
Abstract
Myelodysplastic syndromes (MDS) represent a heterogeneous group of acquired clonal hematopoietic disorders characterized by peripheral blood cytopenias, paradoxical BM hypercellularity, ineffective hematopoiesis, and increased risk of leukemic transformation. Risk stratification, using different prognostic scores and markers, is at the core of MDS management. Deletion 5q [del(5q)] MDS is a distinct class of MDS characterized by the haploinsufficiency of specific genes, microRNAs, and proteins, which has been linked to increased sensitivity to the drug lenalidomide. Phase II and III clinical trials have demonstrated the efficacy of lenalidomide in improving clinical outcomes of patients with del(5q) MDS, including reduction in red blood cell transfusion requirements and improvements in quality of life. Lenalidomide has also demonstrated some activity in non-del(5q) lower-risk MDS as well as higher-risk MDS, especially in combination with other agents. In this paper, we review the pathogenesis of del(5q) MDS, the proposed mechanisms of action of lenalidomide, the major clinical trials that documented the activity of lenalidomide in different MDS populations, potential predictors of benefit from the drug and suggested mechanisms of resistance, and the use of combination strategies to expand the clinical utility of lenalidomide in MDS.
Introduction
Myelodysplastic syndromes (MDS) include a heterogeneous group of acquired clonal hematopoietic malignancies characterized by an apparent paradox of peripheral blood cytopenias and bone marrow (BM) hypercellularity, ineffective hematopoiesis, and a variably increased risk of leukemic transformation.Citation1,Citation2 While MDS is usually characterized by BM hypercellularity, a minority of patients exhibit BM hypoplasia which can be difficult to distinguish from aplastic anemia.Citation3 MDS incidence increases with age in the general population, and the number of diagnosed cases is expected to increase with the increasing longevity of the population.Citation4–Citation11 Risk stratification is at the core of current MDS management,Citation10–Citation12 and is accomplished using different prognostication schemes that group patients into different risk categories based on factors such as number and severity of cytopenias, karyotypic abnormalities, BM blast percentage, and transfusion dependence.Citation13 The most widely used prognostic scores are the International Prognostic Scoring System (IPSS) and its revised version (IPSS-R), the World Health Organization Classification-Based Prognostic Scoring System, the MD Anderson prognostic schemes, and others.Citation14–Citation20
Only a limited number of therapeutic options currently exist for MDS, and their use is usually guided by clinical risk stratification tools rather than specific biological markers, with the notable exception of the 5q-cytogenetic deletion that predicts particular sensitivity to lenalidomide in lower-risk MDS patients.Citation11–Citation13 Lenalidomide, a thalidomide analog, is an immunomodulatory agent that has demonstrated clinical efficacy in MDS patients with low to intermediate IPSS scores and a deletion in the long arm of chromosome 5 [del(5q)].Citation21,Citation22 Lenalidomide has also demonstrated some activity, although less impressive, in MDS patients outside this group. Several studies have tried to identify factors beyond del(5q) that might predict response to lenalidomide.Citation13 Lenalidomide is also being evaluated in combination with other agents used to treat MDS, including hypomethylating agents in higher-risk MDS patients and erythropoiesis-stimulating agents (ESAs) in lower-risk MDS patients.Citation23,Citation24 This paper reviews the pathogenesis of del(5q) MDS, the proposed mechanisms of action of lenalidomide, the major clinical trials that documented the activity of lenalidomide in different MDS populations, potential predictors of benefit from the drug and suggested mechanisms of resistance, and the use of combination strategies to expand the clinical utility of lenalidomide in MDS.
Pathogenesis of del(5q) MDS
The pathogenesis of del(5q) MDS is likely related to deletion of various genes that are important for normal erythropoiesis and cell cycle regulation.Citation25–Citation28 The long arm of chromosome 5 (5q), particularly the 5q31 region, has a gene cluster that is relevant to hematopoiesis.Citation25 This gene cluster includes interleukin (IL)-3, IL-4, IL-5, IL-9, IL-13, and IL-17β, as well as granulocyte-monocyte colony stimulating factor and several cytokine receptor genes (colony-stimulating factor 1 receptor and platelet-derived growth factor-β).Citation26–Citation28 The hallmark of 5q-syndrome is an isolated interstitial deletion on the long arm of chromosome 5. The 5q-syndrome was first characterized in 1974 by Van Den Berghe et al.Citation29 Clinically, the 5q-syndrome is typically characterized by macrocytic hypoproliferative anemia, hypolobulated micromegakaryocytes, fewer than 5% BM blasts, normal or increased platelet counts, and a tendency to occur in older women.Citation22,Citation30 MDS with isolated del(5q) or with additional chromosomal abnormalities is not entirely clinically equivalent to 5q-syndrome. However, because the 5q-syndrome and MDS associated with del(5q) are both sensitive to lenalidomide, the World Health Organization classification puts them under one special category, ie, MDS with chromosome 5q deletion.Citation31 The 5q-syndrome occurs only in a subgroup of patients with del(5q). The commonly deleted region in 5q-syndrome is 5q32–33. This region is known as the distal common deleted region (CDR). Another region frequently deleted in patients with del(5q) MDS or acute myeloid leukemia (AML) is a 1 to 1.5 megabase region at chromosome 5q31. This region is known as the proximal CDR. Genes in the CDR, their effect, and the potential effects of lenalidomide on the haplodeficient genes are listed in .Citation32
Table 1 Genes in the commonly deleted region, their effect, and potential effects of lenalidomide on the haplodeficient genes
Haploinsufficiency of RPS14
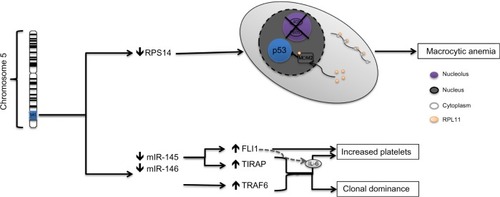
RPS14 is a ribosomal protein essential for the assembly of the ribosomal complex.Citation33 Ebert et al demonstrated that the haploinsufficiency of RPS14 results in erythroid differentiation defects and that its forced expression in cells from patients with 5q-syndrome promotes erythroid differentiation.Citation33 The potential mechanism of how ribosomal haploinsufficiency leads to impaired erythropoiesis is summarized in . It is thought that RPS14 haploinsufficiency interferes with normal ribosomal biosynthesis, leading to accumulation of free ribosomal proteins.Citation34 The free ribosomal proteins bind to murine double minute 2 (MDM2), blocking the binding of MDM2 to p53. This ultimately leads to accumulation of p53in erythroid progenitor cells, increasing apoptosis and impairing erythropoiesis.Citation34,Citation35
Figure 1 Molecular alterations associated with the 5q-syndrome.
Haploinsufficiency of microRNA genes
MicroRNAs (miRNAs) are small noncoding RNA molecules, and are important for inhibiting translation and destabilizing target protein encoding mRNA. Two miRNAs (miR145 and miR146α) are involved in downregulation of genes involved in regulation of the innate immune system.Citation32 The genes for both miRNAs are downregulated in CD34+ cells from del(5q) MDS patients compared with healthy controls.Citation32,Citation36 Haploinsufficiency of these miRNAs will result in upregulation of TIRAP, TRAF6, IRAK1, and IRAK2 (IL-1 receptor-associated kinase 1 and 2, respectively).Citation36 TRAF6 upregulation will lead to increased production of IL-6 and activation of nuclear factor kappa beta.Citation37 Increased IL-6 is thought to lead to abnormal megakaryocytes and the elevated platelet count seen in MDS with 5q-syndrome.Citation37 Activation of nuclear factor kappa beta is thought to lead to clonal dominance (). Starczynowski et al showed that chimeric mouse BM, in which miR145 and miR146α are reduced or TRAF6 is overexpressed, had characteristic megakaryocytic dysplasia, elevated platelets, and clonal dominance similar to what is seen in BM failure or AML.Citation37
Haploinsufficiency of tumor suppressor genes
Haploinsufficiency in several tumor suppressor genes () may contribute to the proliferative advantage of del(5q) clones and lead to hypercellular BM. Among the tumor suppressor genes lost is SPARC, which regulates extracellular interactions and has antiangiogenic, antiproliferative, and antiadhesive properties.Citation38 Other haploinsufficient genes include EGR1, DIAPH1, and NPM-1 ().Citation32
Mechanism of action of lenalidomide
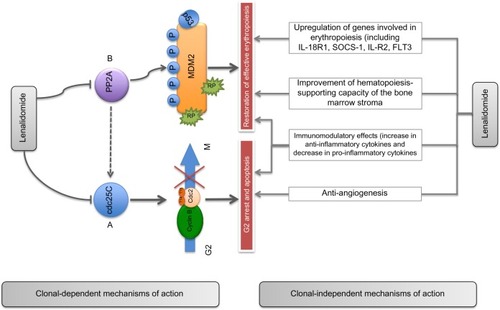
Thalidomide has been historically used in lower-risk MDS, although its use has been limited due to its side effect profile. Limited clinical data have shown that its effect in del(5q) MDS is similar to that in non-del(5q) MDS.Citation39–Citation43 Several in vitro and in vivo studies demonstrated the sensitivity of del(5q) cells to lenalidomide.Citation32 Although the in vivo mechanisms of action of lenalidomide in MDS (particularly del(5q) MDS) are not completely understood, several studies suggest that lenalidomide most probably acts through karyotype-dependent pathways by its impact on haplodeficient genesCitation32 and karyotype-independent pathways by its effect on erythroid differentiation genes, immune function, and angiogenesis ( and ).Citation22,Citation32,Citation34
Figure 2 Suggested mechanism of action of lenalidomide del(5q) MDS.
Effect of lenalidomide on haplodeficient genes and their pathways
Wei et alCitation44 demonstrated that lenalidomide is selectively cytotoxic to del(5q) cells as a result of its direct and indirect inhibition of the haplodeficient phosphatases (CDC25C and PP2A).Citation32 PP2A dephosphorylates CDC25C, enabling mitotic entry. Lenalidomide directly inhibits CDC25C phosphatase and indirectly inhibits PP2A and CDC25A activity. This translates into a higher apoptotic response (G2 arrest) in cells with dual knockdown of CDC25C and PP2Acα-mimicking haplodeficient cells.Citation32 Lenalidomide can reverse the stabilization of p53 that results from haploinsufficiency in RPS14 and exerts dose-dependent inhibitory effects on CDC25C and PP2ACitation44 ( and ). This in turn prevents PP2A from dephosphorylating MDM2. The treatment of PP2Aα-haplodeficient cells with lenalidomide results in concentration-dependent hyperphosphorylation of MDM2, abolishing its autoubiquitination. This will stabilize MDM2 and promote p53 degradation.Citation44 Additionally, lenalidomide upregulates the expression of miRNA-143 and miRNA-145 and also upregulates SPARC expression. Increased SPARC expression normalizes the interaction of del(5q) clones with the extracellular matrix. This might increase the apoptotic activity of lenalidomide in del(5q) cells.Citation32
Effect on BM function
Lenalidomide improves BM function by different mechanisms. By reducing del(5q) clones, it helps accelerate the repopulation of BM by normal cells. In addition to helping decrease abnormal clones, lenalidomide can promote normal hematopoiesis by upregulating several genes important for erythroid differentiation and by improving the hematopoiesis-supporting capacity of the BM stroma ().Citation32,Citation45 Lenalidomide was shown to increase red blood cell (RBC) production.Citation46 Studies demonstrated that primary human CD34+ cells treated with lenalidomide had increased expression of several genes involved in erythropoiesis. Among the genes upregulated by lenalidomide alone or in combination with dexamethasone are FLT3, JAK2, and IL-1R2. These genes have important functions in erythropoiesis. Forced expression of the FLT3 gene confers a proliferative advantage with increasing erythroid differentiation. Increased expression of JAK2 increases the response to erythropoietin.
In addition to increasing the expression of genes important for erythropoiesis in non-del(5q) erythroid precursors, lenalidomide enhances erythropoietin signaling in these cells.Citation47,Citation48 Inhibition of PP2A phosphatase in non-del(5q) erythroid precursors by lenalidomide leads to enhancement of erythropoietin receptor signaling by relieving CD45 repression of ligand-dependent signaling JAK2 and Lyn kinase-mediated STAT5 activation.Citation47,Citation48 This mechanism is thought to be secondary to rearrangements of lipid rafts resulting in incorporation of the erythropoietin receptor and its signaling intermediates such as Lyn kinase and STAT5 into raft domains and in translocation of their principal negative regulator (CD45 protein tyrosine phosphatase) into non-raft membrane fractions.Citation47,Citation48
Effect on immune function and angiogenesis
Altered cytokine production
The immunomodulatory activity of lenalidomide leads to inhibition of production of proinflammatory cytokines, namely IL-1, IL-6, IL-12, and tumor necrosis factor-α, while also leading to upregulated production of anti-inflammatory cytokines, such as IL-10.Citation49 Tumor necrosis factor-alpha is primarily produced by monocytes and macrophages and plays an important role in combating viral and bacterial infections. Its elevation is implicated in stem cell apoptosis and the ineffective hematopoiesis seen in MDS.Citation50,Citation51 Another proinflammatory cytokine decreased by lenalidomide is IL-6. This can help in reversal of the IL-6 upregulation that results from miRNA haploinsufficiency.Citation36
T-cell activation
T-cell activation involves the presentation of antigen by antigen-presenting cells to the T-cell receptor.Citation51 A secondary costimulatory interaction of the B7 molecule on antigen-presenting cells and CD28 on the T-cell surface augments the T-cell response and aids in T-cell proliferation, differentiation, and survival.Citation51 Cereblon is a potential inhibitor of CD28 stimulation.Citation52 Lenalidomide, by suppressing cereblon, might increase functional T-cell activation through the CD28 pathway.Citation52 Increased T-cell activation can lead to increased antileukemic immunosurveillance.Citation52 Alternatively, it may help in removing the suppressive immature cell population from the BM microenvironment, allowing for improved erythropoiesis.Citation52
Antiangiogenic activity
Immunomodulatory agents like thalidomide and lenalidomide have been shown to significantly decrease the expression of the angiogenic factors vascular endothelial growth factor and IL-6.Citation53,Citation54 In MDS patients, blast cells overexpress vascular endothelial growth factor receptors, an observation correlated with lower remission rates.Citation55 The antiangiogenic activity of lenalidomide results in reduced BM vascularity in patients with del(5q) MDS. Reduced BM vascularity in del(5q) has been associated with a clinical response and its loss was found to predict disease progression.Citation32,Citation34,Citation56
Clinical efficacy
Ineffective hematopoiesis is one of the salient features of MDS. Prior to lenalidomide, many MDS patients with anemia secondary to ineffective erythropoiesis were only managed with blood transfusion and/or ESAs, with variable symptomatic responses. The first trial to evaluate the safety and hematological activity of lenalidomide was MDS-001Citation57 (). In this single-center Phase I/II trial, 43 patients with MDS (mostly lower-risk) and symptomatic anemia (defined as hemoglobin <10 g/dL or transfusion dependence requiring at least 4 units of red cells within 8 weeks of enrollment) were enrolled. All patients were refractory to ESAs or had high endogenous erythropoietin levels (>500 mIU/mL), and 12 patients had del(5q). Patients with neutropenia (<500/mm3) or thrombocytopenia (platelet count <10,000/mm3) were excluded. The clinical efficacy and safety of lenalidomide at doses of 25 or 10 mg daily or 10 mg daily for 21 days of every 28-day cycle were assessed. The hematological overall response rate was 56%. RBC transfusion independence (RBC-TI) was achieved in 20/32 patients who were transfusion-dependent. Patients with del(5q) had an overall response rate of 83% versus 53% in patients with non-del(5q) and 12% in patients with other karyotypic abnormalities. The cytogenetic response also correlated significantly with the hematological response.Citation57
Table 2 Summary of the major clinical trials assessing use of lenalidomide in myelodysplastic syndromes
Clinical efficacy in lower risk MDS with del(5q)
The efficacy of lenalidomide in MDS with del(5q) was further investigated in MDS-003 and MDS-004 ().Citation45,Citation58 Both trials included low-risk and intermediate-1 risk IPSS patients and excluded patients with severe neutropenia (<500/mm3) or thrombocytopenia (platelet count <50×103/mm3 in MDS-003 and platelet count <25×109/L in MDS-004). MDS-003 was a single-arm study that included 148 patients requiring transfusion of at least 2 units of blood in the 8 weeks prior to enrollment.Citation45 In total, 111 patients had isolated del(5q) while 37 had del(5q) with additional chromosomal abnormalities. At 24 weeks, the overall response rate was 76%. Among the responders, 99 (67%) achieved RBC-TI. The median time to RBC-TI was 4.6 weeks. The median hemoglobin increase in patients achieving RBC-TI was 5.4 g/dL, and the median duration of RBC-TI was 2.2 (range 1.5–2.9) years.Citation59 Complete cytogenetic response, assessed at week 24 of treatment, was reached in 38/85 patients (45%), while 24/85 (28%) had a partial cytogenetic response, defined as a more than 50% reduction in abnormal metaphases.Citation45 Side effects are summarized in , with myelosuppression being the most prominent. Sixty-two percent of grade 3–4 myelosuppression occurred within the first 8 weeks of treatment. Dose reductions were required in 84% of patients. Thirty patients (20%) discontinued the drug due to adverse events.
The results of the MDS-003 trial were validated further in the randomized, double-blind, placebo-controlled MDS-004 trial.Citation58 MDS-004 randomized 205 patients with lower-risk IPSS, transfusion-dependent MDS, and del(5q) with or without additional cytogenetic abnormalities to receive placebo daily, lenalidomide 5 mg daily, or lenalidomide 10 mg daily for 21 days of 28-day cycles. All patients were transfusion-dependent. RBC-TI for ≥26 weeks was 56.1% with lenalidomide 10 mg, 42.6% with lenalidomide 5 mg, and 5.9% with placebo.Citation58 The cytogenetic response rate was 50% in the 10 mg group and 25% in 5 mg group. Again, myelosuppression was a major side effect reported in MDS-004, with 55.1% of patients in the 10 mg group and 52.2% of those in the 5 mg group requiring dose reduction. The drug was discontinued in 8.7% and 17.4% of patients in the 10 mg and 5 mg groups, respectively.
Quality of life data in lower risk del(5q) MDS
Quality of life was not reported in MDS-003, but was reported in MDS-004 and in a study reported by Oliva et al.Citation60 In the latter study, patients who responded to lenalidomide experienced progressive improvement in their quality of life in the first 24 weeks of therapy. A health-related quality of life outcome analysis from the MDS-004 study demonstrated that the hematological improvements obtained with lenalidomide were associated with improvement in health-related quality of life in both the short term (12 weeks) and the long term (48 weeks).
Progression and survival outcome in lower-risk MDS with del(5q)
New chromosomal abnormalities were observed in a subset of patients treated with lenalidomide (24/148 patients in MDS-003). This raised concerns regarding a potential increase in the incidence of clonal evolution and progression to AML. The results of a long-term follow-up analysis of 42 patients with low-risk or intermediate-risk del(5q) MDS treated with lenalidomide have been published.Citation61 After a median follow-up of 40 months, 36% of patients progressed to AML, and most (87%) acquired additional chromosome aberrations. Responders have a decreased risk of progression. At 5 years, the cumulative incidence of progression to AML for patients with a cytogenetic response was 21% compared with 60% for nonresponders.Citation61 This prompted several groups to perform historical comparisons of the rate of leukemic progression between low-risk del(5q) MDS patients treated before the lenalidomide era and lenalidomide-treated patients. Comparative analysis by the Groupe Francophone des Myélodysplasies found no significant difference in progression of AML between the lenalidomide-treated group and a matched control cohort.Citation62 In this comparative study, 71 lenalidomide-treated patients were matched with 71 patients from a historical control cohort based on propensity score. The control cohort was treated with erythropoietin or thalidomide. The median follow-up from diagnosis for the lenalidomide-treated group was 4 years and that for the control cohort was 6.5 years. There was no statistically significant difference in the 4-year estimated cumulative incidence of AML from diagnosis between the two groups, with a hazard ratio of 0.87 (95% confidence interval 0.27–2.82; P=0.82). The 4-year estimated cumulative incidence in the lenalidomide-treated group was 9% and 15.7% in the matched controls.Citation62
Results from the comparative analysis reported by Kuendgen et al support the above results from Groupe Francophone des Myélodysplasies.Citation63 In the study by Kuendgen et al, long-term clinical outcomes in del(5q) MDS patients treated with lenalidomide in the MDS-003 and MDS-004 trials were compared with a cohort of untreated low-risk or intermediate-1 risk MDS patients with del(5q) not treated with lenalidomide derived from nine MDS registries. The cumulative incidence of progression to AML was 6.9% and 22.8% at 2 and 5 years, respectively, for the lenalidomide-treated group, and 12.1% and 19.9% at 2 and 5 years, respectively, for the group not treated with lenalidomide. Treatment with lenalidomide was not associated with an increased risk of AML progression (hazard ratio 0.9; P=0.930). The median overall survival was higher (5.2 years, 95% confidence interval 4.5–5.9) in the treated group versus 3.8 years (95% confidence interval 2.9–4.8) in nontreated patients.Citation63
Further data about survival and risk of AML progression came from the MDS-003 study investigators, who reported the long-term outcomes of overall survival and AML progression in patients enrolled in the MDS-003 trial.Citation59 After a median follow-up of 3.2 years, median overall survival was 3.3 years and the cumulative one-year and 5-year overall survival rates were 84.2% and 30.4%, respectively. Median overall survival was longer in patients with isolated del(5q) than in patients with del(5q) and additional cytogenetic abnormalities (3.9 years versus 2.7 years, respectively). The mortality rates were lower in patients with RBC-TI for at least 8 weeks compared with nonresponders (58.8% versus 86.3%).Citation59 Patients with RBC-TI for at least 8 weeks had better overall survival rates at one and 5 years than nonresponders (96.8% and 41.1% versus 81.6% and 14% respectively). Cytogenetic response was also associated with a lower mortality rate and better overall survival. Median overall survival was 4.9 years in cytogenetic responders versus 3.1 years in nonresponders.Citation59 When compared with historical controls (MDS patients who received best supportive care), the median overall survival was around one year longer in responders. Patients who achieved RBC-TI for at least 26 weeks and a cytogenetic response had the lowest incidence of AML progression (14%), while those who achieved neither had the highest incidence of AML progression (52.9%).Citation59
Taken together, these observations suggest that hematological and cytogenetic responses in IPSS lower-risk del(5q) anemic MDS patients treated with lenalidomide are possibly associated with Yimproved overall survival and reduced risk of AML progression, but further data are needed. These results are consistent with emerging data suggesting that AML progression rates in patients treated with lenalidomide are probably not drug-related but are associated with additional risk factors as discussed later in the section “Predictors and prognosticators beyond the del(5q) and IPSS”. MDS-003 and MDS-004 are the main studies supporting the use of lenalidomide in the treatment of IPSS lower-risk del(5q) MDS patients who are RBC transfusion-dependent.
Clinical efficacy in higher-risk MDS with del(5q)
The overall response rate to lenalidomide 10–30 mg as a single agent in patients who have IPSS higher-risk MDS with del(5q) is lower than that seen in IPSS low-to-intermediate-1 risk MDS with del(5q).Citation1 The overall response rate in the high-risk population was around 25%–30% and did not differ between patients with del(5q) and non-del(5q).Citation1 In addition, the response was not durable.Citation1 In a Phase II trial,Citation64 47 patients with higher-risk del(5q) MDS received lenalidomide 10 mg/day, and the overall response rate according to the International Working Group 2006 criteria was 27% (13/47). Most of the complete hematological remissions were seen in patients with isolated del(5q). The median duration of response was 6.5 months.Citation64
Strategies have been employed to increase responses in this population, including combining lenalidomide with other agents (see “Combination strategies” section.) or increasing the dose of lenalidomide. Another Phase II trialCitation65 investigated the role of higher doses of lenalidomide in patients who have higher-risk MDS with del(5q). Twenty-nine patients were enrolled in this study (16 with AML, 12 with intermediate-2 or high-risk MDS) who were not candidates for regular induction treatment. The lenalidomide dose was escalated from 10 mg to a target dose of 30 mg at week 10. Ten patients completed 16 weeks of treatment, and five of these patients achieved a major cytogenetic response. The overall response rate in MDS patients was 36% (4/11). Despite the small size of the MDS patient sample, this study showed that a group of patients with high-risk MDS and del(5q) could tolerate and respond to higher doses of lenalidomide.Citation65
Clinical efficacy in non-del(5q) MDS
MDS-001 showed that the overall response rate in anemic patients with non-del(5q) lower-risk MDS is lower than that in del(5q). However, the trial demonstrated that a group of non-del(5q) MDS patients did respond to lenalidomide. Several studies were conducted to assess the efficacy of lenalidomide in non-del(5q) MDS. The reported hematological improvement in these studies, with patient samples that included lower-risk MDS of unselected or non-del(5q) karyotype, ranged from 26% to 64%, with a median duration of response of 12–20 months.Citation1
The largest study assessing the efficacy of lenalidomide in non-del(5q) MDS was conducted by Raza et al.Citation66 In this Phase II study, the efficacy of lenalidomide 10 mg daily for 21 of 28 days was assessed in 214 patients with low-risk or intermediate-1 risk non-del(5q) MDS who were RBC transfusion-dependent and receiving at least 2 units of RBC within 8 weeks of initiation of treatment. The overall response rate was 43%, with 26% of patients becoming RBC-TI. The median time to RBC-TI was 4.8 weeks. The median duration of RBC-TI was 41 weeks.Citation12,Citation66
Lenalidomide has not been approved by the US Food and Drug Administration for use in anemic patients with non-del(5q) MDS, although it is commonly used after failure of ESAs or for those with a high baseline serum erythropoietin level. Ongoing studies are trying to identify strategies that increase the response rate, such as using it in combination with other agents, in addition to trying to predict which non-del(5q) patients will have the best response.
Predictors and prognosticators beyond the del(5q) and IPSS
Within the del(5q) MDS patient population, clinical outcomes and response to lenalidomide have been negatively affected by certain baseline clinical characteristics, such as higher transfusion burden, anemia, lower platelet count, male sex, additional chromosomal abnormalities, and a higher percentage of BM blasts.Citation63 To date, no clinical or molecular factors have consistently predicted the response to lenalidomide in patients with del(5q) or identified subsets of non-del(5q) or high-risk del(5q) that benefit from lenalidomide. With improvements in the use of next- generation sequencing platforms, we are learning more about the abundance of these mutations in MDS. Ebert et al analyzed the pretreatment gene expression patterns in patients from MDS-002 (low-risk MDS patients without del(5q),Citation67 and identified a set of 47 genes that were more highly expressed in nonresponders than responders. These genes are specific to terminal erythroid differentiation. This gene signature correctly predicted the response to lenalidomide in 9/11 (82%) samples from low-risk patients without del(5q). This gene signature has yet to be validated in a larger series. A 29-gene expression profile signature has been reported to be a predictor of hematologic response in non-del(5q) lower-risk MDS patients treated with lenalidomide alone or combined with erythropoietin-beta.Citation68
In another study, ten (18%) of 55 patients having low-risk or intermediate-1 risk MDS with del(5q) were found to harbor TP53 mutations at diagnosis.Citation69 The rate of progression to AML was 50% in the mutated group compared with 16% in the nonmutated group, and the response rate was 0% in the mutated group compared with 50% in the nonmutated group.Citation69,Citation70 Mallo et al utilized conventional G-banding cytogenetics, single nucleotide polymorphism assays, and gene sequencing to identify additional molecular markers that could predict the response to lenalidomide in 52 patients with del(5q).Citation71 TP53 mutations were associated with an absence of a hematologic or complete cytogenetic response. Otherwise, this study did not show significant genomic differences between lenalidomide responders and nonresponders.Citation71 These data highlight the clinical significance of TP53 mutations in the treatment of patients with del(5q) and low-risk IPSS categorization. As discussed in the “Combination strategies” section patients with del(5q) MDS and mutated TP53 might benefit from combination or more aggressive treatment.
Other mutations occur in patients with del(5q). It has been reported that 40% of patients with 5q-syndrome harbor at least one gene mutation.Citation72 Elucidation of the clinical significance of these additional mutations requires further investigation. In addition to TP53, other biomarkers that may predict the response to lenalidomide were evaluated in several relatively small studies. Sugimoto et al explored the relationship between molecular features and the clinical response to lenalidomide in patients without del(5q).Citation73 This study demonstrated that normal karyotype and gain of chromosome 8 material were predictive of response to lenalidomide. Wu et al showed that lower RPS14 levels in low-risk MDS patients without del(5q) are a good prognostic marker and can potentially predict a good response to lenalidomide.Citation74 Specific cereblon polymorphisms have been associated with a hematological response to lenalidomide and may potentially serve as a predictive marker if well validated in future studies.Citation68,Citation75
As discussed, lenalidomide can activate T-cells by increasing CD28 activation. This may translate into increased antileukemic immunosurveillance.Citation52 Epling-Burnette et al demonstrated that a higher percentage of CD28-negative T-cells is associated with hematological failure of lenalidomide in non-del(5q) MDS.Citation52 Thus, CD28 expression and signaling may serve as a potential predictor of hematologic response to lenalidomide in non-del(5q) MDS.Citation52
Mechanisms of resistance
The phenotypic heterogeneity that characterizes del(5q) MDS is in part a reflection of additional genetic and karyotypic abnormalities beyond the 5q segment deletion that ultimately leads to a poorer response to lenalidomide. Beyond genetic and karyotypic abnormalities, resistance to lenalidomide is mediated by changes in several haplodeficient pathways leading to p53 accumulation, resulting in loss of erythropoietic response.Citation11 In vitro studies suggest that haploinsufficiency of CDC25C and PP2A in del(5q) confers sensitivity to lenalidomide, and its overexpression might confer resistance. Wei et al demonstrated that forced overexpression of PP2A in del(5q) cells promotes drug resistance.Citation44 This is potentially clinically relevant. Studying sequential BM specimens from lenalidomide-treated patients, cellular expression of PP2A declined at the time of response to lenalidomide treatment, and significantly increased at the time of treatment failure. Overexpression of PP2A restores p53 expression in erythropoietic cells and leads to treatment failure.Citation44
Given the central role of p53 in hypoplastic anemia, investigational strategies targeting p53 expression have been evaluated. The efficacy of cenersen, an antisense RNA that cleaves mRNA and effectively downregulates p53 expression, has been studied in overcoming resistance to lenalidomide. In vitro, cenersen suppressed p53 expression in del(5q) MDS. This was associated with a proportional increase in erythroid response without del(5q) clonal suppression.Citation11,Citation76 Further discussion about the clinical role and application of p53 suppression is discussed in more detail in the “Combination strategies” section.
In a small study that included seven patients who achieved transfusion independence on lenalidomide, Tehranchi et al demonstrated that lenalidomide was effective in eradicating the majority of del(5q) clones in responders.Citation77 However, in all seven patients, even those with a complete response, there was evidence of selective persistence of a CD34+, CD38−/low, and CD90+ resistant clone. This clone may persist in the BM because of its quiescent state (G0) and/or its high expression of multiple drug resistance genes. This resistant clone might explain why around 50% of responders relapsed despite lenalidomide treatment.Citation77 Validating these results in larger cohorts may allow for better monitoring and targeting of this resistant clone.
Combination strategies
Several strategies are under evaluation to increase the response to lenalidomide, broaden its usage beyond the current approved indications, and overcome resistance. Lenalidomide has been combined with growth factors, AML-like chemotherapy, azacitidine, and other new agents. Komrokji et al evaluated hematologic response rates to lenalidomide monotherapy and combined treatment with recombinant erythropoietin-alpha.Citation78 Thirty-nine low-risk or intermediate-1 risk patients with symptomatic anemia or transfusion dependence were enrolled in this Phase II trial. The majority were non-del(5q) patients (n=32). The patients were started on monotherapy with lenalidomide (10 or 15 mg daily). After 16 weeks of treatment with lenalidomide, nonresponders and relapsing patients were offered combination therapy with lenalidomide and recombinant erythropoietin-alpha. Adding erythropoietin increased the response rate in both del(5q) and non-del(5q) by a total of 25%. A Phase III trial is currently being conducted to validate these results.
Combination therapy was not associated with increased adverse events, including venous thromboembolism (VTE).Citation78 Another Phase II study supported the role of combination therapy.Citation68 In this study, transfusion-dependent, low risk non-del(5q) MDS patients resistant to ESA or relapsed were randomized to lenalidomide alone or lenalidomide plus erythropoietin-beta. The lenalidomide dose was 10 mg/day for 21/28 days and the erythropoietin-beta dose was 60,000 U/week. After four cycles of therapy, patients in the combination arm achieved better hematologic improvement, ie, 52.0% (26/50) versus 30.6% (14/49) in the lenalidomide group. RBC-TI was also higher in the combination arm, at 16 patients (32%) versus nine (18.4%) in the lenalidomide arm. Side effects were similar in the two arms, with no increase in deep vein thrombosis in the combination arm. The authors concluded that combination treatment significantly increased the erythroid response rate in lower-risk non-del(5q) MDS patients with anemia resistant to ESA alone.Citation68
Another Phase II study evaluated the safety and efficacy of combining romiplostim with lenalidomide to decrease the incidence of treatment-related thrombocytopenia in patients with low-risk or intermediate-1 risk MDS.Citation79 The authors reported that this combination decreased the rate of clinically significant thrombocytopenic events and in turn decreased the frequency of lenalidomide dose reductions or delays.Citation71 The main concern about using romiplostim in MDS is the increased risk of transformation to AML, especially in high-risk groups, as suggested by early Phase II trials.Citation79 Only results from large Phase III trials can adequately assess this risk, especially in patients with low-risk disease in whom lenalidomide is used for the most part at this time.Citation80
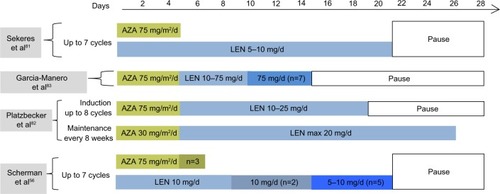
Several Phase I and II studies examined the efficacy and safety of combining azacitidine and lenalidomide.Citation81–Citation83 Lenalidomide and azacitidine could potentially have synergistic effects. Azacitidine can potentially increase the response rate in del(5q) patients with TP53 mutations, while lenalidomide can potentially increase the response rate in patients with complex karyotypes including del(5q).Citation84 A landmark Phase II trial by Sekeres et al explored the efficacy of a concurrent combination of lenalidomide and azacitidine.Citation81 The study included 36 patients, the majority (87%) of whom had intermediate-2 and high-risk IPSS disease, and only two patients had del(5q). The overall response rate was 72% and the complete response rate was 44%. The median time to response was 3.7 months and the median duration of response in patients with a complete response was 17+ months. This is compared with the overall response rate of 49% and the complete response rate of 17% with azacitidine alone. Median overall survival was 13.6 months. This is shorter than the median overall survival in the AZA-001 trial, which was 24.5 months.Citation85 This could be due to a shorter median follow-up (11.5 months versus 21.1 months). The median neutrophil and platelet decrease was 35% and 15%, respectively. Grade 3 and 4 nonhematologic toxicities were comparable with those seen with each medication individually.Citation81 This combination is the subject of an ongoing randomized Phase III US Intergroup study.
In a multicenter Phase I trial, 19 patients with higher-risk MDS/AML and del(5q) were enrolledCitation82 to receive a sequential combination regimen of lenalidomide and azacitidine. In partial responders, induction therapy was continued for up to eight cycles. Patients who achieved a complete BM response after two cycles of induction were shifted to maintenance therapy aiming at decreasing the hematologic toxicity. The overall response rate was 26% in all patients, and was 44% in previously untreated patients. The median duration of hematologic and cytogenetic response was 2.3 months and 3.2 months, respectively. These responses, although short-lived, were achieved in a study population rich in the p53 mutation (11/17). This sequential combination resulted in a TP53 mutant clone decline and disappearance in one patient, and in decline followed by re-emergence in another patient.Citation82 Re-emergence preceded relapse. Although the number is small, these effects on TP53 mutated clonal cells are significant since they have not been reported with lenalidomide alone.Citation82 The authors of this study attributed the lower overall response rate when compared with the overall response rate seen in the study reported by Sekeres et al to the higher percentage of complex karyotypes as well as the higher proportion of patients with TP53 mutations in their cohort.Citation81
summarizes the treatment scheme for some of the clinical trials using a combination of azacitidine and lenalidomide. The verdict is still out regarding the best regimen, ie, concurrent versus sequential, as well as the best maintenance strategy.Citation23,Citation86 So far, Phase I and Phase II studies suggest that combining azacitidine and lenalidomide is generally well tolerated, and can potentially lead to a better and faster overall response rate. However, it may be associated with more neutropenia and thrombocytopenia, and some of the responses were short-lived. Although the mechanisms of action for lenalidomide and azacitidine are different and can be synergistic, their cytoreductive potential is overlapping. Therefore, the search for compounds that act synergistically with lenalidomide without overlapping cytotoxic potential is ongoing.
Figure 3 Treatment scheme of Phase I and II clinical trials using combinations of azacitidine and lenalidomide in patients with myelodysplastic syndrome or acute myeloid leukemia.
Ezatiostat is potentially one of these compounds. Ezatiostat hydrochloride is a glutathione analog that can reversibly inhibit glutathione-S transferase P1-1, leading to activation of JNK and subsequent growth and maturation of hematopoietic progenitors.Citation87 It has shown in vivo and in vitro activity in improving cytopenias in MDS.Citation87 Its use with lenalidomide is very appealing because, unlike many of the other combinations, it does not have a myelosuppressive effect and the response rate to ezatiostat was higher in patients previously treated with lenalidomide.Citation87 Raza et al demonstrated the safety of combining ezatiostat 1,000 mg twice daily with lenalidomide 10 mg (21/28).Citation87 Efficacy data are encouraging since the combination showed multilineage hematologic improvements even in some patients who progressed on lenalidomide. The combination is now being evaluated in Phase II studies.Citation87
Given the role of p53 in the hypoplastic anemia of del(5q) MDS and its potential role in drug resistance, a p53-targeted strategy to overcome resistance was explored in a proof-of-principle pilot study by Caceres et al.Citation76 In this study, eight lenalidomide-resistant patients were treated with lenalidomide and dexamethasone. Dexamethasone was chosen because it is a transcriptional antagonist of p53. All patients had del(5q) MDS with an IPSS score of 1. Initially, all patients responded to lenalidomide by becoming transfusion-independent. However, all developed resistance and became transfusion-dependent again. A weekly dose of 20 mg of dexamethasone was combined with the usual dose of lenalidomide. Five patients achieved transfusion independence, with durations of response ranging from 4.4 months to 15 months.Citation76 p53-targeted strategies should employ treatment strategies that lead to nonsustained suppression of p53, such as weekly dexamethasone, since sustained suppression may significantly increase the risk of neoplasia.
Real-life use of lenalidomide for treatment of MDS
The “real-life” patterns of use and clinical efficacy of lenalidomide in management of MDS in the USA are not clear. Zeidan et al published the first report of lenalidomide use in a large cohort of Medicare-enrolled patients with MDS.Citation88 The authors identified 23,855 MDS patients enrolled in the Medicare program in the USA using International Classification of Diseases 9 codes between 2006 and 2008 and followed the patients until the end of the study or death. Claims-based data were used to determine MDS subtype, lenalidomide dose, time to initiation and duration of therapy, use of other MDS therapies, comorbidities, and RBC transfusion frequency. The researchers defined RBC transfusion status using weekly measures in a rolling 8-week period to classify patients into three separate categories based on their transfusion needs: those who received RBC transfusions in separate 2 weeks were classified as transfusion dependent, those who received one transfusion as transfusion users, and those who did not receive any transfusions as transfusion-independent.Citation88
In total, 753 MDS patients (3.2%) received lenalidomide. Interestingly, most of these patients did not have a coding diagnosis of del(5q) MDS, while only 31% of 470 patients who had a code for del(5q) MDS received the drug. Nonetheless, the percentage of patients with del(5q) MDS who were prescribed lenalidomide increased over time, probably indicating increasing familiarity and experience of physicians with the drug. The authors observed that, in contrast with the drug approval label, only 33% of patients were RBC transfusion-dependent at the time of initiation of therapy. Physicians initiated lenalidomide therapy more rapidly for patients with del(5q) MDS than for other lower-risk MDS patients (median time to initiation from diagnosis 8 weeks versus 20 weeks; P<0.01, respectively). The use of lenalidomide was negatively associated with increasing age and baseline comorbidities. The authors noted that overall, the reduction in transfusion rates were consistent with clinical trials data, ie, 44% of transfusion-using/transfusion-dependent patients achieved reductions in transfusion use. Responses were more frequent among transfusion-dependent patients who received three or more cycles of therapy (77% reduced their transfusion use and 40% became transfusion-independent). Response rates were higher when three or more lenalidomide cycles were received. Among patients with transfusion using/transfusion-dependent del(5q) MDS, 53% achieved reductions in their need for transfusion.Citation88
As previously mentioned, the data from MDS-004 suggest that lenalidomide is associated with improvement in quality of life among responders. However, data regarding cost-effectiveness from this trial are not available. Early data suggest that oral lenalidomide is cost-effective in the USA in the treatment of transfusion-dependent, low-risk, or intermediate-risk del(5q) MDS. Goss et al demonstrated that the cost of lenalidomide treatment was offset by reduced blood transfusion and erythropoietin costs.Citation89
Our approach and conclusion
Currently, the approved indication of lenalidomide in MDS is restricted to IPSS lower-risk MDS patients with del(5q) and symptomatic transfusion-dependent anemia. Although the dose of lenalidomide approved by the US Food and Drug Administration for del(5q) MDS is 10 mg daily, in clinical practice doses of 5–10 mg for 21–28 days of 28 days are usually used. If well tolerated, responders should continue treatment indefinitely.Citation1 Lower doses and/or an intermittent schedule might be used if toxicity occurs. Myelosuppression is the most common side effect of lenalidomide. Blood counts should be checked weekly for the first 8 weeks and then monthly thereafter. Adding granulocyte colony-stimulating factors can be considered once the neutrophil count is less than 1,000×106 cells/L.Citation90 We usually hold treatment until the neutrophil count is >500×106 cells/L. We also hold treatment if the platelet count is less than 50×109 cells/L and resume it once counts are above 50×109/L.Citation90 The reported incidence of VTE in lenalidomide-treated patients in the Groupe Francophone des Myélodysplasies, MDS-001, MDS-003, and MDS-004 studies is relatively low (3.4%).Citation45,Citation57,Citation58,Citation91 Prophylaxis for deep vein thrombosis is generally not recommended. However, VTE prophylaxis with low molecular weight heparin may be considered in patients with a prior VTE history.Citation1,Citation90 Evolving information suggests that testing for TP53 mutations should be incorporated into the prognostic score because of its potential impact on treatment choice in patients with del(5q) who are classified as low-risk to intermediate-risk based on current IPSS. Lenalidomide in non-del(5q) should be used for patients who are purely anemic; the National Comprehensive Cancer Network guidelines list lenalidomide as an option for treatment. The sequence of utilizing lenalidomide in lower risk non-del(5q) MDS may be of importance. For high-risk patients with del(5q), lenalidomide is not recommended outside the context of a clinical trial at this time. Potential use of lenalidomide in these patient populations includes using higher doses of the drug as well as combining lenalidomide with other medications, such as hypomethylating agents.Citation92 Future directions include finding biological markers to help in predicting responders in this population.
Acknowledgments
AMZ is supported by a Young Investigator Award from the American Society of Clinical Oncology (ASCO YIA) and by an Evans Fellow award from the MDS Clinical Research Consortium of the Aplastic Anemia and Myelodysplastic Syndromes International Foundation (AAMDSIF) and the Ed Evans Foundation.
Disclosure
The authors report no conflicts of interest in this work.
References
- LeitchHABucksteinBShamyAStorringJMThe immunomodulatory agents lenalidomide and thalidomide for treatment of the myelodysplastic syndromes: a clinical practice guidelineCrit Rev Oncol Hematol201385216219222901762
- MitchellMGoreSDZeidanAMIron chelation therapy in myelodysplastic syndromes: where do we stand?Expert Rev Hematol20136439741023991926
- HuangTCKoBSTangJLComparison of hypoplastic myelodysplastic syndrome (MDS) with normo-/hypercellular MDS by International Prognostic Scoring System, cytogenetic and genetic studiesLeukemia200822354455018094713
- MalcovatiLHellström-LindbergEBowenDDiagnosis and treatment of primary myelodysplastic syndromes in adults: recommendations from the European LeukemiaNetBlood2013122172943296423980065
- RådlundAThiedeTHansenSCarlssonMEngquistLIncidence of myelodysplastic syndromes in a Swedish populationEur J Haematol19955431531567720834
- AulCGiagounidisAGermingUEpidemiological features of myelodysplastic syndromes: results from regional cancer surveys and hospital-based statisticsInt J Hematol200173440541011503953
- GermingUStruppCKündgenANo increase in age-specific incidence of myelodysplastic syndromesHaematologica200489890591015339672
- RollisonDEHowladerNSmithMTEpidemiology of myelodysplastic syndromes and chronic myeloproliferative disorders in the United States, 2001–2004, using datat from the NAACCR and SEER programsBlood20081121455218443215
- NeukirchenJSchoonenWMStruppCIncidence and prevalence of myelodysplastic syndromes: data from the Düsseldorf MDS-registryLeuk Res201135121591159621708407
- ZeidanAMFaltasBDouglas SmithBGoreSMyelodysplastic syndromes: what do hospitalists need to know?J Hosp Med20138635135723666619
- ZeidanAMSmithBDKomrokjiRSGoreSDPrognostication in myelodysplastic syndromes: beyond the International Prognostic Scoring System (IPSS)Am J Med20131264e2523507216
- FaltasBZeidanAMGergisUMyelodysplastic syndromes: toward a risk-adapted treatment approachExpert Rev Hematol20136561162424094045
- ZeidanAMKomrokjiRSThere’s risk, and then there’s RISK: The latest clinical prognostic risk stratification models in myelodysplastic syndromesCurr Hematol Malig Rep20138435136023979829
- BennettJMCatovskyDDanielMTProposals for the classification of the myelodysplastic syndromesBr J Haematol19825121891996952920
- VardimanJWThieleJArberDAThe 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changesBlood2009114593795119357394
- GreenbergPCoxCLeBeauMMInternational scoring system for evaluating prognosis in myelodysplastic syndromesBlood1997896207920889058730
- MalcovatiLGermingUKuendgenATime-dependent prognostic scoring system for predicting survival and leukemic evolution in myelodysplastic syndromesJ Clin Oncol200725233503351017687155
- GreenbergPLTuechlerHSchanzJRevised international prognostic scoring system for myelodysplastic syndromesBlood2012120122454246522740453
- BennettJMCatovskyDDanielMTProposals for the classification of the acute leukaemias. French-American-British (FAB) co-operative groupBr J Haematol1976334451458188440
- KantarjianHO’BrienSRavandiFProposal for a new risk model in myelodysplastic syndrome that accounts for events not considered in the original International Prognostic Scoring SystemCancer200811361351136118618511
- EisenmannKMDykemaKJMathesonSF5q-myelodysplastic syndromes: chromosome 5q genes direct a tumor-suppression network sensing actin dynamicsOncogene200928393429344119597464
- VoutsadakisIACairoliAA crtitical review of the molecular pathophysiology of lenalidomide sensitivity in 5q-myelodysplastic syndromesLeuk Lymphoma201253577978821955212
- ZeidanAMGoreSDKomrokjiRSHigher-risk myelodysplastic syndromes with del(5q): is sequential azacitidine-lenalidomide combination the way to go?Expert Rev Hematol20136325125423782079
- FaltasBZeidanAGergisUMyelodysplastic syndromes: toward a risk-adapted treatment approachExpert Rev Hematol20136561162424094045
- BoultwoodJLewisSWainscoatJSThe 5q-syndromeBlood19948410325332607949083
- BoultwoodJPellagattiAMcKenzieANJWainscoatJSAdvances in the 5q-syndromeBlood2010116265803581120733155
- van LeeuwenBHMartinsonMEWebbGCYoungIGMolecular organization of the cytokine gene cluster, involving the human IL-3, IL-4, IL-5, and GM-CSF genes, on human chromosome 5Blood1989735114211482564789
- RobertsWMLookATRousselMFSherrCJTandem linkage of human CSF-1 receptor (c-fms) and PDGF receptor genesCell19885546556612846185
- Van den BergheHCassimanJJDavidGFrynsJPMichauxJLSokalGDistinct haematological disorder with deletion of long arm of no 5 chromosomeNature197425154744374384421285
- EbertBLDeletion 5q in myelodysplastic syndrome: a paradigm for the study of hemizygous deletions in cancerLeukemia20092371252125619322210
- KomrokjiRSPadronEEbertBLListAFDeletion 5q MDS: molecular and therapeutic implicationsBest Pract Res Clin Haematol201326436537524507813
- GiagounidisAMuftiGJFenauxPGermingUListAMacBethKJLenalidomide as a disease-modifying agent in patients with del(5q) myelodysplastic syndromes: linking mechanism of action to clinical outcomesAnn Hematol201493111124018623
- EbertBLPretzJBoscoJIdentification of RPS14 as a 5q-syndrome gene by RNA interference screenNature2008451717633533918202658
- NarlaAHurstSNEbertBLRibosome defects in disorders of erythropoiesisInt J Hematol201193214414921279816
- ShiDGuWDual roles of MDM2 in the regulation of p53: ubiquitination dependent and ubiquitination independent mechanisms of MDM2 repression of p53 activityGenes Cancer201233–424024823150757
- StarczynowskiDTKuchenbauerFArgiropoulosBIdentification of miR-145 and miR-146a as mediators of the 5q-syndrome phenotypeNat Med2010161495819898489
- StarczynowskiDTKarsanADeregulation of innate immune signaling in myelodysplastic syndromes is associated with deletion of chromosome arm 5qCell Cycle20109585585620160505
- LehmannSO’KellyJRaynaudSFunkSESageEHKoefflerHPCommon deleted genes in the 5q-syndrome: thrombocytopenia and reduced erythroid colony formation in SPARC null miceLeukemia20072191931193617625608
- AdèsLFenauxPImmunomodulating drugs in myelodysplastic syndromesHematology Am Soc Hematol Educ Program2011201155656022160089
- KelaidiCParkSBrechignacSTreatment of myelodysplastic syndromes with 5q deletion before the lenalidomide era; the GFM experience with EPO and thalidomideLeuk Res20083271049105318191202
- RazaAMeyerPDuttDThalidomide produces transfusion independence in long-standing refractory anemias of patients with myelodysplastic syndromesBlood200198495896511493439
- Moreno-AspitiaAColon-OteroGHoeringAThalidomide therapy in adult patients with myelodysplastic syndrome. A North Central Cancer Treatment Group Phase II trialCancer2006107476777216826578
- StruppCHildebrandtBGermingUHaasRGattermannNCytogenetic response to thalidomide treatment in three patients with myelodysplastic syndromeLeukemia20031761200120212764395
- WeiSChenXMcGrawKLenalidomide promotes p53 degradation by inhibiting MDM2 auto-ubiquitination in myelodysplastic syndrome with chromosome 5q deletionOncogene20133291110112022525275
- ListADewaldGBennettJLenalidomide in the myelodysplastic syndrome with chromosome 5q deletionN Engl J Med2006355141456146517021321
- NarlaADuttSMcAuleyJRDexamethasone and lenalidomide have distinct functional effects on erythropoiesisBlood201111882296230421527522
- ListAFEstesMWilliamsALenalidomide (CC-5013; Revlimid) promotes erythropoiesis in myelodysplastic syndromes (MDS) by CD45 protein tyrosine phosphatase (PTP) inhibitionASH Annual Meeting Abstracts20061081360
- KomrokjiRSListAFRole of lenalidomide in the treatment of myelodysplastic syndromesSemin Oncol201138564865721943671
- CorralLGHaslettPAMullerGWDifferential cytokine modulation and T cell activation by two distinct classes of thalidomide analogues that are potent inhibitors of TNT-alphaJ Immunol1999163138038610384139
- SymeonidisAKourakliAKatevasPImmune function parameters at diagnosis in patients with myelodysplastic syndromes: correlation with the FAB classification and prognosisEur J Haematol19914742772811954986
- KotlaVGoelSNischalSMechanism of action of lenalidomide in hematological malignanciesJ Hematol Oncol200923619674465
- Epling-BurnettePKHanYMaillouxAWNovel predictor of lenalidomide response in non-del5q MDS reveals linkage to molecular mechanism: first characterization of T-cell function in cereblon homozygous deficient mice55th ASH Annual Meeting and Exposition2013 Available from: https://ash.confex.com/ash/2013/webprogram/Paper65378.htmlAccessed August 28, 2014
- GuptaDTreonSPShimaYAdherence of multiple myeloma cells to bone marrow stromal cells upregulates vascular endothelial growth factor secretion: therapeutic applicationsLeukemia200115121950196111753617
- TeoSKProperties of thalidomide and its analogues: implications for anticancer therapyAAPS J200571E14E1916146335
- GiagounidisAAGermingUHaaseSClinical, morphological, cytogenetic, and prognostic features of patients with myelodysplastic syndromes and del(5q) including band q31Leukemia200418111311914586479
- SchermanEMalakSPerotCGorinNCRubioMTIsnardFInterest of the association azacitidine-lenalidomide as frontline therapy in high-risk myelodysplasia or acute myeloid leukemia with complex karyotypeLeukemia201226482282421997572
- ListAKurtinSRoeDJEfficacy of lenalidomide in myelodysplastic syndromesN Engl J Med2005352654955715703420
- FenauxPGiagounidisASelleslagDA randomized phase 3 study of lenalidomide versus placebo in RBC transfusion-dependent patients with low-/intermediate-1-risk myelodysplastic syndromes with del5qBlood2011118143765377621753188
- ListAFBennettJMSekeresMAExtended survival and reduced risk of AML progression in erythroid-responsive lenalidomide-treated patients with lower-risk del(5q) MDSLeukemia20142851033104024150217
- OlivaENLatagliataRMorabitoFLenalidomide for the treatment of low- and int-1-risk MDS with del(5q): efficacy and quality of life studyBlood200911421080
- GöhringGGiagounidisABüscheGPatients with del(5q) MDS who fail to achieve sustained erythroid or cytogenetic remission after treatment with lenalidomide have an increased risk for clonal evolution and AML progressionAnn Hematol201089436537419855965
- AdèsLLe BrasFSebertMTreatment with lenalidomide does not appear to increase the risk of progression in lower risk myelodysplastic syndromes with 5q deletion. A comparative analysis by the Groupe Francophone des MyelodysplasiesHaematologica201297221321821993675
- KuendgenALausekerMListAFLenalidomide does not increase AML progression risk in RBC transfusion-dependent patients with low- or intermediate-1-risk MDS with del(5q): a comparative analysisLeukemia20132751072107923257782
- AdèsLBoehrerSPrebetTEfficacy and safety of lenalidomide in intermediate-2 or high-risk myelodysplastic syndromes with 5q deletion: results of a phase 2 studyBlood2009113173947395218987358
- MöllgårdLSaftLTreppendahlMBClinical effect of increasing doses of lenalidomide in high-risk myelodysplastic syndrome and acute myeloid leukemia with chromosome 5 abnormalitiesHaematologica201196796397121719884
- RazaAReevesJAFeldmanEJPhase 2 study of lenalidomide in transfusion-dependent, low-risk, and intermediate-1 risk myelodysplastic syndromes with karyotypes other than deletion 5qBlood20081111869317893227
- EbertBLGaliliNTamayoPAn erythroid differentiation signature predicts response to lenalidomide in myelodysplastic syndromePLoS One200852e35
- TomaAA randomized study of lenalidomide (LEN) with or without EPO in RBC transfusion dependent (TD) IPSS low and int-1 (lower risk) myelodysplastic syndromes (MDS) without del 5q resistant to EPOJ Clin Oncol201331Suppl 15 Abstr 7002
- JäderstenMSaftLSmithATP53 mutations in low-risk myelodysplastic syndromes with del(5q) predict disease progressionJ Clin Oncol201129151971197921519010
- GiagounidisAALenalidomide for del(5q) and non-del(5q) myelodysplastic syndromesSemin Hematol201249431232223079061
- MalloMDel ReyMIbáñezMResponse to lenalidomide in myelodysplastic syndromes with del(5q): influence of cytogenetics and mutationsBr J Haematol20131621748623614682
- Fernandez-MercadoMBurnsAPellagattiATargeted re-sequencing analysis of 25 genes commonly mutated in myeloid disorders in del(5q) myelodysplastic syndromesHaematologica201398121856186423831921
- SugimotoYSekeresMAMakishimaHCytogenetic and molecular predictors of response in patients with myeloid malignancies without del[5q] treated with lenalidomideJ Hematol Oncol20125422390313
- WuLLiXXuFZhangZChangCHeQLow RPS14 expression in MDS without 5q – aberration confers higher apoptosis rate of nucleated erythrocytes and predicts prolonged survival and possible response to lenalidomide in lower risk non-5q-patientsEur J Haematol201390648649323506134
- SardnalVRouquetteAKaltenbachSA G polymorphism in the CRBN gene acts as a biomarker of response to treatment with lenalidomide in low/int-1 risk MDS without del(5q)Leukemia20132771610161323434730
- CaceresGMcGrawKYipBHTP53 suppression promotes erythropoiesis in del(5q) MDS, suggesting a targeted therapeutic strategy in lenalidomide-resistant patientsProc Natl Acad Sci U S A201311040161271613224043769
- TehranchiRWollPSAndersonKPersistent malignant stem cells in del(5q) myelodysplasia in remissionN Engl J Med2010363111025103720825315
- KomrokjiRSLancetJESwernASCombined treatment with lenalidomide and epoetin alfa in lower-risk patients with myelodysplastic syndromeBlood2012120173419342422936658
- WangESLyonsRMLarsonRAA randomized, double-blind, placebo-controlled phase 2 study evaluating the efficacy and safety of romiplostim treatment of patients with low or intermediate-1 risk myelodysplastic syndrome receiving lenalidomideJ Hematol Oncol201257123190430
- WörmannBClinical indications for thrombopoietin and thrombopoietin-receptor agonistsTransfus Med Hemother201340531932524273485
- SekeresMATiuRVKomrokjiRPhase 2 study of the lenalidomide and azacitidine combination in patients with higher-risk myelodysplastic syndromesBlood2012120254945495122915641
- PlatzbeckerUBraulkeFKündgenASequential combination of azacitidine and lenalidomide in del(5q) higher-risk myelodysplastic syndromes or acute myeloid leukemia: a phase I studyLeukemia20132761403140723354011
- Garcia-ManeroGDaverNGBorthakurGPhase I study of the combination of 5-azacitidine sequentially with high-dose lenalidomide in higher-risk myelodysplastic syndrome (MDS) and acute myelogenous leukemia (AML)Blood20111181122
- PlatzbeckerUGermingUCombination of azacitidine and lenalidomide in myelodysplastic syndromes or acute myeloid leukemia – a wise liaison?Leukemia20132791813181923644421
- FenauxPMuftiGJHellstrom-LindbergEEfficacy of azacitidine compared with that of conventional care regimens in the treatment of higher-risk myelodysplastic syndromes: a randomised, open-label, phase III studyLancet Oncol200910322323219230772
- ZeidanAMLinharesYGoreSDCurrent therapy of myelodysplastic syndromesBlood Rev201327524325923954262
- RazaAGaliliNMulfordDPhase 1 dose-ranging study of ezatiostat hydrochloride in combination with lenalidomide in patients with non-deletion (5q) low to intermediate-1 risk myelodysplastic syndrome (MDS)J Hematol Oncol201251822546242
- ZeidanAMGoreSDMcNallyDLLenalidomide performance in the real world: patterns of use and effectiveness in a Medicare population with myelodysplastic syndromesCancer2013119213870387823922173
- GossTFSzendeASchaeferCCost effectiveness of lenalidomide in the treatment of transfusion-dependent myelodysplastic syndromes in the United StatesCancer Control200613Suppl172517242663
- DuongVHKomrokjiRSListAFEfficacy and safety of lenalidomide in patients with myelodysplastic syndrome with chromosome 5q deletionTher Adv Hematol20123210511623556117
- Le BrasFSebertMKelaidiCTreatment by Lenalidomide in lower risk myelodysplastic syndrome with 5q deletion – the GFM experienceLeuk Res201135111444144821715006
- ZeidanAMKharfan-DabajaMAKomrokjiRSBeyond hypomethylating agents failure in patients with myelodysplastic syndromesCurr Opin Hematol201421212313024335709
- BarlowJLDrynanLFHewettDRA p53-dependent mechanism underlies macrocytic anemia in a mouse model of human 5q-syndromeNat Med2010161596619966810
- WeiSChenXRochaKA critical role for phosphatase haplodeficiency in the selective suppression of deletion 5q MDS by lenalidomideProc Natl Acad Sci U S A200910631129741297919470455
- DeWardADLealiKWestRAPrendergastGCAlbertsASLoss of RhoB expression enhances the myelodysplastic phenotype of mammalian diaphanous-related Formin mDia1 knockout micePLoS One200949e710219768111