc. 2016;64(3):142–148. doi:10.1016/j.epag.2016.04.002
- Kucukbayrak A, Tas T, Tosun M, et al. Erythrocytes parameters in the course of brucellosis. Abant Med J. 2013;2(1):36–39. doi:10.5505/abantmedj.2013.26349
- Okan DH, Gokmen Z, Seyit B, Yuksel K, Cevdet Z, Deniz A. Mean platelet volume in brucellosis: correlation between brucella standard serum agglutination test results, platelet count, and C-reactive protein. Afr Health Sci. 2014;14(4):797–801. doi:10.4314/ahs.v14i4.425834485
- Bozlu G, Karpuz D, Hallioglu O, Unal S, Kuyucu N. Relationship between mean platelet volume-to-lymphocyte ratio and coronary artery abnormalities in Kawasaki disease. Cardiol Young. 2018;28(6):1–5. doi:10.1017/S104795111800042228803588
- Lee MY, Kim YJ, Lee HJ, et al. Mean platelet volume in mycobacterium tuberculosis infection. Biomed Res Int. 2016;7508763.27419136
- Baxendell K, Walelign S, Tesfaye M, et al. Association between infection with Helicobacter pylori and platelet indices among school-aged children in central Ethiopia: a cross-sectional study. BMJ Open. 2019;9(4):e027748. doi:10.1136/bmjopen-2018-027748
- Robbins G, Barnard DL. Mean platelet volume changes in infection. J Clin Pathol. 1983;36(11):1320. doi:10.1136/jcp.36.11.1320-a