
Abstract
Purpose
Our study aims to describe the mortality trends and disparities among individuals with thalassemia in the United States (US).
Patients and Methods
We used CDC WONDER database to calculate the age-adjusted mortality rates (AAMRs) per 1,000,000 individuals and used the Joinpoint Regression Program to measure the average annual percent change (AAPC). Subgroup evaluations were performed by sex, age, race, census region, and urbanization level.
Results
From 1999 to 2020, there were 2797 deaths relatd to thalassemia in the US. The AAMR of thalassemia-related death showed a decreasing trend from 0.50 (95% CI, 0.41–0.58) in 1999 to 0.48 (95% CI, 0.41–0.55) in 2020 with the AAPC of −1.42 (95% CI, −2.42, −0.42). Asians have the highest AAMR (1.34 [95% CI, 1.20–1.47]), followed by non-Hispanic Blacks (0.65 [95% CI, 0.59–0.71]), non-Hispanic Whites (0.32 [95% CI, 0.30–0.33]), and Hispanics (0.11 [95% CI, 0.08–0.14]). Cardiovascular disease remains the leading cause of death among individuals with thalassemia. The urban population has a higher AAMR than the rural population (0.43 [95% CI, 0.41–0.45] vs 0.29 [95% CI, 0.26–0.32]).
Conclusion
Our study calls for targeted interventions to address the racial and geographic disparities existed among individuals of thalassemia in the US.
Introduction
Thalassemias are a group of hereditary blood disorders resulting from decreased and/or defective α or β globin proteins in the hemoglobin as a result of gene mutation.Citation1 Hemoglobin is the primary oxygen carrier in the red blood cells. The dominant hemoglobin molecule in adults, known as HbA was made up of two α globin chains and two β globin chains. In thalassemia, the abnormal or low levels of α or β globin proteins disrupt the normal functioning of hemoglobin, leading to impaired erythropoiesis and anemia of varying severity among the affected individuals.Citation2
Thalassemias are one of the most common causes of inherited anemia worldwide.Citation3 Approximately 56,100 infants are born with thalassemia annually, of whom more than half of them have transfusion-dependent β-thalassemia.Citation4 Generally, thalassemia was known to be highly prevalent in certain regions of the world, including Southeast Asia, the Mediterranean area, the Middle East, and Africa.Citation5 However, there is an increasing trend of prevalence in the other regions, namely North America and Northern Europe attributed to migrations.Citation6 In the United States, there was 7.5% increase in the prevalence of thalassemia in the last fifty years.Citation7
Patients with thalassemia have varying presentation ranging from asymptomatic or mild anemia among patients with thalassemia trait to severe anemia requiring lifelong blood transfusion among thalassemia major patients. As a result of regular blood transfusion, patients may develop complications from iron deposition in multiple organs and tissues, including cardiac myocytes, liver, pancreas and other endocrine tissues. Over the last two decades, there have been some advances in the treatment of thalassemia, including the introduction of iron chelators, the use of luspatercept in reducing blood transfusion requirement,Citation8 and the recent approval of betibeglogene autotemcel gene therapy for transfusion-dependent beta-thalassemia major.Citation9
With the increasing prevalence of thalassemia in the US, it remains uncertain of the mortality trends among individuals with thalassemia in the US. In addition, the advances in treatment does not always necessarily translate to improve outcomes at the population level due to the disparities existed across the population. Our study aimed to assess the causes of death and mortality trends among individuals with thalassemia, as well as the disparities among different demographics in the US.
Materials and Methods
Data Source
Centers for Disease Control and Prevention’s Wide-Ranging Online Data for Epidemiologic Research (CDC WONDER) is a publicly available online database that contains public health data, including mortality data since the year 1999. We utilized the death certificate data in the CDC WONDER from 1999 to 2020 to examine the longitudinal trends of thalassemia-related mortality among the US population at all ages. Patients with thalassemia were identified using the code in the International Statistical Classification of Diseases and Related Health Problems-10th Revision (ICD-10). We excluded patients with unspecified ages and unspecified contributing causes of death. No prior institutional review approval is required as the data has been deidentified and is publicly available.
Using the CDC WONDER from 1999–2020, we first evaluated the demographics for mortality in thalassemia patients. We selected thalassemia as the contributing cause of death and measured the age-adjusted mortality rates, which were standardized to 2000 US census proportions.
The World Health Organization defines the contributing cause of death as any cause of death that is neither the direct, intervening, originating antecedent nor an underlying cause of death.Citation10 The demographic features were used to stratify the study population based on sex, age, race, and geographic region of residence at the time of death. This study methodology has been validated in similar research topics.Citation11,Citation12
Data Description
We utilized Microsoft Excel to organize the data into line graphs to show the overall AAMR trends of the individuals with thalassemia over the study period. We then grouped the data based on different demographic characteristics including sex, race, age, US census region, and urbanization level and used Microsoft Excel to exhibit the mortality trends among different groups. Joinpoint trend analysis was performed to determine the average annual percent change (AAPC) in the overall thalassemia-related mortality trends. Due to the smaller sample size of the study population when they were grouped under different demographic characteristics, percentage change from the period of 1999–2010 to 2011–2020 was calculated to compare the changes in the AAMR trends in these 2 periods.
Study Outcomes
The age-adjusted mortality rates (AAMRs) per 1,000,000 individuals were standardized for the year 2000 US census population. We compared the AAMRs in different sex, age, race, and geographic regions. For geographical variations, we cross-examined the AAMRs across different states, US census regions, and urbanization. The study population was categorized into urban (large central metro, large fringe metro, medium metro, and small metro counties) and rural (micropolitan non-metro and non-core non-metro counties) according to the 2013 US Census Classifications.Citation13
Ethics Approval and Consent
Our study does not require institutional review approval as the population data is de-identified and publicly available.
Results
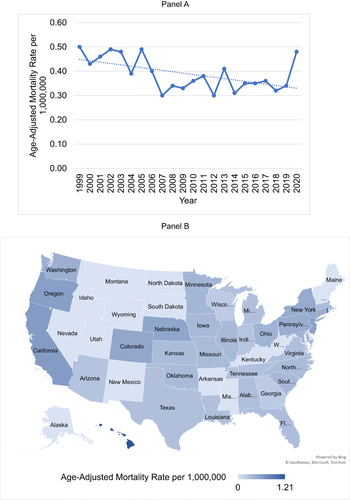
From 1999 to 2020, there were 2797 deaths related to thalassemia, of which 1222 (43%) were male and 1575 (56%) were female. Out of 2797 deaths, there are 1857 (66%) deaths from thalassemia of unspecified types. When deaths from thalassemia of unspecified types were excluded, there were 700 (n=700/940, 74%) beta thalassemia deaths, 169 (n=169/940, 18%) alpha thalassemia deaths, and 71 (n= 71/940, 8%) thalassemia traits deaths. The baseline demographics of patients who met the inclusion criteria are shown in . Overall, the AAMRs decreased from 0.50 (95% CI, 0.41–0.58) per 1,000,000 individuals in 1999 to 0.34 (95% CI, 0.28–0.40) in 2019, then increased to 0.48 (95% CI, 0.41–0.55) in 2020, with the AAPC of −1.42 (95% CI, −2.42, −0.42) (p < 0.01) ().
Table 1 Demographic Characteristics of Thalassemia-Related Death in the United States, 1999–2020
Figure 1 (A) Trend of age-adjusted mortality rate of thalassemia-related death between 1999 to 2020. (B) Overall age-adjusted mortality rate of thalassemia-related death stratified by states.
Causes of Death
Among individuals with thalassemia, the leading underlying causes of mortality when stratified by organ systems are cardiovascular (n=727, 26%), followed by hematological (n=579, 21%), malignancy (n=499, 18%), endocrine (n=176, 6%), respiratory (n=173, 6%), nervous (n=141, 5%), gastrointestinal (n=46, 5%), psychiatry (n=91, 3%), infection (n=84, 3%), and other systems (n=186, 7%) (). When the cardiovascular causes were further stratified, ischemic heart disease (n=309/727, 43%) was the most common reason, followed by hypertensive disease (n=83/727, 11%), cerebrovascular disease (n=48/727, 7%), aortic valve disease (n=30/727, 4%), cardiomyopathy (n=22/727, 3%), and atrial fibrillation and flutter (n=22/727, 3%). When the hematological causes were stratified, thalassemia (n=254/579, 43.9%) and sickle cell anemia (n=37/579, 6%). The three most common malignancies among individuals with thalassemia are lung or bronchus cancer (n=90/499, 18.4%), followed by myelodysplastic syndrome (n=42/499, 8.4%) and breast cancer (n=35/499, 7.0%).
Table 2 Underlying Causes of Death Among Individuals with Thalassemia in the United States, 1999–2020
Race and Age
Most of the deaths occurred in non-Hispanic Whites (n=1820, 65.1%), followed by non-Hispanic Blacks (n=489, 17.5%), Asians (n=395, 14.1%), and Hispanics (n=73, 2.61%). The highest AAMR was observed among Asians (1.34 [95%, 1.20–1.47] per 1,000,000 individuals), followed by non-Hispanic Blacks (0.65 [95% CI, 0.59–0.71] per 1,000,000 individuals), non-Hispanic Whites (0.32 [95% CI, 0.30–0.33] per 1,000,000 individuals), and Hispanics (0.11 [95% CI, 0.08–0.14] per 1,000,000 individuals) ().
Our study shows that the AAMR of patients with thalassemia increased with age. The highest AAMR was observed among patients aged 80 and above (0.17 [95% CI, 0.17–0.17] per 1,000,000 individuals), followed by patients aged 60–79 years (0.09 [95% CI, 0.09–0.09] per 1,000,000 individuals), patients aged 40–59 years (0.05 [95% CI, 0.05–0.05] per 1,000,000 individuals), patients aged 20–39 years (0.04 [95% CI, 0.04–0.04] per 1,000,000 individuals), and patients aged <20 years (0.03 [95% CI, 0.03–0.03] per 1,000,000 individuals).
Geographic Regions
When stratified by state, California had the largest percentage of deaths of individuals with thalassemia (n=487, 17.4%), followed by New York (n=221, 7.9%), and Florida (n=175, n=6.3%). The highest AAMR was observed in Hawaii (1.21 [95% CI, 0.86–1.65]) per 1,000,000 individuals), followed by Rhode Island (0.90 [95% CI, 0.58–1.32]) per 1,000,000 individuals), and California (0.61 [95% CI, 0.55–0.66]) per 1,000,000 individuals) ().
By US census region, the West recorded the highest AAMR at 0.53 (95% CI, 0.49–0.56) per 1,000,000 individuals, whereas the South recorded the lowest AAMR at 0.31 (95% CI, 0.28–0.33) per 1,000,000 individuals. The smallest decrease in AAMR was also observed in the West at −4.00% and the greatest decrease in AAMR was observed in the Midwest.
In terms of urbanization, the urban population had a higher AAMR compared to the rural population (0.43 [95% CI, 0.41–0.45] per 1,000,000 individuals vs 0.29 [95% CI, 0.26–0.32] per 1,000,000 individuals). Despite having a lower AAMR compared to the urban population, the rural population exhibited an increasing trend in the AAMR (+6.90%). On the contrary, the urban population exhibited a decreasing trend of AAMR from 1999–2010 to 2011–2020 (−11.36%).
Discussion
Our study provides important insights into the trends for thalassemia-related mortality in the US. Our study shows that (1) there is a decreasing trend in thalassemia-related mortality; (2) cardiovascular cause is the most common underlying cause of death among individuals with thalassemia; (3) Asians had the highest AAMR compared to other races; (4) urban population and the West had a higher AAMR compared to their counterparts.
Our study demonstrates a decreasing trend of thalassemia-related mortality from 1999 to 2019, and an increasing trend from 2019 to 2020. The initial decreasing trend of mortality rate could be multifactorial. First, alpha- and beta-thalassemia were often detected in the universal newborn screening programs that initially aimed to screen for sickle cell disease since 2006.Citation14,Citation15 Besides, the approval of iron chelators, namely deferasirox and deferiprone in the US in 2005 and 2011 respectively, delays the development of iron-induced cardiac toxicity which may lead to heart failure and arrhythmia.Citation16,Citation17 As cardiovascular causes are the most common cause of death among patients with thalassemia, the declining death rate among patients with thalassemia can also be related to the declining death rate attributed to ischemic heart disease in the last two decadesCitation18 as a result of the increased availability of preventive interventions and advancements in therapy.Citation19 We propose that the later upward trend in mortality may be attributed to the impacts of the COVID-19 pandemic.
Our study found that cardiovascular cause, hematological cause, and malignancy are the three most common causes of death, comprised of more than half of the deaths among individuals with thalassemia. It was observed that cardiovascular causes are the most common cause of death among individuals with thalassemia, similar to the general population.Citation20 This is consistent with the existing studies which show heart diseases are the leading causes of death for both thalassemia major patientsCitation21,Citation22 and non-transfusion-dependent thalassemia.Citation23 There are multiple explanations for this. Individuals with thalassemia were similarly burdened by cardiovascular risk factors eg, hypertension, dyslipidemia, and diabetes mellitus like the general population.Citation24 Besides, individuals with transfusion-dependent thalassemia are prone to develop cardiac complications from iron overload, including sudden cardiac death, arrhythmia, and heart failure.Citation25 Similar to the general population, lung and bronchus cancer and breast cancer are the leading causes of cancer death in our study population.Citation26 Myelodysplastic syndrome is found to be one of the common causes of cancer death among individuals with thalassemia, which is consistent to a study done by Chung et al.Citation27 It was suggested that iron accumulation from chronic blood transfusion can induce oxidative stress and DNA damage, contributing to the pathogenesis of MDS.Citation28
Besides, our study demonstrates that Asians had the highest AAMR compared to other racial groups. This can be explained by the higher prevalence of thalassemia among the Asians. A previous study found that Asian patients made up more than half of the thalassemia population in North America.Citation29 Asians are predisposed to have thalassemia due to their genetic predisposition such as the deletions of HBA1 or HBA2.Citation30,Citation31 The higher mortality in certain geographic regions such as the West and the urban areas can be related to the immigration patterns of Asians to the United States. The higher mortality in the urban population can also be related to the fact that almost one-third of the Asian immigrants lived in the metropolitan areas from 2015 to 2019.Citation32 The highest mortality was observed in the West, mainly in California. This may be due to the fact that almost half of the US Asian population resides in the West, with about 30% of them in California.Citation33
There are a few limitations in our study. First, the database consists of no clinical and imaging data, therefore we are unable to further characterize the clinical status of the population. Besides, the database has no information at individual levels, such as comorbidity burden, duration of diseases, medical treatments, or prior intervention, which are important confounders for mortality. Despite these limitations, our study sufficiently demonstrates the demographic and temporal mortality trend of patients with thalassemia. It provides valuable insights into the need to improve the outcome of patients with thalassemia.
Conclusion
Current management of thalassemia includes transfusion therapy, use of Luspatercept in reducing transfusion requirement, iron chelation, and curative options like hematopoietic stem cell transplantation (HSCT).Citation34 Population-based study is essential to measure the outcomes of the latest treatment. Besides, our study highlights cardiovascular causes as the predominant cause of mortality among patients with thalassemia. This underscores the need for targeted cardiovascular monitoring and management in this patient population. Although the mortality rate among individuals with thalassemia declined over the years, the disparities existed across different races and geographic regions demonstrated in our study suggested that targeted interventions are required to address the disparities in the mortality trends among the individuals of thalassemia in the US.
Data Sharing and Data Accessibility
The datasets generated during and/or assessed during the current study are available in the CDC WONDER, https://wonder.cdc.gov/
Disclosure
All authors report no conflicts of interest in this work.
Acknowledgments
The abstract of this paper was presented at the American Society of Hematology (ASH) as a poster presentation with interim findings. The poster’s abstract was published in ‘Poster Abstracts’ in Blood: [https://doi.org/10.1182/blood-2023-179572].
Additional information
Funding
References
- Shafique F, Ali S, Almansouri T, et al. Thalassemia, a human blood disorder. Braz J Biol. 2021;83:e246062. doi:10.1590/1519-6984.246062.
- Angastiniotis M, Lobitz S. Thalassemias: an overview. Int J Neonatal Screen. 2019;5(1):16. doi:10.3390/ijns5010016
- Aydinok Y. Thalassemia. Hematology. 2012;17(Suppl 1):S28–31. doi:10.1179/102453312X13336169155295
- Modell B, Darlison M. Global epidemiology of haemoglobin disorders and derived service indicators. Bull World Health Organ. 2008;86(6):480–487. doi:10.2471/blt.06.036673
- Kattamis A, Forni GL, Aydinok Y, Viprakasit V. Changing patterns in the epidemiology of beta-thalassemia. Eur J Haematol. 2020;105(6):692–703. doi:10.1111/ejh.13512
- Colah R, Gorakshakar A, Nadkarni A. Global burden, distribution and prevention of beta-thalassemias and hemoglobin E disorders. Expert Rev Hematol. 2010;3(1):103–117. doi:10.1586/ehm.09.74
- Sayani FA, Kwiatkowski JL. Increasing prevalence of thalassemia in America: implications for primary care. Ann Med. 2015;47(7):592–604. doi:10.3109/07853890.2015.1091942
- Cappellini MD, Viprakasit V, Taher AT, et al. A Phase 3 trial of luspatercept in patients with transfusion-dependent beta-Thalassemia. N Engl J Med. 2020;382(13):1219–1231. doi:10.1056/NEJMoa1910182
- Locatelli F, Thompson AA, Kwiatkowski JL, et al. Betibeglogene autotemcel gene therapy for non–β0/β0 genotype β-Thalassemia. N Engl J Med. 2021;386(5):415–427. doi:10.1056/NEJMoa2113206
- Instructions for Classification of Underlying and Multiple Causes of Death - Section I - 2021. Centers for disease control and prevention. Available from.: https://www.cdc.gov/nchs/nvss/manuals/2a-sectioni-2021.htm#:~:text=Any%20cause%20of%20death%20that,a%20contributory%20cause%20of%20death.&text=Also%20known%20as%20terminal%20cause,(a)%20in%20Part%20I. Accessed Aug 28, 2023.
- Alexander KM, Orav J, Singh A, et al. Geographic disparities in reported us amyloidosis mortality from 1979 to 2015: potential underdetection of cardiac amyloidosis. JAMA Cardiol. 2018;3(9):865–870. doi:10.1001/jamacardio.2018.2093
- Tanaka Y, Shah NS, Passman R, Greenland P, Lloyd-Jones DM, Khan SS. Trends in cardiovascular mortality related to atrial fibrillation in the United States, 2011 to 2018. J Am Heart Assoc. 2021;10(15):e020163. doi:10.1161/JAHA.120.020163
- Kobo O, Van Spall HGC, Mamas MA. Urban-rural disparities in diabetes-related mortality in the USA 1999-2019. Diabetologia. 2022;65(12):2078–2083. doi:10.1007/s00125-022-05785-4
- Bender MA, Yusuf C, Davis T, et al. Newborn screening practices and alpha-Thalassemia detection - United States, 2016. MMWR Morb Mortal Wkly Rep. 2020;69(36):1269–1272. doi:10.15585/mmwr.mm6936a7
- Bender MA, Hulihan M, Dorley MC, Aguinaga MDP, Ojodu J, Yusuf C. Newborn screening practices for beta-Thalassemia in the United States. Int J Neonatal Screen. 2021;7(4):83. doi:10.3390/ijns7040083
- Pepe A, Meloni A, Capra M, et al. Deferasirox, deferiprone and desferrioxamine treatment in thalassemia major patients: cardiac iron and function comparison determined by quantitative magnetic resonance imaging. Haematologica. 2011;96(1):41–47. doi:10.3324/haematol.2009.019042
- Aessopos A, Berdoukas V, Tsironi M. The heart in transfusion dependent homozygous thalassaemia today--prediction, prevention and management. Eur J Haematol. 2008;80(2):93–106. doi:10.1111/j.1600-0609.2007.01018.x
- Sidney S, Quesenberry CP Jr, Jaffe MG, Sorel M, Go AS, Rana JS. Heterogeneity in national U.S. mortality trends within heart disease subgroups, 2000-2015. BMC Cardiovasc Disord. 2017;17(1):192. doi:10.1186/s12872-017-0630-2
- Lanas F, Soto A. Trends in mortality from ischemic heart disease in the region of the Americas, 2000-2019. Glob Heart. 2022;17(1):53. doi:10.5334/gh.1144
- Ahmad FB, Anderson RN. The leading causes of death in the US for 2020. JAMA. 2021;325(18):1829–1830. doi:10.1001/jama.2021.5469
- Forni GL, Gianesin B, Musallam KM, et al. Overall and complication-free survival in a large cohort of patients with beta-thalassemia major followed over 50 years. Am J Hematol. 2023;98(3):381–387. doi:10.1002/ajh.26798
- Zurlo M, De Stefano P, Borgna-Pignatti C, et al. SURVIVAL AND CAUSES OF DEATH IN THALASSAEMIA MAJOR. Lancet. 1989;334(8653):27–30. doi:10.1016/S0140-6736(89)90264-X
- Musallam KM, Vitrano A, Meloni A, et al. Survival and causes of death in 2033 patients with non-transfusion-dependent beta-thalassemia. Haematologica. 2021;106(9):2489–2492. doi:10.3324/haematol.2021.278684
- Vaduganathan M, Mensah GA, Turco JV, Fuster V, Roth GA. The global burden of cardiovascular diseases and risk: a compass for future health. J Am Coll Cardiol. 2022;80(25):2361–2371. doi:10.1016/j.jacc.2022.11.005
- Russo V, Melillo E, Papa AA, Rago A, Chamberland C, Nigro G. Arrhythmias and sudden cardiac death in beta-thalassemia major patients: noninvasive diagnostic tools and early markers. Cardiol Res Pract. 2019;2019:9319832. doi:10.1155/2019/9319832
- Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. 2024;74(1):12–49. doi:10.3322/caac.21820
- Chung WS, Lin CL, Lin CL, Kao CH. Thalassaemia and risk of cancer: a population-based cohort study. J Epidemiol Community Health. 2015;69(11):1066–1070. doi:10.1136/jech-2014-205075
- Hodroj MH, Bou-Fakhredin R, Nour-Eldine W, Noureldine HA, Noureldine MHA, Taher AT. Thalassemia and malignancy: an emerging concern? Blood Rev. 2019;37:100585. doi:10.1016/j.blre.2019.06.002
- Vichinsky EP, MacKlin EA, Waye JS, Lorey F, Olivieri NF. Changes in the epidemiology of thalassemia in north America: a new minority disease. Pediatrics. 2005;116(6):e818–25. doi:10.1542/peds.2005-0843
- Vlok M, Buckley HR, Miszkiewicz JJ, et al. Forager and farmer evolutionary adaptations to malaria evidenced by 7000 years of thalassemia in Southeast Asia. Sci Rep. 2021;11(1):5677. doi:10.1038/s41598-021-83978-4
- (MD) B. Genes and Disease [Internet]. National Center for Biotechnology Information (US). Available from: https://www.ncbi.nlm.nih.gov/books/NBK22200/. Accessed Aug 21, 2023.
- Mary Hanna JB Immigrants from Asia in the United States. Migration Policy Institute. Available from: https://www.migrationpolicy.org/article/immigrants-asia-united-states-2020#:~:text=In%20the%202015%2D19%20period,residing%20in%20the%20United%20States. Accessed Sep 1, 2023.
- Abby Budiman NGR Key facts about Asian Americans, a diverse and growing population. Available from: https://www.pewresearch.org/short-reads/2021/04/29/key-facts-about-asian-americans/. Accessed Sep 2, 2023.
- Gaziev J, Lucarelli G. Hematopoietic stem cell transplantation for thalassemia. Curr Stem Cell Res Ther. 2011;6(2):162–169. doi:10.2174/157488811795495413