
Abstract
Primary cauda equina lymphoma is an extremely rare entity previously documented in only 24 reported cases. Primary cauda equina lymphoma represents a subtype of neurolymphomatosis, which occurs when lymphoma cells with neurotropism infiltrate and destroy peripheral nerves, spinal nerve roots, nerve plexuses and cranial nerves. The cauda equina is an anatomic structure located in the lower part of the spinal canal consisting of multiple lumbar and sacral nerve roots. Herein, we report a unique case of primary cauda equina diffuse large B-cell lymphoma presenting as a tumor mass in the lower spinal canal, which was treated with a CNS-centric treatment approach followed by autologous hematopoietic stem cell transplantation.
Introduction
In rare instances, malignant lymphoma cells can be discovered as primary lesions originating within the spinal cord, and even more rarely, within the cauda equina itself. The cauda equina is an anatomic structure in a crowded lower spinal canal consisting of multiple lumbar and sacral nerve roots. Primary cauda equina lymphoma (PCEL) presents as a primary lesion within the cauda equina, and has only been reported in a limited number of case reports. PCEL represents an extremely rare and distinct subcategory of neurolymphomatosis. Neurolymphomatosis is a rare lymphomatous manifestation in which lymphoma cells with neurotropism infiltrate and destroy peripheral nerves, spinal nerve roots, nerve plexuses and cranial nerves. Histologically, the majority of neurolymphomatosis cases involve B cell lymphomas, with previous studies documenting frequencies of B-cell involvement as high as 82% and 97.5%.Citation1–Citation3 Occurring less frequently, T-cell lymphomas have been found to range anywhere from 2.5% to 10% of cases.Citation1,Citation3 Typically presenting due to secondary involvement from systemic lymphoma, primary neurolymphomatosis is extremely rare. PCEL appears to comprise less than 1% of neurolymphomatosis cases.Citation2 We report a unique case in which diffuse large B-cell lymphoma involved multiple nerve roots in the cauda equina, presenting as a large tumor occupying the lower spinal canal. Moreover, we describe and highlight the unique treatment approach incorporated in the case of our patient.
Case Presentation
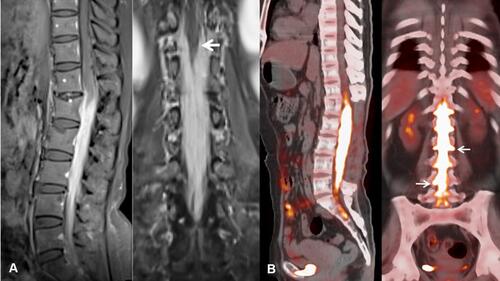
A 55 year-old Asian female patient presented to an outside facility with complaints of tingling, numbness, and significant pain radiating into both lower extremities. Her pain was accompanied by loss of bowel and bladder function as well as significant weakness in both legs resulting in multiple falls, inability to ambulate and subsequent wheel-chair dependency. She further complained of consistent radicular pain radiating around her abdomen. Initial magnetic resonance imaging (MRI) of the lumbar spine identified a homogeneously enhancing mass diffusely infiltrating the cauda equina and filum terminale, superiorly encasing the conus medullaris (). PET-CT scan of the whole body revealed a markedly hypermetabolic tumor occupying the spinal canal and nerve root sleeves from T12 to S1 with no evidence of the disease outside the spine ().
Figure 1 (A) Gadolinium enhanced sagittal and coronal T1 MRI showing diffuse involvement of cauda equina with encasement of conus medullaris (arrows). (B) Staging whole-body 18F-FDG PET-CT coronal and sagittal views showing hypermetabolic mass in the cauda equina and lumbar nerve root sleeves (arrows).
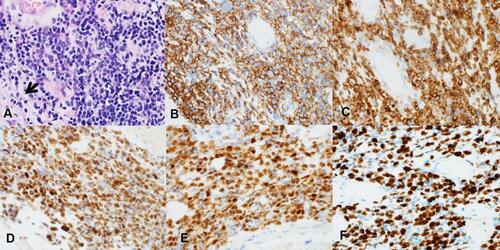
The patient underwent L1-L4 lumbar laminectomy with biopsy of the tumor. Hematoxylin and eosin (H&E) sections of the tumor demonstrated diffusely infiltrating large atypical lymphocytes encasing the lumbar nerve (). Immunohistochemical (IHC) studies showed that the neoplastic lymphocytes were positive for CD20, CD79a, BCL6, BCL2, and MUM1 (–); negative for CD10, TdT, cyclin D1, and MYC. The proliferative rate by ki-67 was also high (>90%) (). Fluorescence in situ hybridization (FISH) analysis from resected tissue was negative for MYC and BCL2 rearrangement, but positive for BCL6 rearrangement in 80% of nuclei. Cerebrospinal fluid (CSF) cytology was positive for lymphoma cells. These findings were consistent with activated B cell subtype of diffuse large B-cell lymphoma (ABC-DLBCL). A bone marrow aspirate and biopsy were negative for lymphomatous involvement.
Figure 2 (A) Pathology examination by H&E staining revealing diffusely infiltrating large atypical lymphocytes dissecting through the nerve bundles (arrow indicating residual nerve). IHC studies showed that the neoplastic lymphocytes were positive for (B) CD20, (C) BCL2, (D) BCL6, (E) MUM1, (F) with a high proliferate rate (>90%) by Ki-67.
The patient was subsequently initiated on systemic therapy with rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) with mid-cycle high-dose methotrexate (HD-MTX). After completing 5 cycles of treatment, restaging MR of the spine and PET-CT scans revealed some residual hypermetabolic abnormalities within the spine despite improved resolution of the spinal lesion. It was at this time that the patient presented to our department for further management and evaluation for potential autologous stem cell transplant. Although her neurological status seemed to be somewhat improved with increased strength in her lower extremities, the patient continued to endorse sensory symptoms in the lower extremities and abdomen as well as significant weakness in her right lower extremity. These clinical findings in combination with restaging PET scan indicated a partial response to previous treatment with R-CHOP and HD-MTX.
She was then initiated on consolidation treatment with 2 cycles of methotrexate, cytarabine, thiotepa, and rituximab (MATRIX) chemoimmunotherapy due to previously reported success of MATRIX therapy in patients with primary central nervous system lymphoma (PCNSL).Citation4 Following the first cycle of MATRIX, the patient reported significant improvement in symptoms as her legs felt much stronger and she was finally able to ambulate on her own with the assistance of a walker. Restaging following MATRIX therapy with PET-CT, MRI of the brain, and MRI of the spine revealed complete resolution of the original lesion with no evidence of disease elsewhere in the body (). She then underwent high-dose Bis-chloroethyl nitrosourea (BCNU) plus thiotepa followed by autologous hematopoietic stem cell transplantation (auto-SCT). Restaging after auto-SCT with MRI of the thoracic and lumbar spine at day +100 continued to reveal no evidence of disease. She was then initiated on maintenance therapy with Ibrutinib 560 mg daily. At 18 months following the initial diagnosis, the patient has remained in complete remission and her neurological status has greatly improved with regaining of her right lower extremity strength with the help of intensive physical therapy.
Figure 3 Follow up MRI (A) and PET-CT (B) after chemotherapy showing complete resolution of the hypermetabolic cauda equina lesion. Linear FDG uptake in the posterior lumbar dura (arrows) is postoperative in nature.

Discussion and Literature Review
The clinical and pathologic findings for our patient are most consistent with PCEL with CSF involvement. Her presenting neurological findings fit the classical presentation of cauda equina syndrome. Radiologic review of her imaging scans from the time of initial presentation did not show any evidence of intramedullary involvement of the spinal cord, but they did reveal a mass encasing multiple nerve roots in the cauda equina. Unlike typical neurolymphomatosis which most commonly represents a challenging diagnostic entity due to patchy nerve involvement requiring multiple biopsies and investigations over time,Citation5,Citation6 our patient presented with a solid tumor due to lymphomatous involvement of multiple nerve roots in the cauda equina region in a tight spinal canal. This unique presentation, in contrast to most cases of neurolymphomatosis, allowed for a more expedient diagnosis and prevented any delays in treatment. The pathologic findings in our case were consistent with activated B cell subtype of DLBCL associated with BCL6 translocation. The immunophenotype is similar to that of PCNSL; there was positive expression of CD20, BCL6, and MUM1.
Our patient was initially treated with R-CHOP with mid-cycle HD-MTX achieving a partial response. Under our care, she was further treated with two cycles of MATRIX resulting in complete remission. Although radiation therapy was originally offered to the patient as an alternative consolidation therapy, the patient declined any radiation therapy and elected to undergo high-dose chemotherapy followed by auto-SCT. Since it is well known that PCNSL is more amenable to cure at initial diagnosis that in the relapsed/refractory setting, we believed that it was critical for our patient to receive CNS penetrating agents to ensure that the entire CNS was permeated with therapeutic agents. Because we felt that she did not receive good CNS coverage during her initial induction treatment, it was decided that she receive consolidation therapy with two cycles of MATRIX therapy. She was further consolidated with high-dose BCNU and Thiotepa chemotherapy followed by auto-SCT. She has remained in complete remission following the transplant. We decided to put her on maintenance Ibrutinib as her lymphoma was aggressive with significant neurological impacts. Ibrutinib has previously shown significant therapeutic efficacy in ABC-DLBCL and PCNSL with excellent CNS penetration.Citation7–Citation11 It is also pertinent to emphasize the importance of the role of intensive physical therapy, which tremendously helped our patient during her recovery.
Our medical literature review identified 25 PCEL patients () with a median age of 55.5 years (range 11–79) at the time of diagnosis and a 3:2 male to female predominance.Citation12–Citation34 Of those cases that describe lymphoma type, 91% (22/24) classify as B-cell lymphoma whereas only 9% (2/24) describe lymphomas that are T-cell in origin. Diffuse large B-cell lymphoma clearly appears to be the most common subtype as it comprises 77% of those lymphomas that are B-cell in nature and 72% of all PCEL cases in general (17/24). It is also worth noting that over half of patients presented with a mass-like lesion in the cauda equina region on imaging of the spine (62.5%, 15/24) and CSF involvement by lymphoma was reflected on cytology in more than half of cases when lumbar puncture was performed (52.6%, 10/19). Of the 23 cases which included descriptions of treatment, the most common method of treatment appears to be both chemotherapy and radiation (56.5%), followed by chemotherapy (30.4%), and lastly radiation (4.3%), tumor resection (4.3%), and oral steroids (4.3%). Similar to the standard treatment of lymphoma with CNS involvement, the majority of chemotherapy regimens in PCEL patients included CNS penetrating agents, including high dose methotrexate and cytarabine. The death rate at the time of publication in this review appears to be 34.8% (8/23). Of those patients that survived longer than a year, the large majority were treated with systemic chemotherapy incorporating CNS penetrating agents (85.7%, 12/14). Our case appears to be the first to incorporate MATRIX therapy for CNS penetration as well as the only report to include auto-SCT as part of the treatment for PCEL.
Table 1 Traits of 25 PCEL Patients Reported in the Literature
Conclusion
In conclusion, PCEL is a rare, yet frequently aggressive lymphoma that can manifest as a mass lesion in the lower spinal canal. The congregation and conglomeration of multiple nerve roots involved by neurolymphomatosis in a tight anatomical space helps facilitate a proper diagnosis and prevents delays in treatment. We propose that PCEL should be treated like PCNSL, with regimens consisting of CNS-penetrating agents. CNS-penetrating high-dose chemotherapy followed by auto-SCT should be considered in eligible patients.
Ethics and Consent
Written informed consent was obtained from the patient for the publication of this manuscript and any accompanying images. Institutional approval was not required for publication.
Disclosure
Dr Han W Tun reports grants, personal fees from Acrotech pharmaceutical, grants from Celgene, grants from Bristol Myers Squibb, grants from Mundipharma, grants from TG Therapeutic, grants from Curis, grants from Zhejiang DTRM Biopharma, outside the submitted work. In addition, Dr Han W Tun has a patent 9464093 (USA), a patent 9839632 (USA), and a patent 10301273 (USA). The authors declare that there are no other conflicts of interest regarding the publication of this manuscript.
Additional information
Funding
References
- Grisariu S, Avni B, Batchelor TT, et al. Neurolymphomatosis: an international primary CNS lymphoma collaborative group report. Blood. 2010;115(24):5005–5011.
- Baehring JM, Damek D, Martin EC, Betensky RA, Hochberg FH. Neurolymphomatosis. Neuro Oncol. 2003;5(2):104–115. doi:10.1215/15228517-5-2-104
- Novo M, Nowakowski G, Micallef I, Ristow K, Habermann T, Johnston P. Clinical features, treatment and outcome of neurolymphomatosis: single institution experience. Age. 2019;60:37–83.
- Ferreri AJ, Cwynarski K, Pulczynski E, et al. Chemoimmunotherapy with methotrexate, cytarabine, thiotepa, and rituximab (MATRix regimen) in patients with primary CNS lymphoma: results of the first randomisation of the International Extranodal Lymphoma Study Group-32 (IELSG32) Phase 2 trial. Lancet Haematol. 2016;3(5):e217–e227. doi:10.1016/S2352-3026(16)00036-3
- Keddie S, Nagendran A, Cox T, et al. Peripheral nerve neurolymphomatosis: clinical features, treatment, and outcomes. Muscle Nerve. 2020;62(5):617–625. doi:10.1002/mus.27045
- Li V, Jaunmuktane Z, Cwynarski K, Carr A. Diagnostic delay in a case of T-cell neurolymphomatosis. BMJ Case Rep. 2019;12(12):e232538. doi:10.1136/bcr-2019-232538
- Grommes C, Pastore A, Gavrilovic I, et al. Single-Agent Ibrutinib in Recurrent/Refractory Central Nervous System Lymphoma. Washington, DC: American Society of Hematology; 2016.
- Grommes C, Younes A. Ibrutinib in PCNSL: the curious cases of clinical responses and aspergillosis. Cancer Cell. 2017;31(6):731–733. doi:10.1016/j.ccell.2017.05.004
- Lionakis MS, Dunleavy K, Roschewski M, et al. Inhibition of B cell receptor signaling by ibrutinib in primary CNS lymphoma. Cancer Cell. 2017;31(6):833–843. e835. doi:10.1016/j.ccell.2017.04.012
- Soussain C, Choquet S, Blonski M, et al. Ibrutinib monotherapy for relapse or refractory primary CNS lymphoma and primary vitreoretinal lymphoma: final analysis of the Phase II ‘proof-of-concept’iLOC study by the Lymphoma study association (LYSA) and the French oculo-cerebral lymphoma (LOC) network. Eur J Cancer. 2019;117:121–130.
- Wilson WH, Young RM, Schmitz R, et al. Targeting B cell receptor signaling with ibrutinib in diffuse large B cell lymphoma. Nat Med. 2015;21(8):922–926. doi:10.1038/nm.3884
- Beitzke M, Enzinger C, Beitzke D, Neureiter D, Ladurner G, Fazekas F. Primary leptomeningeal lymphoma of the cauda equina: a rare cause of radiculopathy. J Neurol. 2010;257(10):1734–1737. doi:10.1007/s00415-010-5574-8
- Belcastro V, Bellcocchi S, Patriarca C, et al. Cauda equina syndrome due to large B-cell lymphoma: a case report. Neurol Sci. 2016;37(5):825–827. doi:10.1007/s10072-015-2470-0
- Broen M, Draak T, Riedl RG, Weber WE. Diffuse large B-cell lymphoma of the cauda equina. Case Rep. 2014;2014:bcr2014205950.
- Cugati G, Singh M, Symss NP, Pande A, Vasudevan M, Ramamurthi R. Primary spinal intradural extramedullary lymphoma causing cauda equina syndrome. J Craniovertebr Junction Spine. 2012;3(2):58. doi:10.4103/0974-8237.116538
- Giobbia M, Carniato A, Scotton P, Vaglia A, Marchiori G. Primary EBV-associated cauda equina lymphoma. J Neurol. 1999;246(8):739–740. doi:10.1007/s004150050445
- Iwasaki M, Hida K, Yano S, Aoyama T, Kaneko S, Iwasaki Y. Primary cauda equina lymphoma treated with high-dose methotrexate. Neurol Med Chir (Tokyo). 2012;52(9):679–683. doi:10.2176/nmc.52.679
- Khong P, Pitham T, Owler B. Isolated neurolymphomatosis of the cauda equina and filum terminale: case report. Spine. 2008;33(21):E807–E811. doi:10.1097/BRS.0b013e31818441be
- Klein P, Zientek G, VandenBerg SR, Lothman LE. Primary CNS lymphoma: lymphomatous meningitis presenting as a cauda equina lesion in an AIDS patient. Can J Neurol Sci. 1990;17(3):329–331. doi:10.1017/S0317167100030687
- Knopp EA, Chynn KY, Hughes J. Primary lymphoma of the cauda equina: myelographic, CT myelographic, and MR appearance. Am J Neuroradiol. 1994;15(6):1187–1189.
- Kumar N, Dyck PJB. Hypertrophy of the nerve roots of the cauda equina as a paraneoplastic manifestation of lymphoma. Arch Neurol. 2005;62(11):1776. doi:10.1001/archneur.62.11.1776
- Mauney M, Sciotto CG. Primary malignant lymphoma of the cauda equina. Am J Surg Pathol. 1983;7(2):185–190. doi:10.1097/00000478-198303000-00009
- Morita M, Osawa M, Naruse H, Nakamura H. Primary NK/T-cell lymphoma of the cauda equina: a case report and literature review. Spine. 2009;34(24):E882–E885. doi:10.1097/BRS.0b013e3181b29de6
- Nakashima H, Imagama S, Ito Z, et al. Primary cauda equina lymphoma: case report and literature review. Nagoya J Med Sci. 2014;76(3–4):349.
- Nishida H, Hori M, Obara K. Primary B-cell lymphoma of the cauda equina, successfully treated with high-dose methotrexate plus high-dose cytarabine: a case report with MRI findings. Neurol Sci. 2012;33(2):403–407. doi:10.1007/s10072-011-0752-8
- Ooi G, Peh W, Fung C. Magnetic resonance imaging of primary lymphoma of the cauda equina. Br J Radiol. 1996;69(827):1057–1060. doi:10.1259/0007-1285-69-827-1057
- Sasaki R, Ohta Y, Yamada Y, et al. A case of neurolymphomatosis in the cauda equina diagnosed by an open biopsy. Intern Med. 2019;1018–1049.
- Shin HK, Oh SK, Woo CG, Huh JR, Suh CW, Jeon SR. Cauda equina lymphoma mimicking non-neoplastic hypertrophic neuropathy of the cauda equina: a case report. Br J Neurosurg. 2016;30(6):678–680. doi:10.3109/02688697.2015.1111295
- Suzuki K, Yasuda T, Hiraiwa T, Kanamori M, Kimura T, Kawaguchi Y. Primary cauda equina lymphoma diagnosed by nerve biopsy: a case report and literature review. Oncol Lett. 2018;16(1):623–631.
- Tajima Y, Sudo K, Matumoto A. Malignant lymphoma originating in the cauda equina mimicking the inflammatory polyradiculoneuropathy. Intern Med. 2007;46(13):1029–1032. doi:10.2169/internalmedicine.46.0005
- Teo MK, Mathieson C, Carruthers R, Stewart W, Alakandy L. Cauda equina lymphoma–a rare presentation of primary central nervous system lymphoma: case report and literature review. Br J Neurosurg. 2012;26(6):868–871. doi:10.3109/02688697.2012.697225
- Toner GC, Holmes R, Sinclair RA, Tang S, Schwarz MA. Central nervous system lymphoma: primary lumbar nerve root infiltration. Acta Haematol. 1989;81(1):44–47. doi:10.1159/000205399
- Wang G, Liu Y, He F. Primary lymphoma involving cranial nerves and cauda equina detected by 18F-FDG PET/CT and MRI. Nuklearmedizin. 2016;55(05):N46–N48. doi:10.1055/s-0037-1616497
- Zagami A, Granot R. Non-Hodgkin’s lymphoma involving the cauda equina and ocular cranial nerves: case reports and literature review. J Clin Neurosci. 2003;10(6):696–699. doi:10.1016/S0967-5868(03)00089-4