
Abstract
Transfusional iron overload is a major target in the care of patients with transfusion-dependent thalassemia (TDT) and other refractory anemias. Iron accumulates in the liver, heart, and endocrine organs leading to a wide array of complications. In this review, we summarize the characteristics of the approved iron chelators, deferoxamine, deferiprone, and deferasirox, and the evidence behind the use of each, as monotherapy or as part of combination therapy. We also review the different guidelines on iron chelation in TDT. This review also discusses future prospects and directions in the treatment of transfusional iron overload in TDT whether through innovation in chelation or other therapies, such as novel agents that improve transfusion dependence.
Introduction
The transfusion of packed red blood cells (pRBCs) is the cornerstone of treatment of many refractory anemias, whether congenital or acquired. These anemias include transfusion-dependent thalassemia (TDT), sickle-cell anemia, acquired red cell aplasia, Diamond–Blackfan anemia, myelodysplastic syndromes (MDS), myelofibrosis, and aplastic anemia. Patients with transfusional iron overload usually require iron chelation therapy (ICT) to help decrease the iron burden and to prevent and/or delay long-term complications associated with iron deposition in tissues. The burden of transfusional iron overload is associated with the frequency, volume, and duration of blood transfusion therapy. The complications resulting from untreated transfusional iron overload include hepatic dysfunction and failure, endocrinopathies, and cardiac dysfunction.
The theoretical necessity of iron chelation is based on the fact that iron absorption and excretion are balanced at about 1 mg/day, commensurate with body iron requirements.Citation1 Iron is used by erythrocytes for heme synthesis and by other body cells to meet metabolic needs. Excess iron is stored in hepatocytes and macrophages within a dynamic cycle of iron utilization and recycling.Citation1 Macrophages play a central role in iron recycling by engulfing senescent erythrocytes and releasing heme-derived iron into the plasma.Citation2 However, the body does not have any mechanism to excrete excess transfusional iron that, for example, amounts up to 0.3–0.6 mg/kg/day in TDT, assuming a transfusion rate of 2–4 units per month with 200–250 mg of iron per unit.Citation3
In this review, we discuss: 1) the diagnosis and assessment of transfusional iron overload in TDT; 2) the available treatment modalities, whether monotherapy or combination therapy; and 3) how treatment is initiated and subsequently modified with patient follow-up. The review also includes an overview of 4) future directions in treating transfusional iron overload in TDT.
The efficacy and pharmacological profile of the three approved iron chelators, deferoxamine (DFO), deferiprone (DFP), and deferasirox (DFX), are discussed. The characteristics of DFO, DFP, and DFX are summarized in . It is noteworthy that most of the data concerning the management of transfusional iron overload emanate from the thalassemia population with extrapolation to other diseases, although differences do exist.
Table 1 Characteristics of iron chelators in clinical use
Overview of the pathophysiology of iron overload
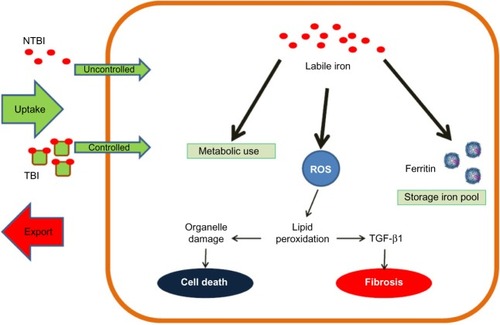
When red blood cells senesce, transfused red cells are phagocytized by reticuloendothelial macrophages where the hemoglobin is digested and the iron is freed from the heme. With a continuous increase in the iron load because of frequent transfusions, the excess iron in the cytosol of the macrophages starts spilling out into the plasma where transferrin binds the released iron.Citation4 However, as transferrin is increasingly saturated with iron, iron storage in hepatocytes starts. As the storage capacity of the hepatocytes and the macrophages gets saturated, circulating iron surmounts the binding capacity of transferrin. Therefore, non-transferrin-bound-iron (NTBI) starts circulating in the plasma and is deposited in cardiac myocytes, hepatocytes, pituitary cells, and pancreatic cells.Citation5 Reactive oxygen species produced by the metabolism of NTBI play a central role in inducing cellular dysfunction, apoptosis, and necrosis.Citation5 summarizes the interaction between the storage iron pool and the functional iron pool. depicts the role of NTBI in transfusional iron overload.
Figure 1 After absorption of iron into the enterocyte at the level of the duodenum, ferroportin transports iron into the circulation.
Abbreviation: NTBI, non-transferrin-bound-iron.
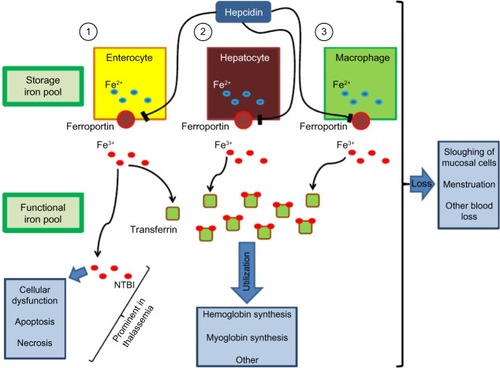
Figure 2 The excessive uncontrolled uptake of labile iron (NTBI) leads to iron overload in hepatocytes and cardiac myocytes.
Abbreviations: NTBI, non-transferrin-bound-iron; ROS, reactive oxygen species; TBI, transferrin-bound-iron; TGF-β1, transforming growth factor beta 1.
Iron distribution is modulated by the synthesis of hepcidin, a hepatic peptide, whereby increased hepcidin synthesis decreases iron release from enterocytes, hepatocytes, and macrophages through binding to ferroportin, the iron exporter, and causing its internalization.Citation6,Citation7 Even though ineffective erythropoiesis is significantly improved by transfusions in TDT, hepcidin suppression might contribute to iron overload, especially later in the transfusion-to-transfusion intervals. It has been suggested that the production of growth differentiation factor 15 (GDF15) and possibly other proteins, such as twisted-gastrulation 1 (TWSG1), contributes to the inhibition of hepcidin synthesis and thus promotes iron absorption despite systemic iron overload.Citation8,Citation9 Nevertheless, more recent studies argue against the role of GDF15 in hepcidin suppression.Citation10,Citation11 Kautz et al suggested that, upon erythropoietic stimulation, bone marrow and spleen erythroblasts increasingly produce erythroferrone, which, upon secretion into the circulation, directly acts on the liver to inhibit hepcidin production.Citation12
Overview of the iron chelating agents in use: characteristics and evidence
Deferoxamine
DFO is a hexadentate iron chelator that binds iron in 1:1 complexes. DFO cannot be orally absorbed; therefore, it is administered at a dose of 20–50 mg/kg/day, subcutaneously or intravenously.Citation13 Higher doses up to 60 mg/kg/day have been used in patients with high body iron stores. Having a short plasma half-life of 20–30 minutes, DFO should be administered over a span of 8–10 hours a day, on 5–7 days a week. Given the pharmacokinetics of DFO, it does not provide 24-hour-long chelation of NTBI.Citation14 DFO is excreted through biliary secretions and the urine. It is approved in the US, Canada, Europe, and other countries for transfusional iron overload. Only one randomized trial has compared chelation in 20 children with TDT with no therapy (10 were treated with DFO and 10 received no therapy).Citation15 After a mean of 5.8 years of follow-up, the patients treated with DFO intramuscularly had a mean liver iron concentration (LIC) of 25.9 mg/g dry weight (dw) of liver tissue as compared to 42.2 mg/g dw in the control group. In 1982, Modell et al suggested a survival benefit for thalassemia patients treated with 4 g or more of DFO weekly as, at 14 years, six deaths occurred in the control group compared to only one death in the treatment group.Citation16 A large observational study at seven Italian centers, involving 977 patients with TDT, also suggested a survival benefit for DFO.Citation17 The survival rate was found to be progressively increasing for every 5-year birth cohort since 1975, the year of introduction of DFO.Citation17 Moreover, Brittenham et al followed 59 patients with TDT, treated with DFO, for 4–10 years or until death.Citation18 Using a natural logarithm of the ratio of transfusional iron load to DFO use, they suggested that early chelation with DFO in an amount proportional to the transfusional iron load decreases hepatic iron concentration and helps safeguard against diabetes mellitus, cardiac disease, and earlier death in patients with TDT. The cardiac benefits of DFO in the context of transfusional iron overload were highlighted by Anderson et al and Davis and Porter, who showed, respectively, that higher doses of DFO up to 60 mg/kg/day can reduce cardiac iron load and reverse cardiac complications.Citation19,Citation20 The side effects of DFO include irritation at the infusion site, growth retardation, skeletal changes, and ocular and auditory disturbances.Citation13,Citation21,Citation22 Symptoms of cutaneous irritation at the site of the infusion respond to local anesthetic or glucocorticoid creams. Respiratory distress syndrome has been also reported with very high intravenous doses in the context of acute iron intoxication.Citation13,Citation22 Patients treated with DFO should be followed up with yearly assessments of vision and auditory function. Pediatric patients treated with DFO should be monitored for growth delay by assessing body weight and growth every 3 months.Citation13 Finally, limited compliance with DFO, due to the inconvenience of parenteral administration and its infectious complications, may lead to decreased efficacy in terms of iron chelation and progression of the manifestations of transfusional iron overload.Citation23,Citation24
Deferiprone
DFP, the first oral iron chelator to be used, is approved in Europe and other countries for transfusional iron overload in patients with TDT, when DFO therapy is contraindicated or inadequate.Citation25 In the US, since October 2011, DFP is indicated for the treatment of adults with transfusional iron overload due to thalassemic disorders when chelation therapy with DFX or DFO is inadequate.Citation26 DFP is a bidentate iron chelator that forms 3:1 complexes, usually given at a dose of 75–100 mg/kg/day divided over three doses.Citation25 The lipophilicity of DFP enables this small molecule to gain access into myocytes. As previously mentioned, DFO therapy has been associated with improved survival of thalassemia patients, but cardiac complications remained the major cause of mortality. From this stemmed the interest in the possible benefits of DFP in reversing or preventing cardiac complications. Borgna-Pignatti et al observed that DFP therapy was associated with significantly greater cardiac protection than DFO in thalassemic patients.Citation27 Moreover, a retrospective study by Piga et al showed, through Kaplan–Meier analysis, that 5-year cardiac disease-free survival was significantly more favorable in thalassemic patients treated with DFP as compared to those treated with DFO.Citation28 A meta-analytic review of nine clinical trials showed that 75.5% of highly iron-overloaded patients, treated with DFP for at least 16 months at doses of 75 mg/kg/day or higher, had a decrease in serum ferritin (SF) by an average of 23.5% from baseline.Citation29 A 1-year randomized controlled trial involving 144 patients with TDT suggested that DFP (75 mg/kg/day) is as effective as DFO in the treatment of iron overload in TDT.Citation30 Furthermore, higher doses of 100 mg/kg/day were shown to be safe and efficacious in decreasing SF over 2 years in 12 patients with TDT.Citation31 Compared to treatment with DFO, treatment with DFP was observed to be associated with lower myocardial iron deposition and higher left ventricular ejection fractions in a retrospective study by Anderson et al.Citation32 More robust prospective data from a randomized controlled trial of DFP versus DFO in 61 TDT patients with asymptomatic myocardial siderosis confirmed that, after 1 year of follow-up, the improvement in myocardial T2*, a method to quantitate cardiac iron load by MRI, was significantly greater in the DFP group.Citation33 A retrospective study by Berdoukas et al also confirmed that monotherapy with DFP is effective in reducing cardiac siderosis.Citation34 A retrospective study of a UK database of TDT patients suggested that DFP use is associated with a reduction in the risk of heart failure in patients with a baseline ejection fraction of 56–62% and in those with a normal ejection fraction of 63–70%.Citation35 Data from a large randomized controlled trial of 265 patients with TDT showed that DFP-containing regimens (DFP monotherapy, alternating DFO + DFP therapy, and combination therapy with DFO + DFP) were associated with a lower mortality when compared with DFO monotherapy.Citation36 From a clinical standpoint, patients on DFP should be closely monitored as it may cause agranulocytosis and neutropenia necessitating weekly follow-up with complete blood count.Citation25,Citation37 DFP may also cause gastrointestinal disturbances, arthropathy, increased liver-enzyme levels, low plasma zinc level, and progression of hepatic fibrosis associated with increase in iron overload or hepatitis C.Citation25,Citation38 However, more recent studies have shown a lack of progression of liver fibrosis with DFP therapy.Citation30,Citation39–Citation41
Deferasirox
DFX, a tridentate iron chelator that forms 2:1 complexes, is another oral agent with a once-daily dosing at a usual dose of 20–40 mg/kg/day.Citation42 The plasma half-life of DFX is 16–18 hours, and it is predominantly excreted in biliary secretions. Just as DFO, it is approved in the US, Canada, Europe, and other countries for transfusional iron overload.Citation42 In the context of DFP’s potentially life-threatening side effect of agranulocytosis and its short half-life, DFX was developed out of a need for a long-acting chelator with a convenient dosing regimen for patients with transfusional iron overload.Citation43 DFX should be taken on an empty stomach after dissolution in water, apple juice, or orange juice to assure adequate bioavailability.Citation43,Citation44 A Phase II trial randomized patients to DFX at 10 mg/kg/day or DFX at 20 mg/kg/day or DFO 40 mg/kg/day.Citation45 It concluded that DFX was well tolerated and showed similar efficacy to DFO 40 mg/kg in terms of reducing LIC when used at 20 mg/kg/day. Moreover, Galanello et al evaluated the safety, tolerability, and pharmacokinetics of DFX in children 2 years or older.Citation46 The study showed that DFX 10 mg/kg/day is well tolerated but does not induce a negative iron balance. Up to this date, the largest trial comparing DFX with DFO (study 0107, a Phase III trial) included 296 patients assigned to DFX and 290 patients assigned to DFO.Citation47 The failure of this trial to prove non-inferiority was attributed to the underdosing of DFX. A total of 52.9% of the patients assigned to DFX had either a maintained or a reduced LIC at 1 year, while 66.4% of the patients in the DFO arm reached the primary endpoint. However, this trial, which included both pediatric and adult patients, suggested that DFX doses of 30 mg/kg led to negative iron balance and decreased SF levels along with a significant decrease in LIC. Another Phase II trial, including 184 patients with Diamond–Blackfan anemia, MDS, β-thalassemia, or other rare anemias, showed that DFX is effective for reducing iron burden in patients with various transfusion-dependent anemias.Citation48 LIC changes were overall dependent on DFX dose and transfusional iron intake. There were no statistically significant differences in LIC changes between different disease groups. The ESCALATOR study, a prospective, open-label study performed in the Middle East on patients with β-thalassemia, previously treated with DFP and/or DFO, showed that appropriate dosing of DFX controlled iron levels in population of patients with heavy iron load.Citation49 A retrospective pooled analysis of patients with TDT and other transfusion-dependent diseases concluded that DFX therapy at doses greater than 30 mg/kg/day effectively reduced SF to levels lower than those prior to dose escalation with no safety concern.Citation50 Looking further into the effect of DFX on the liver, Deugnier et al showed that DFX therapy for at least 3 years reversed or stabilized liver fibrosis in TDT patients with transfusional iron overload – an effect independent of exposure to hepatitis C virus and of reduction in LIC.Citation51 The prospective 1-year EPIC study, including patients with transfusional iron overload secondary to thalassemia, MDS, aplastic anemia, sickle-cell disease, and other conditions, supported initial DFX doses based on transfusional iron intake with subsequent dose titration guided by SF and safety markers.Citation52 The recommended initial dose was 20 mg/kg/day for patients receiving 2–4 pRBC units per month. DFX at a dose of 10 mg/kg/day or 30 mg/kg/day was recommended for patients receiving, respectively, less or more frequent transfusions.Citation52 A substudy of the EPIC trial showed that DFX doses of 20 mg/kg/day safely maintained LIC <7 mg Fe/g dw.Citation53 Doses of 30 mg/kg/day were required for net iron reduction in patients with LIC ≥7 mg Fe/g dw. An extension of the EPIC cardiac substudy, which recruited 71 patients, concluded that 3 years of DFX treatment significantly decreased cardiac iron overload, as compared to baseline, and normalized T2* in 68.1% of patients with T2* between 10 ms and <20 ms.Citation54 More recently, data from the CORDELIA study showed the non-inferiority of DFX compared with DFO for myocardial iron removal in 197 TDT patients with myocardial siderosis but no signs of cardiac dysfunction.Citation55 The most common adverse events with DFX therapy include gastrointestinal disturbances, rash, and mild increases in serum creatinine.Citation34,Citation42 DFX therapy is not commonly associated with agranulocytosis and growth failure.Citation47 DFX may be rarely associated with renal impairment, hepatic impairment, and gastrointestinal hemorrhage.Citation42
Combining iron chelators
Combination and alternating therapy with DFO and DFP
Combination therapy with DFO and DFP was introduced as a means to manage iron overload in patients suboptimally chelated with maximum doses of DFP.Citation56 The synergistic effect of DFP and DFO on iron balance and urine iron excretion has been explained by the shuttle mechanism. DFP enters cells and removes iron, and then passes it on to DFO for excretion in urine or feces.Citation57–Citation59 Subsequently, DFP becomes free again to enter the cell and remove more iron. In the treatment of cardiac iron overload, evidence from well-conducted randomized controlled trials shows superior efficacy of DFP versus DFO, the superiority of combined DFP + DFO versus DFO alone, and the equivalence of DFX versus DFO.Citation60
Earlier studies suggested a potential role for combination therapy with DFO and DFP showing that DFO + DFP is as effective as DFO in reducing iron load in both the adult and pediatric populations.Citation61–Citation63 This is especially important from the standpoint of compliance with treatment. Aydinok et al compared daily monotherapy with DFP (75 mg/kg/day), monotherapy with DFO (40–50 mg/kg/day for 5 days per week), and combination therapy with DFP (75 mg/kg/day for 7 days per week) + DFO (40–50 mg/kg/day for 2 days per week).Citation64 The patients treated with DFP + DFO showed the highest total iron excretion and iron balance with results reaching statistical significance against DFP monotherapy and DFO monotherapy. In a randomized trial comparing DFO monotherapy, DFP monotherapy, and combination therapy with DFP + DFO, the change in LIC was not statistically significantly different between the different arms, suggesting that twice weekly administration of DFO in combination with DFP is a reasonable alternative regimen to continuous DFO monotherapy.Citation65 Lai et al demonstrated that in TDT patients with well-established cardiac disease, therapy with DFO + DFP is superior to DFO monotherapy.Citation66 In addition to advances in assessment of cardiac iron load, the new chelation regimes have been suggested to contribute significantly to the reduction in cardiac morbidity and mortality in patients with TDT.Citation67 For instance, switching from DFO to combination therapy with DFO + DFP was shown to prevent iron overload-related deaths.Citation68 Combination therapy with DFO + DFP has also been shown to have favorable effects on cardiac iron load as assessed by T2* MRI and left ventricular ejection fraction.Citation69,Citation70 Farmaki et al also showed that intensive combined chelation normalized thalassemic patients’ iron load, as assessed by cardiac T2* MRI, SF, and LIC.Citation71 This approach also prevented and reversed cardiac and multiple endocrine complications.Citation71 Therefore, the combination of DFP + DFO is one of the most helpful available means of decreasing cardiac siderosis. The combination should be used, whenever deemed possible, in patients with significant cardiac iron loading.Citation72
Alternating therapy with DFP (25 mg/kg three times daily for 5 days per week) + DFO has been suggested to be at least as effective as DFO monotherapy in controlling iron overload in patients with TDT.Citation73 Moreover, Abdelrazik showed that alternating DFP (75 mg/kg/day for 4 days per week) + DFO (40 mg/kg/day for 2 days per week) resulted in significant improvement in SF and urinary iron excretion as compared to DFO monotherapy.Citation74 A trial by Maggio et al showed that, compared with DFP (75 mg/kg/day) alone, alternating treatment with DFP (75 mg/kg/day for 4 days per week) + DFO (50 mg/kg/day day for 3 days per week) significantly decreased SF concentration during treatment for 5 years without significant differences in terms of survival, adverse events, and costs.Citation75 This study compared DFP alone at 75 mg/kg versus DFP at 75 mg/kg for 4 days per week and DFO by subcutaneous infusion (8–12 hours) at 50 mg/kg per day for the remaining 3 days per week.
Although the use of different scheduling regimens complicates comparisons among trials, a meta-analysis of LIC at the end of interventional studies favored combination therapy with DFP + DFO as compared to monotherapy with DFP.Citation76 Safety analyses demonstrated no adverse events with DFP + DFO significantly different than those associated with monotherapy with each of DFP and DFO.Citation76,Citation77
Combination of DFO and DFX
A gerbil animal model study failed to produce any noticeable effect of the combined therapy with DFO and DFX above DFX monotherapy in either the liver or heart. Although combined therapy was well tolerated, its efficacy could not be established due to limitations in the animal model.Citation78 In the clinical realm, in 2011, Voskaridou et al reported the first case of a patient with TDT successfully and safely treated with a combination of DFX and DFO.Citation79 A pilot study, involving 14 patients with TDT and significant iron overload, showed that LIC significantly and safely improved after a median follow-up of 29 weeks.Citation80 Grady et al used 34-day metabolic iron balance studies in six patients to evaluate monotherapy with DFX (30 mg/kg/day) versus monotherapy with DFO (40 mg/kg/day) versus combination therapy with DFX (30 mg/kg/day) and DFO (40 mg/kg/day).Citation81 They determined that supplementing the daily use of DFX with 2–3 days of DFO therapy would place all patients into net negative iron balance. Similarly, Lal et al ran a pilot clinical trial to evaluate the safety and efficacy of combined therapy with DFX (20–30 mg/kg/day) and DFO (35–50 mg/kg on 3–7 days/week) in 22 patients with persistent iron overload or organ damage.Citation82 In the 18 patients who completed the study, SF, LIC, and cardiac iron load significantly decreased proving that simultaneous administration of DFO and DFX rapidly reduced systemic and myocardial iron without increase in toxicity.Citation82 Cassinerio et al also studied the efficacy and safety of combined DFX and DFO in 10 TDT patients.Citation83 On 1-year follow-up, there was an improvement in LIC, SF, and cardiac T2* MRI, although results did not reach statistical significance. The Hyperion trial (NCT01254227) evaluated the efficacy and safety of the combination therapy with DFX + DFO, followed by monotherapy with DFX in patients with severe transfusional cardiac siderosis.Citation84 Despite a high attrition rate, the study showed that cardiac T2* improved during 12 months of treatment with DFX + DFO with side effect profiles comparable to adverse events encountered in monotherapy.Citation84
Combination and alternating therapy with DFP and DFX
Combined chelation with DFP and DFX has been the subject of several ongoing or completed unpublished studies.Citation85–Citation87 Cases of successful and safe use of this combination have been reported. Voskaridou et al successfully used a combination of 75 mg/kg/day of DFP with 30 mg/kg/day of DFX in a thalassemic woman with iron overload refractory to DFX monotherapy.Citation88 Combination therapy with DFX and DFP resulted in normalization of cardiac and liver T2* values with a considerable decrease in SF.
Alternating therapy with DFP and DFX has also been reported in two patients, who refused or had adverse effects with DFO, with improvement in LIC and SF.Citation89 More well-designed studies are needed to assess the efficacy and the safety of the combination of DFP and DFX.
Starting and adjusting chelation therapy: what do the guidelines say?
The guidelines governing ICT initiation and adjustment vary slightly depending on the panel of experts writing the recommendations. In our review, we discuss the guidelines from the following countries: Australia, Canada, Italy, the UK, and the US.Citation90–Citation95 We also discuss the recent guidelines issued by the Thalassaemia International Federation (TIF) in 2014.Citation96 The choice of the most appropriate chelation regimen depends on the iron burden, patient preference, the compliance to treatment, and toxicity of ICT. Multiple strategies based on SF, cardiac T2*, hepatic iron concentration, and transfusional iron burden have been suggested. All guidelines reviewed highlight the limitations of liver biopsy for assessment of hepatic liver concentration due to its invasiveness.Citation95 Therefore, as a non-invasive means to assess LIC, MRI remains a reliable tool in the diagnosis of hepatic iron load.Citation91–Citation96
Concerning the indication to initiate ICT, most guidelines agree that ICT should be started after the cumulative transfusion of 10–20 units of pRBC or when SF is greater than 1,000 ng/mL.Citation91,Citation92,Citation94,Citation96 However, the Canadian, Italian, and US guidelines add LIC as a criterion to initiate ICT recommending ICT when LIC exceeds 7 mg/g dw or the upper limit of normal.Citation90,Citation92,Citation93 summarizes the recommendations of the different guidelines for monitoring the efficacy of ICT.
Table 2 Monitoring ICT for efficacy
TIF guidelines
The most recent guidelines, published by TIF in 2014, recommend using DFO at a dose of 20–40 mg/kg/day five to seven times per week as a first line in children of age 2–6 years.Citation96 In the latter group of patients, DFX (20–40 mg/kg/day) may be used as first line in US and as second line in Europe when therapy with DFO is inadequate or contraindicated. The same recommendations apply for children older than 6 years and adults, except that the dose of DFO may reach 60 mg/kg/day. Moreover, in patients older than 6 years, DFP may be used at 75–100 mg/kg/day if other agents are not tolerated or effective. The TIF guidelines also recommend intensive 24-hour therapy with DFO (50–60 mg/kg/day) in case of a persistently high SF or LIC >15 mg/g dw. Significant heart disease may be treated by intensive DFO therapy or combination therapy with DFP + DFO.
Other guidelines
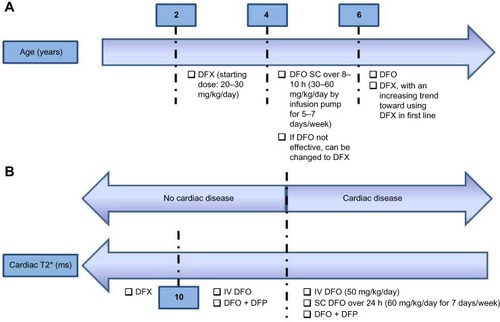
According to the Australian guidelines, initial therapy depends on the age of the patient.Citation94 Notably, in the context of cardiac dysfunction, the Australian guidelines recommend the use of intravenous or subcutaneous DFO or combination therapy with DFO + DFP. The recommendations are summarized in .
Figure 3 The figure summarizes the Australian practice guidelines in treating transfusional iron overload in TDT.
Abbreviations: TDT, transfusion-dependent thalassemia; DFX, deferasirox; DFO, deferoxamine; h, hour; DFP, deferiprone; SC, subcutaneously.
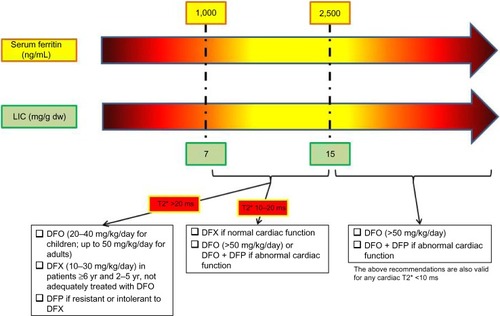
According to the Canadian guidelines, DFO, DFP, or DFX can be used at different doses depending on cardiac T2* if SF is between 1,000 ng/mL and 2,500 ng/mL or LIC is between 7 mg/d dw and 15 mg/d dw, in the absence of cardiac dysfunction.Citation93 However, DFO at doses > 50 mg/kg/day and combination therapy with DFO + DFP should be used if SF >2,500 ng/mL, LIC >15 mg/d dw, cardiac T2* <10 ms, or cardiac dysfunction is present. The recommendations are summarized in .
Figure 4 The figure summarizes the Canadian practice guidelines in treating transfusional iron overload in TDT.
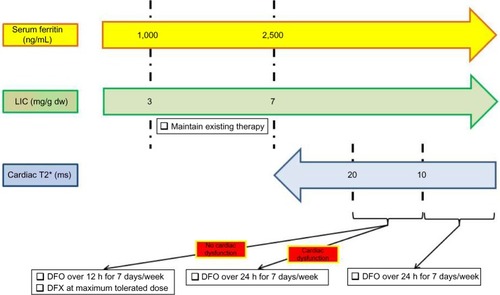
The US guidelines recommend maintaining existing ICT as long as LIC is between 3 mg/dw and 7 mg/dw and SF is between 1,000 ng/mL and 2,500 ng/mL.Citation92 They endorse the use of DFX at maximum tolerated dose or DFO administered over 12 hours daily if cardiac T2* is between 10 ms and 20 ms in the absence of cardiac dysfunction.Citation92 In the context of cardiac dysfunction or a cardiac T2* >10 ms, the US guidelines recommend the continuous use of DFO over 24 hours daily. The recommendations are summarized in .
Figure 5 The figure summarizes the US practice guidelines in treating transfusional iron overload in TDT.
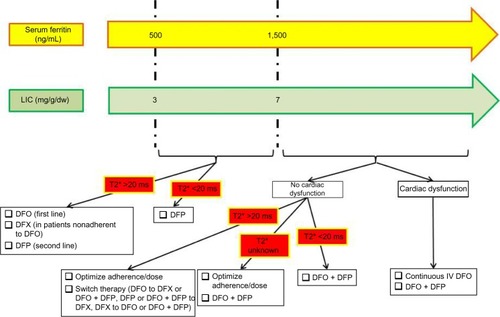
The UK guidelines recommend using DFP as the first-line therapy if cardiac T2* <20 ms, LIC is between 2 mg/g dw and 7 mg/g dw, and SF is between 500 ng/mL and 1,500 ng/mL.Citation91 DFO remains the recommended first-line treatment if cardiac T2* >20 ms, while DFX is reserved for patients non-adherent to DFO. DFP is used as a second-line agent in this context. The different treatment strategies when LIC >7 mg/g dw or SF >1,500 ng/mL are depicted in .
Figure 6 The figure summarizes the UK practice guidelines in treating transfusional iron overload in TDT.
The Italian guidelines recommend DFO for children younger than 6 years. For patients with severe iron overload, evidenced by a SF >3,000 ng/mL for 3 months, LIC >15 mg/g dw, cardiac T2* <12 ms, or cardiac dysfunction, intensive chelation with DFO or combination therapy with DFP + DFO is recommended.Citation90 Otherwise, for moderate iron overload, DFO remains the first-line agent, while DFX is used in patients with intolerance or non-compliance to DFO in the absence of severe iron overload. DFP is reserved for patients who are resistant or intolerant to DFX. Finally, the Italian guidelines recommend DFO for children younger than 6 years. For patients with severe iron overload, evidenced by a SF >3,000 ng/mL for 3 months, LIC >15 mg/g dw, cardiac T2* <12 ms, or cardiac dysfunction, intensive chelation with DFO or combination therapy with DFP + DFO is recommended.Citation90 Otherwise, for moderate iron overload, DFO remains the first-line agent, while DFX is used in patients with intolerance or non-compliance to DFO in the absence of severe iron overload. DFP is reserved for patients who are resistant or intolerant to DFX.
Future directions in treating iron overload
In 2000, Modell et al argued that about 50% of UK patients with β-thalassemia major die before the age of 35 years, mainly because conventional iron-chelation therapy is too burdensome for full adherence. Patients require an individually tailored treatment plan incorporating new, more tolerable approaches.Citation97 Advancing the treatment of transfusional iron overload includes not only pharmacologically improving iron chelators and tailoring chelation regimens through combining or alternating agents but also optimizing the treatment of the underlying disorder and, hence, decreasing the need for transfusions. An ideal iron chelator would have high iron chelating efficiency, high oral availability, tolerable profile of adverse events, once-daily dosing, palatable formulation, and high penetration into organs with iron deposition. Challenges in trial design in the realm of iron chelation include the small number of patients with conditions requiring chronic transfusions and the difficulty to recruit subjects to the parenteral arm in head-to-head trials involving DFO.
Innovation in chelation: improving the available chelators
Most attempts at improving drug administration, compliance, and palatability involve DFX. A single-arm study involving pediatric and adult patients with transfusional iron overload showed that additional administration options for DFX appeared to improve palatability ratings and GI tolerability.Citation43 Taking crushed DFX with soft food at breakfast time seemed to result in the highest palatability ratings.Citation43 A Phase II study (NCT02125877) investigating the benefits of a film-coated tablet of DFX, as opposed to a dispersible tablet, is currently ongoing and recruiting patients of age 10 years or older with TDT or MDS with resultant iron overload.Citation98 As for DFP, there have been studies on the pharmacokinetic profiles of a single dose of a sustained-release formulation without any published data.Citation99,Citation100
Innovation in chelation: a novel agent
A novel oral iron chelator SP-420, which showed efficacy in models of iron overload, has been associated with reduced renal toxicity in exploratory studies.Citation101–Citation103 It is currently being studied in a Phase Ib trial.Citation104 Other clinical studies involving the oral chelator FBS0701, a member of the desazadesferrithiocin class, have been terminated despite the completion of initial pharmacokinetic and pharmacodynamic studies.Citation105
Hitting a step earlier: decreasing transfusional iron burden
Decreasing the need or the frequency of blood transfusions is one way of addressing the issue of iron overload. Agents that might be promising to decrease the transfusional requirements include those that target ineffective hematopoiesis, such as JAK2 inhibitors, and those that appear to limit the overproduction of immature erythroid cells in thalassemia patients, potentially reversing extra-medullary hematopoiesis and preventing splenectomy and sotatercept (ACE-011) that appear to function by blocking the activity of certain TGF-β family cytokines involved in late stages of erythropoiesis, eventually leading to an increase in hemoglobin production in these patients.Citation106,Citation107
As a conclusion, it is imperative that, as new evidence becomes available from ongoing research on novel agents and as more experience is gained from the use of the available iron chelators, clinical practice guidelines, being evidence-based, should be updated to suit the clinical goals of care in TDT.
Disclosure
Antoine N Saliba and Afif Harb have no conflicts of interest to declare. Ali Taher receives research funding and honoraria from Novartis Pharmaceuticals.
References
- PietrangeloAPhysiology of iron transport and the hemochromatosis geneAm J Physiol Gastrointest Liver Physiol20022823G403G41411841990
- KnutsonMWessling-ResnickMIron metabolism in the reticuloendothelial systemCrit Rev Biochem Mol Biol2003381618812641343
- HoffbrandAVTaherACappelliniMDHow I treat transfusional iron overloadBlood2012120183657366922919029
- FilletGBeguinYBaldelliLModel of reticuloendothelial iron metabolism in humans: abnormal behavior in idiopathic hemochromatosis and in inflammationBlood19897428448512502204
- BreuerWHershkoCCabantchikZIThe importance of non-transferrin bound iron in disorders of iron metabolismTransfus Sci200023318519211099894
- NemethETuttleMSPowelsonJHepcidin regulates cellular iron efflux by binding to ferroportin and inducing its internalizationScience200430657042090209315514116
- NemethEIron regulation and erythropoiesisCurr Opin Hematol200815316917518391780
- TannoTPorayettePSripichaiOIdentification of TWSG1 as a second novel erythroid regulator of hepcidin expression in murine and human cellsBlood2009114118118619414861
- TannoTBhanuNVOnealPAHigh levels of GDF15 in thalassemia suppress expression of the iron regulatory protein hepcidinNat Med20071391096110117721544
- TannoTRabelALeeYTYauYYLeitmanSFMillerJLExpression of growth differentiation factor 15 is not elevated in individuals with iron deficiency secondary to volunteer blood donationTransfusion20105071532153520210929
- CasanovasGVujić SpasicMCasuCThe murine growth differentiation factor 15 is not essential for systemic iron homeostasis in phlebotomized miceHaematologica201398344444722983584
- KautzLJungGValoreEVRivellaSNemethEGanzTIdentification of erythroferrone as an erythroid regulator of iron metabolismNat Genet201446767868424880340
- NovartisDesferal (Deferoxamine Mesylate) Prescribing InformationSwitzerlandNovartis Pharmaceuticals2011
- PorterJBAbeysingheRDMarshallLHiderRCSinghSKinetics of removal and reappearance of non-transferrin-bound plasma iron with deferoxamine therapyBlood19968827057138695819
- BarryMFlynnDMLetskyEARisdonRALong-term chelation therapy in thalassaemia major: effect on liver iron concentration, liver histology, and clinical progressBr Med J19742590916204821036
- ModellBLetskyEAFlynnDMPetoRWeatherallDJSurvival and desferrioxamine in thalassaemia majorBr Med J19822846322108110846802413
- Borgna-PignattiCRugolottoSDe StefanoPSurvival and complications in patients with thalassemia major treated with transfusion and deferoxamineHaematologica200489101187119315477202
- BrittenhamGMGriffithPMNienhuisAWEfficacy of deferoxamine in preventing complications of iron overload in patients with thalassemia majorN Engl J Med199433195675738047080
- AndersonLJWestwoodMAHoldenSMyocardial iron clearance during reversal of siderotic cardiomyopathy with intravenous desferrioxamine: a prospective study using T2* cardiovascular magnetic resonanceBr J Haematol2004127334835515491298
- DavisBAPorterJBLong-term outcome of continuous 24-hour deferoxamine infusion via indwelling intravenous catheters in high-risk beta-thalassemiaBlood20009541229123610666195
- CohenAMartinMMizaninJKonkleDFSchwartzEVision and hearing during deferoxamine therapyJ Pediatr19901172 pt 13263302380834
- OlivieriNFBuncicJRChewEVisual and auditory neurotoxicity in patients receiving subcutaneous deferoxamine infusionsN Engl J Med1986314148698733485251
- CohenARGalanelloRPennellDJCunninghamMJVichinskyEThalassemiaHematology Am Soc Hematol Educ Program20041143415561674
- DeleaTEEdelsbergJSofryginOConsequences and costs of noncompliance with iron chelation therapy in patients with transfusion-dependent thalassemia: a literature reviewTransfusion200747101919192917880620
- AgencyEMFerriprox: EPAR – Product Information2009 Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000236/WC500022050.pdf2014
- TraynorKDeferiprone approved for iron overloadAm J Health Syst Pharm201168222106
- Borgna-PignattiCCappelliniMDDe StefanoPCardiac morbidity and mortality in deferoxamine-or deferiprone-treated patients with thalassemia majorBlood200610793733373716373663
- PigaAGagliotiCFogliaccoETrictaFComparative effects of deferiprone and deferoxamine on survival and cardiac disease in patients with thalassemia major: a retrospective analysisHaematologica200388548949612745268
- AddisALoebsteinRKorenGEinarsonTRMeta-analytic review of the clinical effectiveness of oral deferiprone (L1)Eur J Clin Pharmacol19995511610206077
- MaggioAD’AmicoGMorabitoADeferiprone versus deferoxamine in patients with thalassemia major: a randomized clinical trialBlood Cells Mol Dis200228219620812064916
- TaherASheikh-TahaMShararaASafety and effectiveness of 100 mg/kg/day deferiprone in patients with thalassemia major: a two-year studyActa Haematol2005114314614916227677
- AndersonLJWonkeBPrescottEHoldenSWalkerJMPennellDJComparison of effects of oral deferiprone and subcutaneous desferrioxamine on myocardial iron concentrations and ventricular function in beta-thalassaemiaLancet2002360933251652012241655
- PennellDJBerdoukasVKaragiorgaMRandomized controlled trial of deferiprone or deferoxamine in beta-thalassemia major patients with asymptomatic myocardial siderosisBlood200610793738374416352815
- BerdoukasVChouliarasGMoraitisPZannikosKBerdoussiELadisVThe efficacy of iron chelator regimes in reducing cardiac and hepatic iron in patients with thalassaemia major: a clinical observational studyJ Cardiov Magn Reson20091120
- PennellDJCarpenterJPRoughtonMCabantchikZOn improvement in ejection fraction with iron chelation in thalassemia major and the risk of future heart failureJ Cardiov Magn Reson20111345
- MaggioAVitranoACapraMImproving survival with deferiprone treatment in patients with thalassemia major: a prospective multicenter randomised clinical trial under the auspices of the Italian Society for Thalassemia and HemoglobinopathiesBlood Cells Mol Dis200942324725119233692
- CohenARGalanelloRPigaADe SanctisVTrictaFSafety and effectiveness of long-term therapy with the oral iron chelator deferiproneBlood200310251583158712763939
- OlivieriNFBrittenhamGMMcLarenCELong-term safety and effectiveness of iron-chelation therapy with deferiprone for thalassemia majorN Engl J Med199833974174239700174
- WuSFPengCTWuKHTsaiCHLiver fibrosis and iron levels during long-term deferiprone treatment of thalassemia major patientsHemoglobin200630221521816798646
- WanlessIRSweeneyGDhillonAPLack of progressive hepatic fibrosis during long-term therapy with deferiprone in subjects with transfusion-dependent beta-thalassemiaBlood200210051566156912176871
- TaherAAounEShararaAIFive-year trial of deferiprone chelation therapy in thalassaemia major patientsActa Haematol2004112417918315564727
- Exjade (deferasirox)prescribing informationSwitzerlandNovartis Pharmaceuticals2005
- GoldbergSLGiardinaPJChirnomasDEspositoJPaleyCVichinskyEThe palatability and tolerability of deferasirox taken with different beverages or foodsPediatr Blood Cancer20136091507151223637051
- SéchaudRDutreixCBalezSRelative bioavailability of deferasirox tablets administered without dispersion and dispersed in various drinksInt J Clin Pharmacol Ther200846210210818218291
- PigaAGalanelloRForniGLRandomized phase II trial of deferasirox (Exjade, ICL670), a once-daily, orally-administered iron chelator, in comparison to deferoxamine in thalassemia patients with transfusional iron overloadHaematologica200691787388016818273
- GalanelloRPigaAForniGLPhase II clinical evaluation of deferasirox, a once-daily oral chelating agent, in pediatric patients with beta-thalassemia majorHaematologica200691101343135117018383
- CappelliniMDCohenAPigaAA phase 3 study of deferasirox (ICL670), a once-daily oral iron chelator, in patients with beta-thalassemiaBlood200610793455346216352812
- PorterJGalanelloRSaglioGRelative response of patients with myelodysplastic syndromes and other transfusion-dependent anaemias to deferasirox (ICL670): a 1-yr prospective studyEur J Haematol200880216817618028431
- TaherAEl-BeshlawyAElalfyMSEfficacy and safety of deferasirox, an oral iron chelator, in heavily iron-overloaded patients with beta-thalassaemia: the ESCALATOR studyEur J Haematol200982645846519187278
- TaherACappelliniMDVichinskyEEfficacy and safety of deferasirox doses of >30 mg/kg per d in patients with transfusion-dependent anaemia and iron overloadBr J Haematol2009147575275919764988
- DeugnierYTurlinBRopertMImprovement in liver pathology of patients with beta-thalassemia treated with deferasirox for at least 3 yearsGastroenterology20111414120212111211. e1201120321741344
- CappelliniMDPorterJEl-BeshlawyAEPIC Study InvestigatorsTailoring iron chelation by iron intake and serum ferritin: the prospective EPIC study of deferasirox in 1744 patients with transfusion-dependent anemiasHaematologica201095455756619951979
- PorterJBElalfyMSTaherATEfficacy and safety of deferasirox at low and high iron burdens: results from the EPIC magnetic resonance imaging substudyAnn Hematol201392221121923086508
- PennellDJPorterJBCappelliniMDDeferasirox for up to 3 years leads to continued improvement of myocardial T2* in patients with beta-thalassemia majorHaematologica201297684284822271905
- PennellDJPorterJBPigaACORDELIA study investigatorsA 1-year randomized controlled trial of deferasirox vs deferoxamine for myocardial iron removal in beta-thalassemia major (CORDELIA)Blood2014123101447145424385534
- WonkeBWrightCHoffbrandAVCombined therapy with deferiprone and desferrioxamineBr J Haematol199810323613649827905
- BreuerWErmersMJPootrakulPAbramovAHershkoCCabantchikZIDesferrioxamine-chelatable iron, a component of serum non-transferrin-bound iron, used for assessing chelation therapyBlood200197379279811157499
- LinkGKonijnAMBreuerWCabantchikZIHershkoCExploring the “iron shuttle” hypothesis in chelation therapy: effects of combined deferoxamine and deferiprone treatment in hypertransfused rats with labeled iron stores and in iron-loaded rat heart cells in cultureJ Lab Clin Med2001138213013811477380
- EvansPKayyaliRHiderRCEcclestonJPorterJBMechanisms for the shuttling of plasma non-transferrin-bound iron (NTBI) onto deferoxamine by deferiproneTrans Res201015625567
- PennellDJUdelsonJEAraiAEAmerican Heart Association Committee on Heart Failure and Transplantation of the Council on Clinical Cardiology and Council on Cardiovascular Radiology and ImagingCardiovascular function and treatment in beta-thalassemia major: a consensus statement from the American Heart AssociationCirculation2013128328130823775258
- MouradFHHoffbrandAVSheikh-TahaMKoussaSKhoriatyAITaherAComparison between desferrioxamine and combined therapy with desferrioxamine and deferiprone in iron overloaded thalassaemia patientsBr J Haematol2003121118718912670352
- GomberSSaxenaRMadanNComparative efficacy of desferrioxamine, deferiprone and in combination on iron chelation in thalassemic childrenIndian Pediatr2004411212714767084
- HaSYChikKWLingSCA randomized controlled study evaluating the safety and efficacy of deferiprone treatment in thalassemia major patients from Hong KongHemoglobin200630226327416798652
- AydinokYUlgerZNartDA randomized controlled 1-year study of daily deferiprone plus twice weekly desferrioxamine compared with daily deferiprone monotherapy in patients with thalassemia majorHaematologica200792121599160618055982
- El-BeshlawyAManzCNajaMIron chelation in thalassemia: combined or monotherapy? The Egyptian experienceAnn Hematol200887754555018351337
- LaiMEGradyRWVacquerSIncreased survival and reversion of iron-induced cardiac disease in patients with thalassemia major receiving intensive combined chelation therapy as compared to deferoxamine aloneBlood Cells Mol Dis201045213613920678715
- LadisVChouliarasGBerdoukasVRelation of chelation regimes to cardiac mortality and morbidity in patients with thalassaemia major: an observational study from a large Greek UnitEur J Haematol201085433534420561034
- TelferPTWarburtonFChristouSImproved survival in thalassemia major patients on switching from desferrioxamine to combined chelation therapy with desferrioxamine and deferiproneHaematologica200994121777177819815834
- TannerMAGalanelloRDessiCA randomized, placebo-controlled, double-blind trial of the effect of combined therapy with deferoxamine and deferiprone on myocardial iron in thalassemia major using cardiovascular magnetic resonanceCirculation2007115141876188417372174
- TannerMAGalanelloRDessiCCombined chelation therapy in thalassemia major for the treatment of severe myocardial siderosis with left ventricular dysfunctionJ Cardiov Magn Reson20081012
- FarmakiKTzoumariIPappaCChouliarasGBerdoukasVNormalisation of total body iron load with very intensive combined chelation reverses cardiac and endocrine complications of thalassaemia majorBr J Haematol2010148346647519912219
- KwiatkowskiJLReal-world use of iron chelatorsHematology Am Soc Hematol Educ Program2011201145145822160073
- GalanelloRKattamisAPigaAA prospective randomized controlled trial on the safety and efficacy of alternating deferoxamine and deferiprone in the treatment of iron overload in patients with thalassemiaHaematologica20069191241124316956824
- AbdelrazikNPattern of iron chelation therapy in Egyptian beta thalassemic patients: Mansoura University Children’s Hospital experienceHematology200712657758517852442
- MaggioAVitranoACapraMLong-term sequential deferiprone-deferoxamine versus deferiprone alone for thalassaemia major patients: a randomized clinical trialBr J Haematol2009145224525419236376
- MaggioAFilosaAVitranoAIron chelation therapy in thalassemia major: a systematic review with meta-analyses of 1520 patients included on randomized clinical trialsBlood Cells Mol Dis201147316617521843958
- FisherSABrunskillSJDoreeCGoodingSChowdhuryORobertsDJDesferrioxamine mesylate for managing transfusional iron overload in people with transfusion-dependent thalassaemiaThe Cochrane Database of Syst Rev20138Cd004450
- Otto-DuesselMBrewerCGonzalezINickHWoodJCSafety and efficacy of combined chelation therapy with deferasirox and deferoxamine in a gerbil model of iron overloadActa Haematol2008120212312819018129
- VoskaridouEKomninakaVKaravasATerposEAkianidisVChristoulasDCombination therapy of deferasirox and deferoxamine shows significant improvements in markers of iron overload in a patient with beta-thalassemia major and severe iron burdenTransfusion201454364664923834310
- LalASweetersNHerzMSafety of combined chelation therapy with deferasirox and deferoxamine in transfusion-dependent thalassemia [Abstract]Blood20091142021
- GradyRWGalanelloRRandolphREKleinertDADessiCGiardinaPJToward optimizing the use of deferasirox: potential benefits of combined use with deferoxamineHaematologica201398112913522875626
- LalAPorterJSweetersNCombined chelation therapy with deferasirox and deferoxamine in thalassemiaBlood Cells Mol Dis20135029910423151373
- CassinerioEOrofinoNRoghiACombination of deferasirox and deferoxamine in clinical practice: an alternative scheme of chelation in thalassemia major patientsBlood Cells Mol Dis201453316416724846580
- AydinokYKattamisACappelliniMDDeferasirox– deferoxamine combination therapy reduces cardiac iron with rapid liver iron Removal in patients with severe transfusional iron overload (HYPERION)55th ASH annual meetingDecember 8, 2013New Orleans, LA
- Combination Deferasirox and Deferiprone for Severe Iron Overload in Thalassemia2015 Available from: https://clinicaltrials.gov/ct2/show/NCT01709032?term=Deferiprone+AND+deferasirox&rank=12015
- Study of Efficacy, Safety of Combined Deferasirox and Deferiprone Versus Combined Deferiprone and Desferal In Conditions of Iron Overload2015 Available from: https://clinicaltrials.gov/ct2/show/NCT01511848?term=Deferiprone+AND+deferasirox&rank=3Accessed 2015
- Clinical Trial of Deferasirox Combination Treatment with Deferiprone in Thalassaemia Patients2015 Available from: https://clinicaltrials.gov/ct2/show/NCT02198508?term=Deferiprone+AND+deferasirox&rank=42015
- VoskaridouEChristoulasDTerposESuccessful chelation therapy with the combination of deferasirox and deferiprone in a patient with thalassaemia major and persisting severe iron overload after single-agent chelation therapiesBr J Haematol2011154565465621615376
- BaloccoMCarraraPPintoVForniGLDaily alternating deferasirox and deferiprone therapy for “hard-to-chelate” beta-thalassemia major patientsAm J Hematol201085646046120513129
- AngelucciEBarosiGCamaschellaCItalian Society of Hematology practice guidelines for the management of iron overload in thalassemia major and related disordersHaematologica200893574175218413891
- YardumianATelferPDarbyshirePStandards for the Clinical Care of Children and Adults with Thalassaemia in the UK2nd ed2008 Available from:http://www.hbpinfo.com/ukts-standards-2008.pdf2015
- VichinskyELevineLStandard-of-Care Clinical Practice Guidelines2012 Available from: http://thalassemia.com/treatment-guidelines-5.aspx#gsc.tab=02015
- SayaniFWarnerMWuJWong-RiegerDHumphreysKOdameIGuidelines for the Clinical Care of Patients with Thalassemia in CanadaNicosia, CyprusThalassaemia International Federation2009
- HoPJTayLLindemanRCatleyLBowdenDKAustralian guidelines for the assessment of iron overload and iron chelation in transfusion-dependent thalassaemia major, sickle cell disease and other congenital anaemiasIntern Med J201141751652421615659
- MusallamKMAngastiniotisMEleftheriouAPorterJBCross-talk between available guidelines for the management of patients with beta-thalassemia majorActa Haematol20131302647323485589
- CappelliniMDCohenAPorterJTaherAViprakasitVGuidelines for the Management of Transfusion Dependent Thalassemia3rd edNicosia, CyprusThalassaemia International Federation2014
- ModellBKhanMDarlisonMSurvival in beta-thalassaemia major in the UK: data from the UK Thalassaemia RegisterLancet200035592202051205210885361
- Phase II Study to Investigate the Benefits of an Improved Deferasirox Formulation (Film-coated Tablet2015 Available from: https://clini-caltrials.gov/ct2/show/study/NCT02125877?term=Deferasirox&rank=302015
- Pilot Study of the Pharmacokinetic Profile of a Single Dose of Deferiprone Sustained-Release Formulation in Healthy Volunteers2015 Available from: https://clinicaltrials.gov/ct2/show/NCT02189941?term=deferiprone&rank=5Accessed 2015
- Absorption, Metabolism, and Excretion of a Single Dose of Ferriprox® in Patients With Sickle Cell Disease2015 Available from: https://clinicaltrials.gov/ct2/show/study/NCT01835496?term=deferiprone&rank=9Accessed Jan 2015
- BergeronRJWiegandJMcManisJSBhartiNSinghSDesign, synthesis, and testing of non-nephrotoxic desazadesferrithiocin polyether analoguesJ Med Chem200851133913392318533709
- BergeronRJWiegandJBhartiNMcManisJSSinghSDesferrithiocin analogue iron chelators: iron clearing efficiency, tissue distribution, and renal toxicityBiometals201124223925821103911
- BergeronRJBhartiNWiegandJMcManisJSSinghSAbboudKAThe impact of polyether chain length on the iron clearing efficiency and physiochemical properties of desferrithiocin analoguesJ Med Chem20105372843285320232803
- Safety and Pharmacokinetic Study of Escalating Doses of SP-420, an Iron Chelator, in Patients with β-Thalassemia2015 Available from: https://clinicaltrials.gov/ct2/show/record/NCT02274233?term=sp+420&rank=1
- RienhoffHYJrViprakasitVTayLA phase 1 dose-escalation study: safety, tolerability, and pharmacokinetics of FBS0701, a novel oral iron chelator for the treatment of transfusional iron overloadHaematologica201196452152521173101
- SuraganiRNCawleySMLiRModified activin receptor IIB ligand trap mitigates ineffective erythropoiesis and disease complications in murine beta-thalassemiaBlood2014123253864387224795345
- DussiotMMacielTTFricotAAn activin receptor IIA ligand trap corrects ineffective erythropoiesis in beta-thalassemiaNat Med201420439840724658077